A
A pattern See pattern, A.
abathic distance See plane, apparent frontoparallel.
Abbé’s condenser See condenser, Abbé’s.
Abbé’s condition See sin condition.
Abbé’s number See constringence.
Abbé’s refractometer See refractometer.
abducens muscle See muscle, lateral rectus.
abducens nerve See nerve, abducens.
abducens nerve palsy See paralysis of the sixth nerve.
abduct To turn away from the midline, as when the eye rotates outward.
abduction Outward rotation of an eye, that is away from the midline.
See duction; syndrome, Duane’s.
abductors Extraocular muscles that move the eye outward, such as the lateral rectus, the inferior oblique and the superior oblique.
aberrant regeneration An abnormal regeneration process following paralysis or paresis of the fibres of the third cranial nerve (oculomotor) in which the upper lid fails to follow the eye on downward gaze or even retracts on downward gaze or adduction, with occasional contraction of the pupil. Syn. pseudo-von Graefe sign.
aberration An optical defect in which the rays from a point object do not form a perfect point after passing through an optical system.
See astigmatism, oblique; coma; curvature of field; distortion.
axial chromatic a. See aberration, longitudinal chromatic.
lateral chromatic a. Defect of an optical system (eye, lens, prism, etc.) in which the size of the image of a point object is extended by a coloured fringe, due to the unequal refraction of different wavelengths (dispersion). Syn. chromatic difference of magnification; transverse chromatic aberration (TCA).
See dispersion; doublet.
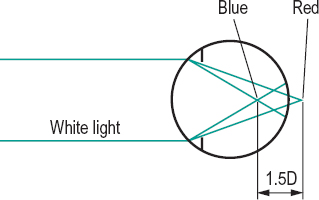
longitudinal chromatic a. (LCA) Defect of an optical system (eye, lens, prism, etc.) due to the unequal refraction of different wavelengths (dispersion) which results in an extended image along the optical axis. In the eye, blue rays are focused in front of the retina (by about 1 D) and red rays slightly behind the retina (0.25–0.5 D) when relaxed. When the eye is accommodated for a near target, blue rays tend to be focused near the retina and red rays are focused behind the retina (1 D), because of a lag of accommodation usually occurring when viewing near targets (Fig. A1). Syn. axial chromatic aberration.
See chromoretinoscopy; chromostereopsis; constringence; dispersion; doublet; lens, achromatizing; pigment, macular; test, duochrome.
monochromatic a. Defect of an optical system (eye, lens, prism, etc.) occurring for a single wavelength of light. There are five such aberrations: spherical aberration, coma, curvature of field, oblique astigmatism and distortion. Syn. Seidel aberration.
negative a. See aberration, spherical.
oblique a . Aberration induced by a point object off the optical axis of the system. These comprise coma, curvature of field, distortion and oblique astigmatism.
positive a. See aberration, spherical.
prism a . Additional effects of a prism on light, in addition to the expected change in direction of light. These effects include different magnifications, curvature of field and chromatic aberration.
Seidel a. See aberration, monochromatic.
spherical a . Defect of an optical system due to a variation in the focusing between peripheral and paraxial rays. The larger the pupil size, the greater the difference in focusing between the two rays. In the gaussian theory, the focus of the optical system is attributed to the paraxial rays. The distance, in dioptres, between the focus of the paraxial rays and the peripheral rays represents the amount of longitudinal spherical aberration of the system. When the peripheral rays are refracted more than the paraxial rays, the aberration is said to be positive or undercorrected. When the peripheral rays are refracted less than the paraxial rays the aberration is said to be negative or overcorrected. The relaxed human eye has a small amount of positive spherical aberration (up to 1 D for a pupil of 8 mm diameter) (Fig. A2).
See caustic; lens, aplanatic; theory, gaussian.
transverse chromatic a. See aberration, lateral chromatic.
wavefront a . The amount of deviation between an output wavefront emanating from an optical system and a conceptualized ideal (reference) wavefront. The specification of the deviation (or error) is usually fitted with a normalized Zernike expansion. The measurement of this aberration can be done subjectively or objectively (e.g. with an aberrometer based on the Hartmann–Shack principle). The method (called aberrometry) has been applied clinically to measure the aberrations displayed by optical systems, such as the eye, the eye with a correction, contact lenses (in vitro or in situ), intraocular lenses (in vitro or in situ), in corneal refractive surgery, cataract, etc. (Fig. A3). Syn. wavefront error.
aberrometry See aberration, wavefront.
aberroscope Instrument for observing aberration. Such an instrument was designed by Tscherning to measure his own spherical aberration. It consists of a planoconvex lens with a grid made up of squares ruled on its plane surface.
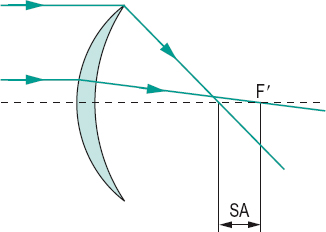
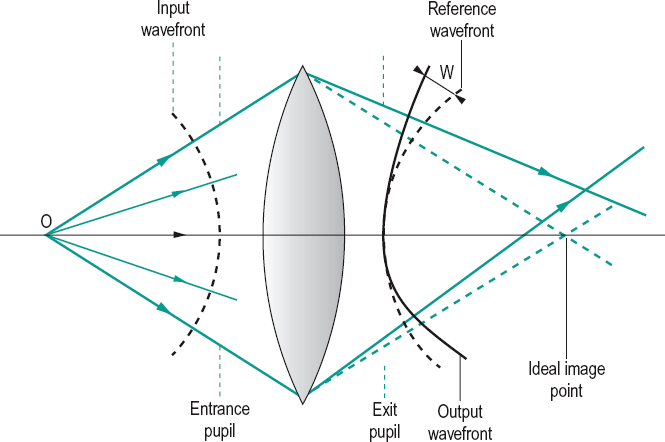
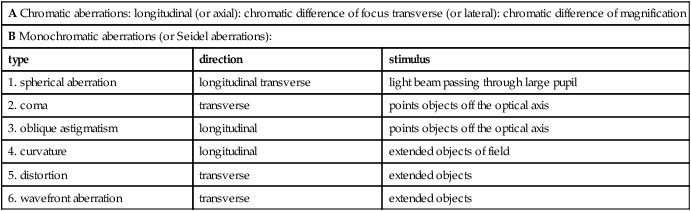
Table A1
Aberrations of the eye
| A Chromatic aberrations: longitudinal (or axial): chromatic difference of focus transverse (or lateral): chromatic difference of magnification | ||
| B Monochromatic aberrations (or Seidel aberrations): | ||
| type | direction | stimulus |
| 1. spherical aberration | longitudinal transverse | light beam passing through large pupil |
| 2. coma | transverse | points objects off the optical axis |
| 3. oblique astigmatism | longitudinal | points objects off the optical axis |
| 4. curvature | longitudinal | extended objects of field |
| 5. distortion | transverse | extended objects |
| 6. wavefront aberration | transverse | extended objects |
abetalipoproteinaemia See syndrome, Bassen–Kornzweig.
ablatio retinae See retinal detachment.
ablation A procedure in which a tissue or body part is removed or destroyed by surgery, radiation or photocoagulation. Example: LASIK.
ablepharon See ablephary.
ablephary Congenital absence, complete or partial, of the eyelids. Syn. ablepharon.
ablepsia See blindness.
ablepsy See blindness.
Abney’s law; phenomenon See under the nouns.
abnormal (anomalous) retinal correspondence See retinal correspondence, abnormal.
abrasion, corneal See corneal abrasion.
abrasive Granular substance used in lens grinding, such as corundum (aluminium oxide), carborundum, etc.
See roughing; smoothing; surfacing.
abscess An accumulation of pus located in infected tissue.
absorbance A measure of absorption equal to the logarithm to the base 10 of the reciprocal of the transmittance T, for a specified wavelength and expressed as A = –log10 T. Syn. optical density.
See density, optical; transmittance.
absorption Transformation of radiant energy into a different form of energy, usually heat, as it passes through a medium. Light that is absorbed is neither transmitted nor reflected. It may, however, be re-emitted as light of another wavelength as, for example, ultraviolet radiation is converted into visible radiation on absorption by a luminescent material. A substance that absorbs all radiations is called a black body.
See absorbance; density, optical; fluorescence.
absorptive lens See lens, absorptive.
AC/A ratio Ratio of the accommodative convergence AC (in prism dioptres) to the stimulus to accommodation A (in dioptres). The most common method of determining this ratio is by the gradient method (or gradient test) in which the phoria at near is measured after changing the accommodation with a spherical lens (usually +1.00 D or –1.00 D) placed in front of the two eyes. It is expressed as

where α is the phoria at near, and α’ is the phoria at the same distance but through a lens of power F. The deviation is measured in prism dioptres, with + for esodeviation and – for exodeviation. Example: if the initial phoria is 4 Δ exo and 8 Δ exo when a lens of +1.00 D is placed in front of the eyes, the AC/A ratio is equal to

The average AC/A ratio is about 4 in young adults and tends to decline slightly with age. The gradient is not affected by proximal convergence, as the target distance and size are relatively constant. Syn. gradient. Another method of determining the AC/A ratio (often called the heterophoria method) compares the phoria measured at distance and at near. It is expressed as

where PD is the interpupillary distance in cm, N the deviation at near, D the deviation at distance and K the near fixation distance in dioptres. Example: A patient has a PD of 70 mm, a distance phoria of 4 Δ eso and a near phoria of 8 Δ exo at 33.3 cm from the eyes, the AC/A ratio is equal to

See convergence, accommodative; convergence, proximal; dioptre, prism.
acanthamoeba keratitis See keratitis, acanthamoeba.
acanthocytosis See syndrome, Bassen–Kornzweig.
acanthosis nigricans A rare skin disorder presenting numerous superficial, pigmented papillomatous growths on various parts of the body. Ocular manifestations are primarily papillomatous lesions of the lid margins, which may be so extensive as to cause punctal occlusion, as well as papillary conjunctivitis. Syn. keratosis nigricans.
accessory lacrimal glands See glands, accessory lacrimal; glands of Krause; glands of Wolfring.
accommodation Adjustment of the dioptric power of the eye. It is generally involuntary and made to see objects clearly at any distance. In man (and primates), this adjustment is brought about by a change in the shape of the crystalline lens. In some animals this adjustment occurs either as a result of an anteroposterior movement of the crystalline lens, or of an alteration in the curvature of the cornea.
See aniso-accommodation; muscle, ciliary; reflex, accommodative; theory, Fincham’s; theory, Helmholtz’s of accommodation.
amplitude of a. The maximum amount of accommodation A that the eye can exert. It is expressed in dioptres, as the difference between the far point and the near point measured with respect either to the spectacle plane or the corneal apex or some other reference point. Thus,

where B is the near point vergence and K is the far point vergence. A is always positive. In the emmetropic eye, A = – B, because the far point is at infinity and K = 0. So, if the near point of an emmetrope is at 25 cm from the spectacle plane, the amplitude of accommodation is equal to – [–1/(25 × 10–2)] = 4 D. The amplitude of accommodation declines from about 14 D at age 10 to about 0.5 D at age 60 (although the measured value is usually higher due to the depth of focus of the eye).
See method, minus lens; method, push-up.
astigmatic a. Postulated unequal accommodation along different meridians of the eye attributed to a differential action of the ciliary muscle which would lead to a difference in the curvature of the surfaces of the crystalline lens along different meridians. Syn. meridional accommodation.
Table A2
Mean amplitude of accommodation as a function of age, in Caucasians (the plane of reference is the spectacle plane)
| age (years) | Duane (N = 2000 subjects, push-up method) | Turner (Nh = 500 subjects, push-out method) |
| 10 | 13.5 | 13.0 |
| 15 | 12.5 | 10.6 |
| 20 | 11.5 | 9.5 |
| 25 | 10.5 | 7.9 |
| 30 | 8.9 | 6.6 |
| 35 | 7.3 | 5.75 |
| 40 | 5.9 | 4.4 |
| 45 | 3.7 | 2.5 |
| 50 | 2.0 | 1.6 |
| 55 | 1.3 | 1.1 |
| 60 | 1.2 | 0.7 |
| 65 | 1.1 | 0.6 |
| 70 | 1.0 | 0.6 |
closed-loop a. Accommodation response to visual stimuli in normal viewing conditions.
See accommodation, open-loop.
components of a . The process of accommodation is assumed to involve four components: reflex, vergence (convergence), proximal and tonic accommodation (also called resting state of accommodation).
See accommodation, convergence; accommodation, proximal; accommodation, reflex; accommodation, resting state of.
consensual a. Accommodation occurring in one eye when the other eye has received the dioptric stimulus.
convergence a. 1. Accommodation induced directly by a change in convergence. 2. That component of accommodation induced by the binocular disparity of the retinal images. Syn. vergence accommodation.
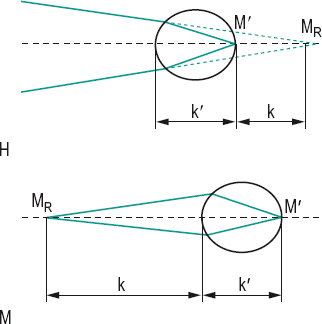
correction induced a. Ocular accommodation induced when changing from spectacles to contact lenses in near vision. Spectacles induce less accommodation in myopes and more accommodation in hyperopes than that exerted by an emmetrope fixating at a given distance. Contact lenses do not induce any different accommodation than that required for a given distance. Consequently, myopes require more accommodation and hyperopes less accommodation when they transfer from spectacles to contact lenses. However, this change in accommodative demand is accompanied by a similar change in convergence, so that a myope transferring to contact lenses accommodates and converges more than with spectacles and the reverse applies for a hyperope.
See convergence, correction induced.
far point of a. A point in space conjugate with the retina (more specifically the foveola) when the accommodation is relaxed. In emmetropia, the far point is at infinity; in myopia, it is at a finite distance in front of the eye; in hyperopia, it is a virtual point behind the eye (Fig. A4). Syn. far point of the eye; punctum remotum.
ill-sustained a. See accommodative insufficiency.
inert a. See accommodative infacility.
insufficiency of a. See accommodative insufficiency.
lag of a. 1. The amount by which the accommodative response of the eye is less than the dioptric stimulus to accommodation, as usually occurs when fixating an object at near. It could be due to uncorrected hyperopia or indicate accommodative insufficiency. Absence of an accommodative lag may indicate latent hyperopia. Syn. lazy lag of accommodation. 2. The condition occurring in dynamic retinoscopy in which the neutral point is situated further from the eyes than is the retinoscopic target.
lead of a. The amount by which the accommodative response of the eye is greater than the dioptric stimulus to accommodation, as occurs when fixating at distance, in a few individuals. It can also occur as a result of a spasm of accommodation.
mechanism of a . Process by which the eye focuses onto an object. It does so by contracting the ciliary muscle which releases the tension on the zonular fibres, allowing the elastic lens capsule to increase its curvature, especially that of the front surface. Along with these changes are an increase in the thickness of the lens, a decrease in its equatorial diameter and a reduction in pupil size. The ciliary muscle is controlled by the parasympathetic system, which is triggered by an out of focus retinal image.
See accommodation, convergence; accommodation, proximal; accommodative response; muscle, ciliary; reflex, near.
meridional a. See accommodation, astigmatic.
microfluctuations of a. Involuntary variations in the contraction of the intraocular muscles responsible for accommodation and resulting in changes of about 0.1–0.5 D with a frequency of 0.5–2.5 Hz.
near point of a. The nearest point in space that is conjugate with the foveola when exerting the maximum accommodative effort. Syn. punctum proximum.
See method, push-up; rule, near point; sphere, near point; test, Scheiner’s.
negative a. 1. A relaxation of accommodation below the apparent zero level or when shifting from near to distance vision. 2. See accommodation, relative amplitude of.
objective a . Accommodation measured without the subject’s judgment. This is accomplished by dynamic retinoscopy, by autorefractors or by visually evoked cortical potentials. The term is sometimes used incorrectly to refer to the amplitude of accommodation without the influence of the depth of focus (e.g. as measured by stigmatoscopy).
See accommodation, subjective; optometer; potential, evoked cortical; retinoscopy, dynamic; stigmatoscopy.
ocular a. The amplitude of accommodation referred to the front surface of the cornea. Symbol: A.
See accommodation, spectacle.
open-loop a . Accommodative response occurring without the usual stimulus to accommodation, such as a blurred retinal image. In these conditions, the accommodative system of the eye tends to return to its position of rest
Table A3
Relationship between viewing distance and spectacle and ocular accommodation of a contact lens wearer and of four corrected hyperopes (with thin spectacle lenses). The vertex distance was 14 mm and ocular accommodation was calculated using the formula A = K – B. The ocular accommodation exerted by a contact lens wearer is the same for all refractive errors and equal to that of an emmetrope
| distance from spectacle lens (cm) | spectacle accom. (D) | ocular accom. (D) of contact lens wearer | ocular accom. (D) of hyperopes | |||
| +2 | +4 | +6 | +8 | |||
| 100 | 1.00 | 0.99 | 1.04 | 1.11 | 1.17 | 1.25 |
| 67 | 1.49 | 1.46 | 1.55 | 1.64 | 1.74 | 1.86 |
| 50 | 2.00 | 1.95 | 2.06 | 2.18 | 2.31 | 2.46 |
| 40 | 2.50 | 2.42 | 2.55 | 2.71 | 2.87 | 3.05 |
| 33 | 3.03 | 2.91 | 3.07 | 3.25 | 3.45 | 3.67 |
| 25 | 4.00 | 3.79 | 4.00 | 4.24 | 4.49 | 4.77 |
| 20 | 5.00 | 4.67 | 4.94 | 5.22 | 5.54 | 5.88 |
| 16 | 6.25 | 5.75 | 6.07 | 6.42 | 6.80 | 7.22 |
| 14 | 7.14 | 6.49 | 6.86 | 7.25 | 7.68 | 8.14 |
| 12 | 8.33 | 7.46 | 7.88 | 8.32 | 8.81 | 9.34 |
| 10 | 10.00 | 8.77 | 9.25 | 9.77 | 10.34 | 10.95 |
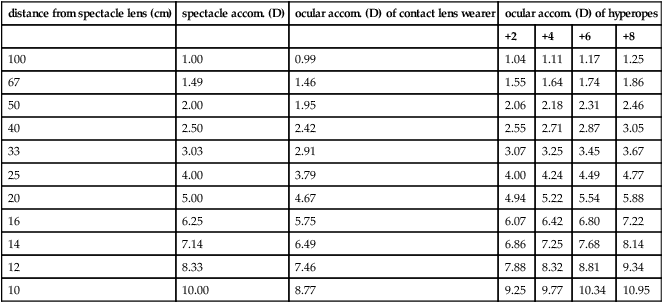
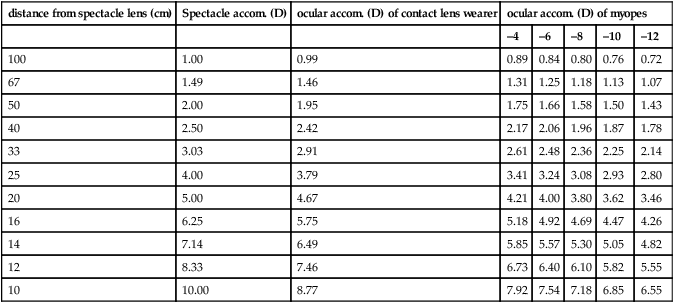
Table A4
Relationship between viewing distance and spectacle and ocular accommodation of a contact lens wearer and of five corrected myopes (with thin spectacle lenses). The vertex distance was 14 mm and ocular accommodation was calculated using the formula A = K – B. The ocular accommodation exerted by a contact lens wearer is the same for all refractive errors and equal to that of an emmetrope
| distance from spectacle lens (cm) | Spectacle accom. (D) | ocular accom. (D) of contact lens wearer | ocular accom. (D) of myopes | ||||
| –4 | –6 | –8 | –10 | –12 | |||
| 100 | 1.00 | 0.99 | 0.89 | 0.84 | 0.80 | 0.76 | 0.72 |
| 67 | 1.49 | 1.46 | 1.31 | 1.25 | 1.18 | 1.13 | 1.07 |
| 50 | 2.00 | 1.95 | 1.75 | 1.66 | 1.58 | 1.50 | 1.43 |
| 40 | 2.50 | 2.42 | 2.17 | 2.06 | 1.96 | 1.87 | 1.78 |
| 33 | 3.03 | 2.91 | 2.61 | 2.48 | 2.36 | 2.25 | 2.14 |
| 25 | 4.00 | 3.79 | 3.41 | 3.24 | 3.08 | 2.93 | 2.80 |
| 20 | 5.00 | 4.67 | 4.21 | 4.00 | 3.80 | 3.62 | 3.46 |
| 16 | 6.25 | 5.75 | 5.18 | 4.92 | 4.69 | 4.47 | 4.26 |
| 14 | 7.14 | 6.49 | 5.85 | 5.57 | 5.30 | 5.05 | 4.82 |
| 12 | 8.33 | 7.46 | 6.73 | 6.40 | 6.10 | 5.82 | 5.55 |
| 10 | 10.00 | 8.77 | 7.92 | 7.54 | 7.18 | 6.85 | 6.55 |
(or tonic accommodation). Examples: looking at an empty field; looking through a very small artificial pupil (0.5 mm or less).
See accommodation, closed-loop.
paralysis of a. Total or partial loss of accommodation due to paralysis of the ciliary muscle.
positive a. Normal accommodation that occurs when looking from a distant to a near object.
proximal a. That component of accommodation initiated by the awareness of a near object. Syn. psychic accommodation.
See accommodation, components of; accommodation, resting state of.
psychic a. See accommodation, proximal.
range of a. The linear distance between the far point and the near point. Part of the range of accommodation is virtual in the case of the hypermetrope.
reflex a. An adjustment of the refractive state of the eye stimulated by blur and aimed at reducing blur. It may be initiated when the eye changes fixation from far to near, or it may be induced by convergence. The amount of reflex accommodation rarely exceeds 2 D.
See accommodation, components of; reflex, near.
relative amplitude of a. The total amount of accommodation which the eye can exert while the convergence of the eyes is fixed. It can be positive (using concave lenses until the image blurs). This is called positive relative accommodation (PRA). It can be negative (using convex lenses until the image blurs). This is negative relative accommodation (NRA).
See zone of clear, single, binocular vision.
reserve a. See addition, near.
resting state of a. The passive state of accommodation of the eye in the absence of a stimulus, i.e. when the eye is either in complete darkness, or looking at a bright empty field. In this condition, the prepresbyopic eye is usually focused at an intermediate point (about 80 cm on average, although there are large variations), that is, the emmetropic eye becomes myopic. This is presumably due to a balance between a parasympathetic innervation to the circular fibres of the ciliary muscle and a sympathetic innervation to the longitudinal fibres of the ciliary muscle. Thus, the resting state of accommodation would correspond to a position of equilibrium between the two systems. Accommodation from this state to the near point of accommodation would be the response to parasympathetic stimulation; and accommodation from this state to the far point of accommodation would be the response to sympathetic stimulation. Syn. dark accommodation; dark focus (these terms are not strictly synonymous but as they have been found to correlate well, they have been adopted as synonyms); tonic accommodation (TA).
See hysteresis, accommodative; myopia, night; myopia, space; tonus; vergence, tonic.
spasm of a. Involuntary contraction of the ciliary muscle producing excess accommodation. It may be constant, intermittent, unilateral or bilateral. Patients typically complain of blurred distance vision and sometimes changes in perceived size of objects, and discomfort. If the patient is a low hyperope or emmetrope, it will give rise to pseudomyopia (false myopia, hypertonic myopia, spurious myopia). Diagnosis is facilitated by cycloplegic refraction to rule out latent hyperopia. Although spasm of accommodation can be a separate entity, it is often associated with excessive convergence (esotropia) and miosis; this is referred to as spasm of the near reflex. Management includes removal of the primary cause, if possible (e.g. uveitis, or patient taking parasympathomimetic drugs), correction of the underlying refraction, if any, changes in the visual working conditions, positive lenses, accommodative facility exercises and, only rarely, cycloplegics.
See accommodative facility; metamorphopsia.
spectacle a. The amplitude of accommodation referred to the spectacle plane. Symbol: As.
See accommodation, ocular.
subjective a. Measurement of the accommodation based on the subject’s judgements, such as the push-up or push-out method or the minus lens method.
See accommodation, objective; method, minus lens; method, push-up.
tonic a. See accommodation, resting state of.
vergence a. See accommodation, convergence.
accommodative Relating to accommodation.
accommodative astigmatism See astigmatism, accommodative.
accommodative convergence See convergence, accommodative.
accommodative convergence/accommodation ratio See AC/A ratio.
accommodative excess A condition in which the subject exerts more accommodation than required for the visual stimulus, or is unable to relax accommodation. It may be due to uncorrected hyperopia, very prolonged near work, emotional problems, spasm of accommodation, uveitis, trigeminal neuralgia, syphilis, meningitis, head trauma, or the side effect of some pharmaceutical agent (e.g. a miotic drug). It is usually associated with convergence excess. The subject reports blurred vision at distance, asthenopia and often headaches. Treatment commonly includes plus lenses and facility exercises, besides therapy of the underlying cause. Syn. hyperaccommodation. Note: spasm of accommodation is one aspect of the general condition of accommodative excess, although some authors consider this term a synonym.
See accommodation, spasm of; accommodative facility; convergence excess.
accommodative demand See accommodation, correction induced.
accommodative esotropia See strabismus, accommodative.
accommodative facility Ability of the eye/s to focus on stimuli at various distances and in different sequences in a given period of time. Clinically, this is measured either monocularly or binocularly, usually by having the subject fixate a small target alternately through plus and minus lenses, which are interchanged as soon as the target appears clear. The operation is repeated many times and the results are commonly presented in cycles per minute (one cycle indicates that both plus and minus lenses have been cleared). Syn. accommodative rock.
See accommodative insufficiency; lens flippers.
accommodative fatigue See accommodative insufficiency.
accommodative inertia Difficulty in altering the accommodative response, such that the latency and completion time of the process are delayed. It may occur as a result of prolonged near vision tasks. Orthoptic exercises may help in this condition.
accommodative hysteresis See hysteresis, accommodative.
accommodative infacility A condition in which there is a slowness in changing from one level of accommodation to another. Patients may complain of transitory blur. It may be due to diabetes, Graves’ disease, measles or the side effects of some drugs. It is commonly associated with asthenopia. Treatment is aimed at the primary cause, but plus lenses and, especially, accommodative facility exercises are usually prescribed. Syn. inert accommodation.
accommodative insufficiency Insufficient amplitude of accommodation that is unequivocally below the appropriate level for the age. It may be due to extreme fatigue, influenza, high stress, systemic medication, ocular inflammation, head trauma, thyroid disease or the juvenile form of diabetes mellitus. The condition is often associated with convergence insufficiency, general fatigue, measles, multiple sclerosis, or myotonic dystrophy, etc. It is the most common accommodative dysfunction. Patients complain of blurred vision, or difficulty in sustaining clear vision at near; this is often accompanied by a frontal headache and even sometimes by pain in the eye. A mild form of accommodative insufficiency is often referred to as ill-sustained accommodation (accommodative fatigue) in which the response may be initially normal but cannot be maintained. It is easily discovered with accommodative facility exercises. Ill-sustained accommodation may be a precursor of accommodative insufficiency. Treatment is aimed at the primary cause, but plus lens correction, and in some cases exercises such as accommodative facility training are prescribed. Syn. premature presbyopia.
See convergence insufficiency; headache, ocular; ophthalmopathy, thyroid.
accommodative reflex See accommodation, reflex.
accommodative response The response of the accommodative system when the eye changes fixation from one point in space to another. The reaction time for the accommodative response is about 370 ms. Clinically it can be estimated by measuring the accommodative lag or accommodative lead.
See accommodation, mechanism of; effect, Mandelbaum.
accommodative rock See accommodative facility.
accommodometer Instrument used to measure accommodation such as the near point rule.
acetazolamide See carbonic anhydrase inhibitors.
acetone Liquid ketone (dimethyl ketone and propanone) used as a solvent for many organic compounds (e.g. cellulose acetate) and for repairing spectacle frames.
acetylcholine (ACh) A neurotransmitter substance with special excitatory properties of all preganglionic autonomic neurons, all parasympathetic postganglionic neurons and a few postganglionic sympathetic neurons. Acetylcholine is synthesized and liberated by the action of the enzyme choline acetyl-tranferase from the compounds choline and acetyl coenzyme A (acetyl CoA) which occurs in all cholinergic neurons. ACh exists only momentarily after its formation, being hydrolysed by the enzyme acetylcholinesterase which is present in the neurons of cholinergic nerves throughout their entire lengths and at neuromuscular junctions: this process is essential for proper muscle function as otherwise the accumulation of ACh would result in continuous stimulation of the muscles, glands and central nervous system. Alternatively a shortage of ACh has devastating effect (e.g. myasthenia gravis). ACh binds to acetylcholine receptors on skeletal muscle fibres. Sodium enters the muscle fibre membrane, which leads to a depolarization of the membrane and muscle contraction. There are two main types of acetylcholine receptors (cholinergic receptors): muscarinic receptors, which are stimulated by muscarine and ACh, belong to a family of G proteins coupled receptors and are situated in parasympathetically innervated structures (e.g. the iris and ciliary body); and nicotine receptors, which are stimulated by nicotine and ACh, are ligand-gated receptors and are situated in striated muscles (e.g. the extraocular muscles). Cholinergic receptors are found in the sympathetic and parasympathetic nervous systems, in the brain and spinal cord. The action of ACh can be either blocked or stimulated by drugs: Anticholinesterase drugs (e.g. neostigmine) inhibit acetylcholinesterase and prolong the action of acetylcholine whereas antimuscarinic drugs (also referred to as anticholinergics or parasympatholytics) such as atropine, cyclopentolate, homatropine, hyoscine and tropicamide inhibit the action of acetylcholine at muscarinic receptors. Other drugs mimic the action of ACh, they are known as parasympathomimetics (e.g. pilocarpine).
See cholinergic; cycloplegia; miotics; mydriatic; neurotransmitter; nicotine; synapse; system, autonomic nervous.
acetylcholinesterase An enzyme that degrades and inactivates acetylcholine. This compound is mainly found in neurons and at neuromuscular junctions. Drugs that inhibit this enzyme (e.g. diisopropyl fluorophosphate, physostigmine, edrophonium, echothiophate, DFP) can be used in the diagnosis and possible treatment of myasthenia gravis as well as certain forms of esotropia and glaucoma. Syn. specific cholinesterase.
acetylcysteine See tears, artificial.
achromasia See achromatopsia.
achromat See lens, achromatic.
achromatic 1. See lens, achromatic. 2. The condition of being totally colour blind.
See achromatopsia; light, white; spectrum, equal energy.
achromatic axis; colour; interval; lens See under the nouns.
achromatic light stimulus, specified Any specified illuminant capable of being accepted as white under usual conditions of observation. Note: This includes the CIE standard illuminants (CIE).
achromatic prism See prism, achromatic.
achromatism 1 . The condition of being totally colour blind. Syn. achromatopsia. 2. Absence of colour. 3. Condition of a lens or an optical system corrected for, or free from, chromatic aberration.
See monochromat.
achromatizing lens See lens, achromatizing.
achromatopsia Total colour blindness. The majority of cases are autosomal recessively inherited and caused by a mutation in genes CNGA3, CNGB3 and CNAT2. There are two types of achromatopsia. Complete achromatopsia which results from having only rods and no functional cones (rod monochromat) have photophobia, poor acuity and nystagmus. Incomplete achromatopsia in which there are the same symptoms, but in a diminished form. Patients benefit from dark tinted lenses. Achromatopsia is non-progressive and very rare: one person in about 35 000 people. A few cases may be acquired resulting from a lesion in cortical area V4 (central achromatopsia). Syn. achromasia; achromatic vision; achromatism; acritochromacy; monochromatism.
See colour vision, defective; hemiachromatopsia; monochromat.
achromic Colourless.
aciclovir See antiviral agents.
acinar cell
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


