Incisional Refractive Techniques: Radial Keratotomy, Astigmatic Keratotomy, and Limbal Relaxing Incisions
CHAPTER CONTENTS
General Preoperative Considerations
General Surgical Considerations
General Postoperative Considerations
Radial keratotomy (RK) and astigmatic keratotomy (AK) were the first refractive procedures to be practiced on a wide scale in North America. Although photorefractive RK and laser in situ keratomileusis have largely replaced these two procedures, they are still effective for low myopia and astigmatism and are occasionally used by refractive surgeons. Most of the concepts now used for refractive surgery were developed originally for RK and AK.
GENERAL PREOPERATIVE CONSIDERATIONS
Indications
- low to moderate myopia and/or astigmatism
- realistic patient expectations of surgical effect
- patient age greater than 21 years
Patient Evaluation
- documented medical history (see list of contraindications on pages 69–70)
- family history (especially of keratoconus or rheumatoid arthritis)
- measurement of distance and near uncorrected visual acuity (for statistical documentation, postoperative patient comparison, and legal considerations)
- manifest refraction and, ideally, cycloplegic refraction [after discontinuation of rigid gas-permeable (RGP) contact lens wear for 3 weeks and soft contact lens (SCL) wear for 3 days]
- evaluate for potential problems using corneal topography (e.g., keratoconus, irregular astigmatism, and contact lens warpage)
- Retest every 2 to 3 weeks until stable using corneal topography, after discontinuing contact lens wear (also helps determine the meridian and zone for arcuate and tangential incisions)
- slit-lamp examination (rules out any preexisting corneal disease)
- dilated fundus examination (rules out any macular or peripheral retinal disease)
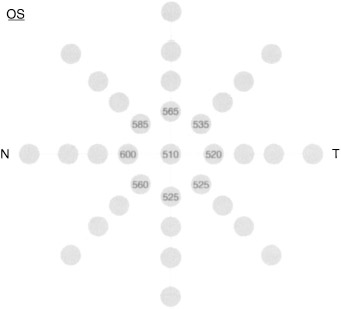
- serial pachymetry at the corneal apex and at eight paracentral meridia (from superotemporal to superior) to determine the thinnest paracentral zone [Be alert for serial readings differing more than 75 μm (Fig. 8-1).]
- tonometry [establishes preoperative baseline intraocular pressure (IOP); increased IOP may result in greater than expected refractive results]
- determination of ocular dominance (see Chapter 5)
- patient education
- one-on-one conferences
- educational brochures
- videos
- ample opportunity for patient questions (and answers from knowledgeable personnel)
- one-on-one conferences
- informed consent read by patient in its entirety and signed in ink; personally reviewed by surgeon with the patient and signed in the patient’s presence by surgeon
Patient Preparation
- Administer broad-spectrum antibiotics for prophylaxis approximately 25 minutes before surgery.
- Instill 1% pilocarpine.
- ensures maximum patient focus intraoperatively with high illumination
- better defines patient’s visual axis
- ensures maximum patient focus intraoperatively with high illumination
- Apply topical anesthetic but not directly to the corneal epithelium [recommended regime: 1 gtt of 4% lidocaine (Xylocaine; Abbott) every 10 minutes (×2), followed by 1 gtt of 0.5% tetracaine every 10 minutes (X2)].
- Administer up to 20 mg of diazepam 20 minutes before surgery (acts as an anxiolytic and relaxes the muscles of the eye to make the lid speculum more comfortable).
GENERAL SURGICAL CONSIDERATIONS
Relative Contraindications
- tendency toward aggressive wound healing due to potential minimized effect and a greater potential for future hyperopic drift
- collagen vascular disease [propensity for stromal melt (keratolysis) following the procedure]
- active infectious or inflammatory ocular conditions (e.g., blepharoconjunctivitis or ocular rosacea, which should be fully controlled before surgery)
- collagen vascular disease [propensity for stromal melt (keratolysis) following the procedure]
Absolute Contraindications
- unrealistic patient expectations of perfect vision or improved best corrected visual acuity (BCVA)
- patient age less than 21 years
- systemic disease (e.g., diabetes mellitus because of possible poor healing of corneal incisions)
- recent unstable refraction greater than 0.5 D sphere or cylinder (within the previous 24 months)
- keratoconus because of progressive ectasia
- corneal warpage from contact lens wear or large, chronic eyelid masses like chalazia (discontinue lens wear and topographically document stable curvature before surgery)
- pre-existing irregular astigmatism
- severe retinopathy
- increased risk for severely compromised acuity in the future
- possible adverse effects on low contrast acuity from increased depth of focus
- increased risk for severely compromised acuity in the future
- severe dry eye (keratoconjunctivitis sicca)
- increased risk for keratolysis
- greatly prolonged visual recovery
- increased risk for keratolysis
- history of chronic herpes simplex or zoster keratitis because of the. increased risk for keratolysis (ideally should not be considered for surgery)
Equipment
- a user-friendly computerized topographer
- an operating microscope (with certain features)
- a para-axial illumination source
- an infrared filter (prevents corneal desiccation)
- an ultraviolet filter (eliminates retinal phototoxicity)
- a coaxial fixation target
- a para-axial illumination source
- durable optical zone (OZ) and radial markers machined from a single sheet of titanium (without soldered cross hairs or gold plating)
- a corneal pachymeter (with certain features)
- a solid-state probe
- continuous readout
- contact activation
- a display monitor
- enough memory for multiple readings
- a solid-state probe
- a combined-style diamond knife (with certain features)
- a 45-degree-angle head
- 80 to 120 μm thick
- retractable for safe handling
- universal design footplates
- a high quality diamond blade (Fig. 8-2)
- a 45-degree-angle head
- a computer-programmable diamond knife with computer-driven motor (allows the pachymeter to communicate with the diamond to reduce microperforations and improve topographic profiles; now superceded by the excimer laser)
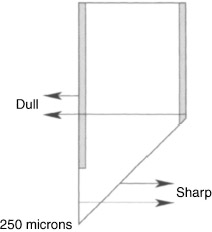
Figure 8–2 Diagram of a combined-style diamond knife.
Methods
- Position the patient comfortably on the operating table with a folded towel or foam pillow under the neck to facilitate the chin-up position required for placement of superior incisions.
- Patch the nonsurgical eye.
- A trained, gloved, and masked technician may administer periocular povidone iodine solution (Betadine).
- Wipe away excess solution.
- Position the open, sterile eye drape over the patient’s face.
- Immediately before beginning the actual procedure, instill 1 final drop of 0.5% tetracaine into the conjunctiva.
- Position a lid speculum to allow adequate ocular exposure and avoid undue eyelid tension.
- Use one of the three methods that follow to mark the exact center of the pupil (i.e., the visual axis).
- Use the miotic pupil centering method.
- Instill a miotic agent, such as 1% pilocarpine.
- Mark the exact center of the pupil (miotic pupil centering).
- Instill a miotic agent, such as 1% pilocarpine.
- Use the light filament reflex method (recommended by the PERK Study Group).
- Physically mark the midpoint along the lower margin of the reflex on the cornea while the patient fixates on the microscope light filament.
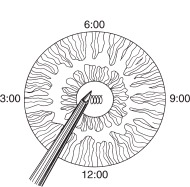
- Look through one ocular and mark along the opposite inferior border of the light filament reflex [e.g., if you fixate through the left ocular, the mark should be positioned along the lower right border of the filament reflex on the cornea (Fig. 8-3)].
- Physically mark the midpoint along the lower margin of the reflex on the cornea while the patient fixates on the microscope light filament.
- Use the coaxial light source method.
- This method allows the patient to fixate on a less intense light during the procedure than does the light filament reflex method and is more precise.
- Coaxially mount a fixation light source between the patient and the surgeon within the operating microscope optical system.
- This method allows the patient to fixate on a less intense light during the procedure than does the light filament reflex method and is more precise.
- Mark the visual axis as follows.
- When the lid speculum is in place, administer 1 drop of balanced salt solution (BSS) over the corneal apex to enhance the corneal light reflex.
- Use a Sinskey hook to carefully indent the epithelium overlying the visual axis.
- Mark the axis carefully because any deep epithelial defect can leave scarring in the visual axis.
- When the epithelial indentation is not easily visible, use a Week cell sponge to dry the central epithelium and enhance visualization.
- Clear excess pooling in the canthal region with a Week cell sponge (a dry field is important for detection of early microperforation).
- Avoid excessive dryness to decrease friction between knife footplates and corneal epithelium.
- When the lid speculum is in place, administer 1 drop of balanced salt solution (BSS) over the corneal apex to enhance the corneal light reflex.
- Identify and mark the OZ.
- Align the cross hairs of the OZ marker with the visual axis epithelial marking.
- Apply proper pressure to the OZ marker to avoid misalignment. (Misalignment commonly occurs when the visual axis does not coincide with the corneal apex and when slippage occurs across the epithelium because of improper pressure.)
- Use a Week cell sponge to gently dry the epithelium and enhance markings (as with all pressure-induced markings, moisture may cause the indentations to become faint).
- Ensure proper globe centration (improper centration contributes to decentration of the OZ marking).
- Use a Week cell sponge to gently dry the epithelium and enhance markings (as with all pressure-induced markings, moisture may cause the indentations to become faint).
- Align the cross hairs of the OZ marker with the visual axis epithelial marking.
- Perform corneal pachymetry.
- Soak the probe tip in hydrogen peroxide.
- Dry the tip with an alcohol wipe.
- Allow the tip to air dry.
- Position the probe tip exactly perpendicular to the epithelium at 1.5 mm temporal to the visual axis and at the thinnest paracentral point (determined by preoperative pachymetery screening).
- If pachymetry readings do not register, ensure that the probe tip is exactly perpendicular with the corneal epithelium or moisten the epithelium with a micro-drop of BSS.
- Usually the thinnest paracentral site corresponds with the paracentral temporal site, but if these two sites differ in thickness, set the diamond blade to 100% of the thinner of the two (use a calibrating microscope to set the blade).
- When the range of paracentral screening values (from thickest to thinnest) is greater than 75 μm, expect less refractive change than predicted by the nomogram, and lengthen the incisions slightly toward the limbus or reduce the recommended optical zone by 0.25 mm.
- Soak the probe tip in hydrogen peroxide.
- Calibrate and adjust the diamond knife.
- Sterilize and mount the diamond knife into the sterile mounting block of the calibrating microscope at the beginning of each procedure.
- Zero the knife footplates and either extend the diamond to 550 μm or set it to correspond with the thinnest paracentral screening pachymetery reading.
- After obtaining real-time intraoperative pachymetry readings, adjust the diamond tip accordingly.
- Make the final setting of the diamond knife blade 100% of the thinnest intraoperative pachymetery reading.
- Sterilize and mount the diamond knife into the sterile mounting block of the calibrating microscope at the beginning of each procedure.
- If consistent undercorrections result but without microperforations or incisions approaching the pre-Descemet’s region, set the diamond blade to a longer setting (in 10-μm or 2% increments) for subsequent incisional procedures on other patients.
- If consistent undercorrections occur with deep incisions or incisions that extend within 1 mm of the limbus, decrease the OZ diameter by 0.25 mm.
GENERAL POSTOPERATIVE CONSIDERATIONS
Medications
- 1 drop neomycin/poly/dexamethasone (Maxitrol); 1 drop diclofenac sodium (Voltaren; Cibavison), 1 drop aminoglycoside, or 1 drop fluoroquinolone
- 1 drop Voltaren every 6 hours as needed for pain (first evening only)
- 1 drop Maxitrol every 6 hours for 5 days and then every 12 hours for 2 days only (same schedule for aminoglycoside or fluoroquinolone, which may be taken several minutes after Maxitrol)
- 2 oxycodone/acetaminophen (Percocet) tabs every 6 hours for immediate postoperative pain (optional)
Patient Instructions
- Provide written instructions to the patient.
- Instruct patient to go home and sleep for several hours and to take the drops as directed (see above).
- Instruct patient not to rub his or her eyes.
- Instruct patient not to use eye make-up for 2 weeks.
- Instruct patient to avoid contaminated water (e.g., pools, hot tubs, showers) for 2 weeks.
- Instruct patient to refrain from reading for the first day after surgery.
- Instruct patient to call emergency telephone numbers if experiencing severe pain, discharge, increased redness, or swelling.
- Inform patient about first follow-up visit.
Follow-Up
- first postoperative visit (day 2)
- Measure uncorrected acuity.
- Perform a slit-lamp examination.
- Measure uncorrected acuity.
- subsequent postoperative visits (weeks 1, 3, and 6 and months 3, 6, and 12)
- Schedule for late afternoon for corneal stability.
- Measure uncorrected visual acuity.
- Measure manifest refraction.
- Measure BCVA.
- Perform slit-lamp examination.
- Review patient progress and symptoms.
- Schedule for late afternoon for corneal stability.
Enhancements
- nonsurgical
- Nonsurgical intervention is possible if the degree of myopia is within 0.5 D of target.
- Begin with pressure patching (preferred) beginning at 1 week and continuing for 6 weeks only at night or continuously both day and night.
- Nonsurgical intervention is possible if the degree of myopia is within 0.5 D of target.
- surgical
- Surgery is required if residual myopia is greater than 0.5 D.
- Provide additional incisions (cumulative total, ≤ 8) if the undercorrection is greater than 1.25 D, the OZ is a minimum of 2.75 mm, the limbal zone is a minimum of 0.5 mm, and there are fewer than eight original incisions.
- Lengthen existing incisions by decreasing the limbal clear zone or by decreasing the optical clear zone (if the undercorrection is 0.50-1.25 D, the OZ is >2.75 mm, the limbal zone is >0.5 mm, and there is significant astigmatism and eight original incisions).
- Deepen some or all of the existing incisions if they appear to be shallow at the slit lamp, the OZ is at the minimum, and there are at least eight original incisions.
- Surgery is required if residual myopia is greater than 0.5 D.
RADIAL KERATOTOMY
Preoperative Considerations
Indications
- particularly effective for up to –4 D of myopia
- increasingly effective with increasing age
- best to aim for slight undercorrection to compensate for the progressive hyperopic shift documented with RK (0.1 D/year)
Surgical Considerations
Methods
- Center radial markings to the optical zone marker (based on the nomogram) and place in contact with the corneal epithelium with moderate pressure for several seconds.
- Perform radial incisions.
- Because the cornea thins progressively during the procedure, incise the thinnest corneal quadrant first and the thickest quadrant last (thinnest to thickest) to minimize perforation risk.
- For an ideal incision, terminate the incision 1 mm inside the limbus at a constant depth within 85% to 90% of stromal depth throughout the length of the cut.
- The central extent of the incision should slightly undermine the OZ.
- Square off the base of the incision and extend it centrally beyond the surface OZ margin (Fig. 8-4).
- Achieving ideal incision characteristics minimizes the risks of fibrovascular ingrowth into incisions and undercorrections.
- The central extent of the incision should slightly undermine the OZ.
- Because the cornea thins progressively during the procedure, incise the thinnest corneal quadrant first and the thickest quadrant last (thinnest to thickest) to minimize perforation risk.
- Use the combined (genesis) technique.
- The centripetal (Russian) incision begins at the limbus and progresses toward the OZ [provides reliably deeper incisions than does the centrifugal (American) incision (Fig. 8-5)].
- The centrifugal (American) incision begins at the optical zone and progresses toward the limbus [safer than the Russian incision because it rarely invades the central clear zone (Fig. 8-6)].
- The diamond knife design for this combined technique allows for both centripetal and centrifugal incisions to be performed with the same blade because of its vector force-sensitive design. The knife cuts along the entire centrifugal (angled) margin and along the distal 250 μm of the centripetal (vertical) margin (see Fig. 8-2).
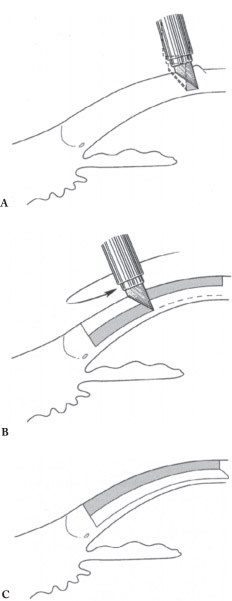
- First perform the centrifugal incision, beginning at the optical zone and ending 1 mm inside the limbus (Fig. 8-7A) (results in an inconsistently deep but relatively shallow “safety” groove of inconsistent depth that helps to guide the centripetal incision.).
- At the termination of the first (centrifugal) incision, keep the blade in the groove.
- Reverse the motion to begin the centripetal incision toward the optical zone. [This second incision deepens and evens out the groove (Fig. 8-7B). During the second incision, it is nearly impossible to veer outside of the first groove or to incise beyond the initiation of the first incision into the optical zone. The uphill centripetal incision also ensures uniform depth and a slight undermining of the optical zone for maximal effect (Fig. 8-7C).]
- The centripetal (Russian) incision begins at the limbus and progresses toward the OZ [provides reliably deeper incisions than does the centrifugal (American) incision (Fig. 8-5)].
- Use the ideal combined technique.
- Insert the combined-style diamond blade (tip points posterocentrally) at the OZ margin slightly oblique to the corneal surface.
- Apply pressure while penetrating posterocentrally and pause for 1 second.
- Gently undermine the OZ.
- Reorient the diamond blade perpendicular to the corneal epithelium.
- Initiate the centrifugal incision directed toward the limbus.
- Terminate the centrifugal incision 1 mm short of the limbus.
- Return toward the OZ with centripetal motion within the groove.
- Gently undermine the OZ again.
- Remove the diamond blade from the groove by pulling away from OZ.
- Control microtremors.
- Use both hands on diamond knife (when using guarded diamond for RK).
- Use a wrist rest.
- Rest hands on the patient’s face.
- Relax your shoulders and exhale slowly.
- Use a mild Valsalva maneuver.
- Unless contraindicated, self-administer beta blocker drops 10 minutes before the procedure.
- Insert the combined-style diamond blade (tip points posterocentrally) at the OZ margin slightly oblique to the corneal surface.
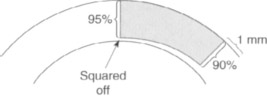
Figure 8-4 Diagram of the base of a radial incision being squared off.
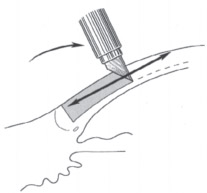
Figure 8-5 Diagram of a centripetal (Russian)

Figure 8-6 Diagram of a centrifugal (American) incision.
Intraoperative Complications
- invasion of incisions into the optical zone (caused by inaccurate visual axis marking or spontaneous patient eye movement and may lead to several postoperative complications); to avoid, ensure proper globe centration when marking visual axis and avoid parallax errors and use the combined (genesis) technique (see pages 74–75) to minimize risk for eye movement.
- increased glare
- irregular astigmatism
- monocular diplopia (possible)
- increased glare
- incisions extending into the limbus (caused by incising beyond clear cornea)
- intersecting incisions
- wound gape
- poor healing
- If either occurs, reapproximate the wound edges with 10-0 or 11-0 nylon sutures left in place for 10 to 12 weeks.
- wound gape
- corneal perforation (more easily recognized in a relatively dry field)
- Microperforations self seal and do not show a leak on a dry Week cell. (Treat with cycloplegia, use topical aqueous suppressants and antibiotics, and cover with a fox shield.
- Larger perforations leak on Week cell challenge and require suture closure, antibiotics, cycloplegia, and coverage with a fox shield.
- Microperforations self seal and do not show a leak on a dry Week cell. (Treat with cycloplegia, use topical aqueous suppressants and antibiotics, and cover with a fox shield.
- diamond blade chipping [rare but possibly caused by a blade that is too thin or has been mishandled (e.g., scraped against metal)]
- optic nerve damage (especially in highly myopic eyes and associated with retrobulbar anesthesia, which is not indicated for use in performing incisional keratotomy)
Postoperative Considerations
Complications
- prevention
- Do not cross incisions.
- Do not incise to limbus.
- Do not redeepen periphery.,
- Do not ignore microperforation.
- Do not operate on a wet field.
- Do not cross incisions.
- adhere to sterile techniques, instill prophylactic antibiotics on the day of surgery, instruct patients to avoid potentially infective water for 2 weeks postoperatively, avoid chronic topical steroids, and discourage postoperative contact lens wear (for infectious keratitis)
- self-limited complications
- halo/starbursting (to minimize, stage the procedure with variable incisions and use a larger OZ; possibly caused by irregular astigmatism)
- diurnal visual fluctuation (usually occurs in the first weeks to months but may be permanent) and is caused by immature wound architecture and variable corneal edema but diminishes as wounds mature; older patients may be hyperopic in the morning; encourage patients not to rub their eyes)
- early regression (characterized by better vision in the morning and increased myopia toward evening; overcorrected older patients are hyperopic with symptoms throughout the day, whereas younger patients are more symptomatic in the morning; patients should avoid rubbing their eyes)
- halo/starbursting (to minimize, stage the procedure with variable incisions and use a larger OZ; possibly caused by irregular astigmatism)
- non–sight threatening complications
- undercorrection (usually requires enhancement)
- overcorrection (may be controlled with epinephrine or propine 4 times a day for 6 weeks to simulate myofibroblast contraction and with 0.5%-l% pilocarpine 4 times a day to lower IOP, which may accelerate the regression of effect; may be necessary to open and scrape out fibrous tissue from within the groove and reapproximate margins with suture closure)
- regression of effect (caused by early wound closure; operate on the patient’s nondominant eye first and adjust the technique accordingly for the patient’s dominant eye)
- progression of effect (less common because incisions often do not extend into the limbus; treat by reopening wounds, removing fibrovascular tissue, and resuturing the wound; patients should avoid contact lens wear before and after surgery)
- regular or irregular induced astigmatism (usually self-limiting but risk increases with fewer incisions, a decentered OZ, or irregular incisions, long incisions, and crossed incisions
- undercorrection (usually requires enhancement)
- miscellaneous other complications
- contact lens intolerance
- epithelial basement membrane dystrophy
- epithelial inclusion cysts
- foreign particles within grooves
- epithelial iron lines
- diminished corneal strength
- endothelial cell loss
- contact lens intolerance
- sight-threatening complications
- keratolysis [often occurs among patients with crossed incisions but also found among patients with rheumatoid arthritis or other collagen vascular diseases associated with keratoconjunctivitis sicca (these patients not considered as good candidates)]
- infectious keratitis (treat aggressively with culture and sensitivity of the stromal infiltrates and frequent broad-spectrum topical antibiotics)
- keratolysis [often occurs among patients with crossed incisions but also found among patients with rheumatoid arthritis or other collagen vascular diseases associated with keratoconjunctivitis sicca (these patients not considered as good candidates)]
Enhancements
- Perform no more than two enhancements per eye.
- Make no more than a total of eight incisions (primary plus enhancements).
- The limbal zone must be a minimum of 0.5 mm.
- The OZ must be a minimum 2.75 mm.
ASTIGMATIC KERATOTOMY
Preoperative Considerations
Preoperative care for AK is identical to that for RK patients.
Indications
- myopic or piano-spherical equivalent refraction
- astigmatic patients intolerant of contact lenses (high cylinder in the spectacle plane creates peripheral vision problems)
Patient Preparation
- Determine the axis of astigmatism using corneal topography, manifest refraction, and cycloplegic refractive results.
- Perform a case-by-case analysis if these three methods reveal disparate axes.
- For orthogonal astigmatism, use manifest refraction cylinder axis.
- For nonorthogonal astigmatism (two steep hemimeridia differ by >180 degrees), use the topographical map cylinder if consistent with refraction in its sphero-cylindrical reconstruction.
- Rely on cycloplegic refractive cylinder to support use of manifest or topographical cylinder.
- Translate the determined axis to cornea.
- Because the axis is determined with the patient upright and without sedation or a lid speculum, mark the cornea for axis with the patient in these same conditions to avoid serious axis positioning errors.
- With the contralateral eye patched and the patient seated at a slit lamp, instill the anesthetic.
- Adjust the slit-lamp light filament coaxial with the patient’s eye.
- To minimize accommodation, instruct the patient to fixate through the light filament at a distance.
- Align the slit-lamp beam (vertically or horizontally) with the light filament.
- Because the axis is determined with the patient upright and without sedation or a lid speculum, mark the cornea for axis with the patient in these same conditions to avoid serious axis positioning errors.
- Carefully abrade the epithelium at the outer margins of the long axis of the beam using jeweler’s forceps or a Sinskey hook. (In the operating room, this epithelial abrasion serves as the markings for the true 90-degree or 180-degree reference axis.)
- With the true axis in place, mark the predetermined actual astigmatism axis on the cornea (using an axis marker and surgical marking pen).
- Once markings are in place, perform pachymetry at the selected optical zone over the incision sites, and set the diamond blade at 100% of the thinner measurements.
Surgical Considerations
Methods
- Fixate the globe with two-point forceps grasping the conjunctiva near the limbus.
- Incise over the corneal marks with the diamond blade perpendicular to corneal stroma.
- Achieve maximal effect with 5- to 7-mm OZs.
- A 3-mm tangential incision yields the same effect as a 45-degree arcuate incision at a 6-mm optical zone.
- Longer incisions and arcuate incisions are more efficient.
- Longer incisions yield greater effect up to a 90-degree arc length.
- AK incisions peripheral to old scars are ineffective.
- Achieve maximal effect with 5- to 7-mm OZs.
Postoperative Considerations
Age and wound healing properties affect outcomes. For example, a 30-year-old patient should theoretically be compensated for effect: EFFECT = 100% + (patient age – 30) x 2%. Because the standard distribution of effect of AK is greater than that of RK, attempt only 60% of the full correction.
Postoperative Care
- Postoperative pharmacological care for AK patients is identical to that for RK patients (see page 72).
- Consider enhancements when applicable.
Enhancements
- Wait at least 6 weeks before attempting enhancements because AK enhancements require more time to stabilize than do radial incisions.
- Dilate patients because you will be able to more easily discern the incisions against a red reflex and avoid intersecting previous incisions.
- If postoperative topography maps show persistent irregular astigmatism in the original hemimeridian, a too-shallow or shelved incision is likely present. Properly place an adjacent incision in the same hemimeridian to correct this (possibly).
- If postoperative topography maps show a shift in astigmatism axis, irregular astigmatism, or undercorrection, use the topographical map to elongate the original incisions in the direction of the resultant steep zone.
- If the resultant refractive error is hyperopic astigmatism, cautiously reopen the original incisions , remove the fibrous plug, and reapproximate the wound margins using 10-0 nylon suture.
- Also, reapproximate wound margins using 10-0 nylon sutures (if the flat axis was incorrectly incised) unless the resultant refractive error is still myopic astigmatism. If so, place conservatively short arcuate incisions at the newly defined steep hemimeridia.
LIMBAL RELAXING INCISIONS
Preoperative Considerations
Advantages
- able to be performed with cataract surgery or separately
- may induce less postoperative healing time, glare, and discomfort than corneal relaxing incisions (CRIs) because the incision is placed at the limbus instead of inside the cornea
- a practical, relatively simple, and forgiving way to correct astigmatism (axis placement and the length of the incisions not critically precise regarding refractive effect)
- rare overcorrections
Indications
- visually significant cataracts and 0.50 to 3.00 D of astigmatism
- strong patient desire for diminished or eliminated dependency on spectacles or contact lenses following cataract surgery
- candidates for clear lens extraction who have up to 3.00 D of astigmatism
Surgical Considerations
Equipment
- corneal topographer and keratometer (determines the amount, axis, and symmetry of corneal cylinder)
- a marking device (mark the steep axis determined by topography)
- a surgical keratometer (confirms axis results before placing incisions)
- an RK/AK surgical diamond knife (e.g., the Lab Instruments L320 micrometer knife)
Methods
- For phakic patients more than 73 years old
- Customize LRI placement according to topography. (Do not consider refractive cylinder.)
- For asymmetric astigmatism, elongate the LRI slightly in the steepest of the two steep axes and shorten it (by the same slight amount) in the flatter of the two steep axes.
- For nonorthogonal astigmatism, place each of the paired LRIs at the steepest portion of the topography “bow tie” that was indicated by topography (i.e., you do not need to create paired LRIs in the same meridian).
- Mark the steep meridian of astigmatism with cautery based on the topography results that were confirmed with surgical keratometry.
- Using the diamond knife (set at 600 μm for most cases), place a 6-mm incision on the steep axis at the limbus barely anterior to the palisades of Vogt (for 1.00 D, use one 6-mm incision; for 1.00-2.00 D, use two 6-mm incisions; for 2.00-3.00 D, use two 8-mm incisions).
- Customize LRI placement according to topography. (Do not consider refractive cylinder.)
- Make shorter incisions for phakic patients less than 73 years old to achieve the same refractive effect as for older patients.
- For patients older than 80 years or those who have corneoscleral thinning, use a diamond blade set at 500 μm.
- For pseudophakic patients
- Use the same nomogram as for phakic patients.
- Base axis and amount of astigmatism on refraction only.
- Base the steep meridian on only the axis of refractive cylinder.
- Determine the symmetry of astigmatism using topography only.
- Use the same nomogram as for phakic patients.
Postoperative Considerations
Complications
Enhancements
- If a single 6-mm LRI results in undercorrection, extend the incisions to 8 mm, or make a second 6-mm incision.
- If you have made two 8-mm incisions but undercorrection still exists, then perform CRIs to treat the residual astigmatism (also for initial astigmatism >3.00 D with LRI).
- For corneal relaxing incisions (more likely to produce glare and discomfort than are LRIs because they are placed inside the corneal limbus)
- First, place two 8-mm LRIs on the steep axis at the limbus.
- Set the diamond blade at 99% of corneal depth (as determined by pachymetry).
- Create one 2-mm incision for every diopter of astigmatism over 3 D and allow an 8-mm OZ. (Exact axial placement of CRIs along the steep axis is critical because CRIs produce significantly more refractive effect than do LRIs.)
- First, place two 8-mm LRIs on the steep axis at the limbus.
Suggested Readings
Assil KK, Schanzlin DJ. Radial and Astigmatic Keratotomy: A Complete Handbook. St. Louis, MO: Poole Press; 1994.
Gills JP. Nomogram for Limbal Relaxing Incisions with Cataract Surgery. Tarpon Springs, FL: St Luke’s Cataract and Laser Institute; 1999.
Sanders DR, Hofmann RF. Refractive Surgery: A Text of Radial Keratotomy. Thorofare, NJ: Slack Inc.; 1980.
< div class='tao-gold-member'>



