Laser Thermal Keratoplasty
CHAPTER CONTENTS
The Holmium:Yttrium-Aluminum-Garnet Laser
In 1898, the Dutch medical student Leendert Lans demonstrated that localized heating with electrocautery can change the curvature of a rabbit cornea by inducing thermal shrinkage of collagen fibers. In 1964, Stringer and Parr reported that the shrinkage temperature of corneal collagen was 55 to 58°C. Gasset and Kaufman clinically applied thermal keratoplasty with a heated metal probe in 1975. Neumann et al described radial thermal keratoplasty in 1990, which proved to be of little value because of the high incidence of regression and poor predictability of results. Despite extensive study using several devices and technologies, investigators have abandoned most nonlaser modalities because of many problems:
- poor refractive predictability
- delayed epithelial healing
- recurrent corneal erosions (RCEs)
- corneal neovascularization and scarring
- regression
- stromal necrosis
- iritis
- corneal endothelial decompensation
Fortunately, computer-controlled laser technology for thermal keratoplasty enables surgeons to deliver controlled quantities of light energy to heat the cornea with exquisite precision but minimal damage to surrounding tissue. Several laser modalities are potential choices for performing laser thermal keratoplasty (LTK), of which holmium: yttrium-aluminum-garnet (Ho:YAG) is the most popular:
- Ho:YAG lasers
- diode lasers
- erbium lasers
- carbon-dioxide lasers
In this chapter, we review the advances, clinical applications, limitations, and future directions of Ho:YAG LTK.
THE HOLMIUM:YTTRIUM-ALUMINUM-GARNET LASER
The Ho:YAG laser is a solid-state laser that emits radiation in the infrared region of the electromagnetic spectrum. The anterior corneal stroma primarily absorbs the laser beam, which creates a cone-shaped temperature profile.
Advantages
- adjustability of pulse duration, repetition rate, energy per pulse, and number of pulses (achieves the ideal temperature elevation to optimize collagen shrinkage without overheating the cornea)
- ideal penetration depth (480-530 μm) for achieving stromal heating with minimal damage to adjacent tissue (no clinical data demonstrate superior long-term stability with deeper penetration)
- better refractive corrections and better long-term stability (because of more pronounced shrinkage of collagen fibrils in the anterior stroma than in the posterior stroma created by the cone-shaped stromal temperature profile vs. the cylinderlike profile produced by the hot needle used for radial thermal keratoplasty)
- ability to perform additional treatments or enhancements on patients with residual hyperopia after initial Ho:YAG LTK treatments
- usefulness for treating myopes who have been overcorrected by PRK or LASIK
Indications
- low to moderate hyperopia (+0.75-+3.0 D)
- refractive and keratometric astigmatism less than 1.0 D
Inclusion Criteria
- patient age more than 40 years
- best corrected visual acuity (BCVA) of 20/40 or better in both eyes
- normal intraocular pressure (10–20 mmHg)
- normal corneal thickness (490–590 μm)
- stable refraction for 12 months before surgery
- no history of corneal surgery or trauma (except for previous excimer laser corneal surgery)
- no ocular pathology (e.g., corneal diseases, glaucoma, or cataracts)
- no history of systemic steroid, antimetabolite, or immunosuppressant use
Two main Ho:YAG laser delivery systems have been investigated: a contact device and a noncontact device, each of which produces a different corneal temperature-time-space distribution. Generalize carefully about results obtained with various devices because differences in any of the many treatment parameters may dramatically affect the device’s thermal effects on the cornea.
Contact Laser Thermal Keratoplasty
Summit Technology Inc. (Waltham, MA) developed the first contact-probe Ho:YAG laser, which emits electromagnetic radiation and has the following specifications.
Laser Specifications
- 2.06-μm wavelength
- 300-msec pulses
- frequency of 15 Hz
- a quartz fiberoptic handpiece (delivers energy to the corneal stroma)
- a sapphire tip that has a cone angle of 120 degrees (focuses the laser energy to form a wedge-shaped collagen shrinkage zone that measures 700 μm in diameter at the corneal surface and a depth of approximately 450 μm) (Fig. 10-1)
Advantages
- ability to heat stromal collagen to a higher average temperature compared with a noncontact device
- delivers approximately twice as much energy per spot (19 mJ × 25 pulses vs. 24-30 mJ × 10 pulses)
- has three times the pulse repetition frequency (15 vs. 5 Hz)
- delivers a higher irradiance (strongly vs. weakly focused) geometry
- delivers approximately twice as much energy per spot (19 mJ × 25 pulses vs. 24-30 mJ × 10 pulses)
Methods*
- Administer topical anesthesia and 1% pilocarpine preoperatively.
- Mark the cornea with a marking instrument to define probe placements.
- Apply the contact focusing tip to the corneal surface in a consistent manner to minimize induction of irregular astigmatism.
Results†
- successful reduction of hyperopia (mean correction of 1.13 D in four patients at 1 year and 1.63 D in two patients at 2 years)
- stabilization of most regression by 6 months (continuation of regression documented in patients followed for 3 years)
- negligible incidence of induced astigmatism at 1 year
- identification of need for further refinement of predictability of the achieved correction
- abandonment of study because of 3-year regression findings
Noncontact Laser Thermal Keratoplasty
Noncontact Ho:YAG LTK uses a slitlamp delivery system (the Corneal Shaping System) from Sunrise Technologies (Fremont, CA) that does not touch the corneal surface.
Laser Specifications
- laser wavelength of 2.13 μm
- a pulse duration of 250 μs (full width at half of maximum intensity)
- a pulse repetition frequency of 5 Hz
- an adjustable pulse energy up to 300 mJ (24-30 mJ × 10 pulses)
- projection of a ring pattern (3-8 mm wide) of up to eight spots on the cornea (some studies have used one to three rings with inner-ring diameters as small as 5 mm)
- nominal spot diameter of 600 μm (containing 90% of the energy per spot)
- a nonuniform energy density distribution within the spot
* These methods are for the Summit device; presumably, the Technomed unit (Baesweiler, Germany), which is being investigated in Europe uses analogous procedures.
† ‘These are results of the Summit laser phase II trial (see Yanoff, 1995, and Thompson, 1994 in Suggested Readings).
Advantages
- well-tolerated by patients
- little maintenance
- safety
- ease of use
Indications
- hyperopia to 2.5 D
Methods
- Center treatments along the line of sight by centering the red helium neon (HeNe) laser tracer beams (wavelength = 633 nm) around the entrance pupil while the patient views a red light-emitting diode fixation source.
- Focus the laser on the surface of the cornea using calibrated green HeNe laser-focusing beams (wavelength = 543 nm).
- Begin administering topical anesthesia at least 10 min prior to treatment (1 drop at 5-min intervals up to a total of 4 drops).
- Introduce a lid speculum to open the eyelids 5 min after administering the last anesthetic drop.
- Hold the eyelids open for 3 min to allow the tear film to dry before beginning treatment.
- Because water absorbs the laser light, the timing of drops and tear-film drying is designed to standardize epithelial swelling and corneal hydration and to maximize evaporation of the tear film.
- Deliver 5 to 10 laser pulses to each treatment ring sequentially over 1 to 2 sec with total treatment energy of 2.1 to 2.4 J per ring.
- Administer antibiotic and nonsteroidal anti-inflammatory drops four times a day until the epithelium heals (usually 1-2 days).
CLINICAL STUDIES Safety and efficacy trials with the Sunrise device began outside the United States in 1993. Results from four clinical studies have been reported. In each of these trials, none of the treated eyes lost two or more lines of BCVA, and there were no clinically significant complications.
Study Parameters and Results
- Koch et al (the first sighted-eye study to correct low hyperopia ≤3D)
- 15 patients (1 eye each)
- one ring of eight spots
- centerline diameter of 6 mm
- 10 pulses of 159 to 199 mJ
- follow-up at 2 years
- improved mean uncorrected visual acuity (UCVA) (from 20/125-1 to 20/50-2)
- mean refractive correction of–1.1 D (−0.38 to −2.63 D) for 11 eyes (73%)
- no persistent refractive correction (±0.25D) for four eyes (27%)
- mean induced refractive astigmatism of 0.18 D
- 2.0 D of regression between 6 months and 2 years on average
- 15 patients (1 eye each)
- Kohnen et al
- 39 eyes with up to +4.75 D of hyperopia
- treated with two rings of eight spots each
- radial spot patterns of 5 and 6 mm, 6 and 7 mm, or 6.5 and 7.5 mm (groups A, B, and C)
- fixed pulse energy of 240 mJ
- 5 pulses of laser light administered per ring
- mean increases in lines of UCVA at 1 year for groups A, B, and C (3.7 ± 0.5, 6.8 ± 2.7, and 5.3 ± 3.3, respectively)
- mean change in the spherical equivalent of the manifest refraction (−2.08 ± 1.13 D, −1.83 ± 0.88 D, −1.22 ± 0.88 D, respectively)
- good refractive stability after 6 months
- 39 eyes with up to +4.75 D of hyperopia
- Koch et al, 1997 [phase Ila U.S. Food and Drug Administration (FDA) trials of noncontact Ho:YAG LTK]
- 28 eyes with up to +3.88 D of hyperopia
- one or two rings each containing eight spots
- centerline diameters of 6 mm (one ring) or 6 to 7 mm (two rings) (Fig. 10-2)
- 10 pulses of 208 to 242 mJ
- improved UCVA by one or more lines in 19 of 26 (73%) of the treated eyes at 2 years
- mean change in spherical equivalent of the subjective manifest refraction (−0.53 ± 0.33 D and −1.48 ± 0.58 D for the one- and two-ring treatment groups, respectively)
- regression of 0.1 D for the one-ring group and 0.2 D for the two-ring group (6 months to 2 years)
- one or two rings each containing eight spots
- 28 eyes with up to +3.88 D of hyperopia
- Vinciguerra et al, 1998 (effects of two different three-ring treatment patterns)
- one session on 16 eyes of eight patients with a mean preoperative subjective cycloplegic refraction (SCR) of +4.90 ± 1.17 D
- three eight-spot rings at ring diameters of 6, 7, or 8 mm
- 10 pulses at a pulse energy of 240 mJ
- treatment of one eye of each patient with a “radial” pattern (the spots of the three rings aligned on the eight semimeridians)
- treatment of the fellow eye with a “staggered” pattern (the spots of the contiguous rings offset 22.5 degrees from each other)
- postoperative mean SCR of +2.75 ± 1.6 D in eyes treated with the radial pattern and +3.40 ± 1.6 D in eyes treated with the staggered pattern
- mean change in SCR of 2.15 D and 1.50 D, respectively
- mean improvement in UCVA of five lines in the radial eyes and four lines in the staggered eyes
- earlier return of mean BCVA to preoperative levels in the radial group
- one-year improvement of BCVA by one line in the radial eyes but no lines in staggered eyes
- larger and more uniform corrected zones in the radial group [indicated by Scheimpflug photography and computerized videokeratography (CVK)]
- because of this study all subsequent Ho:YAG LTK trials conducted using the radial pattern with either two or three rings
- 10 pulses at a pulse energy of 240 mJ
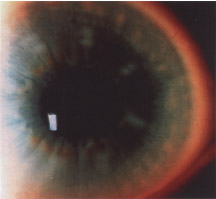
- Koch et al‡ (the FDA-monitored phase III studies of noncontact Ho:YAG LTK)
- 648 hyperopic eyes (+0.75 to +2.50 D)
- enrollment criteria as noted for prior studies (see above)
- two concentric eight-spot rings at diameters of 6 to 7 mm
- seven pulses per spot
- pulse energies ranging from 226 to 256 mJ (Fig. 10-3)
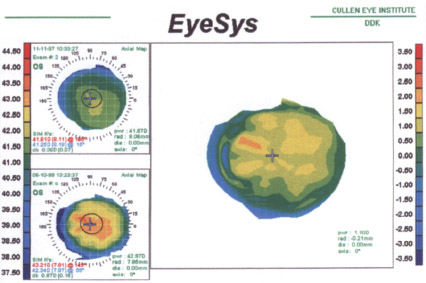
- reduction in hyperopia of 0.5 D or more in 92% of eyes [1.5-2.5 D in 39% of eyes (Fig. 10-4)]
- loss of effect of 0.4 D from 6 to 12 months
- change in stability of less than 1 D in 95% of eyes by 6 months (FDA criterion is <1 D change in 95% of eyes at 3-month intervals)
- good predictability (65% of eyes within ±5 D of attempted correction and 88% of eyes within ±1.0 D of attempted)
- UCVA of ≥20/40 achieved in 86% of eyes and UCVA of ≥20/25 achieved in 57% of eyes
- reduction of full-time dependency on spectacles (from 79% to 13% in patients with hyperopia to +1.99 D and from 91 to 13% in patients with hyperopia of 2.0-2.5 D)
- loss of more than two lines of BCVA at 6 months in one patient (because of a cataract that was presumed to be unrelated to the treatment)
- indication of procedure as extremely safe and effective for treatment of low hyperopia (exceeded all FDA criteria by 6 months postoperatively)
- change in stability of less than 1 D in 95% of eyes by 6 months (FDA criterion is <1 D change in 95% of eyes at 3-month intervals)
- 648 hyperopic eyes (+0.75 to +2.50 D)
- Acer et al §
- 16 spots per ring with two rings at 6 and 7 mm (for treatment of hyperopia of 2.75-4.0 D)
- mean corrections at 6 months slightly greater than 3 D
- no reports of any sight-threatening complications
- 16 spots per ring with two rings at 6 and 7 mm (for treatment of hyperopia of 2.75-4.0 D)
- Pop, 1998
- noncontact Ho:YAG LTK in treating hyperopia following PRK for overcorrection of myopia after PRK
- 36 eyes (33 patients) that underwent noncontact Ho:YAG LTK
- no need for further retreatments for two-thirds of retreated eyes at 12 months after Ho:YAG LTK for an initial PRK
- noncontact Ho:YAG LTK in treating hyperopia following PRK for overcorrection of myopia after PRK
- Ismail et al, 1998 (the efficacy and safety of noncontact Ho:YAG LTK)
- 11 patients (13 eyes) with hyperopia induced by LASIK
- eight pulses per spot
- two staggered rings of eight spots at 6.0 and 7.0 mm
- energy levels from 215 to 245 mJ
- mean follow-up of 18 months
- mean spherical equivalent of +4.60 D preoperatively, –0.5 D at 3 months, +0.48 D at 17 months, and +0.76 D at 18 months postoperatively
- conclusion that Ho:YAG LTK is safe and effective for correcting LASIK-induced hyperopia (perhaps because of reduced corneal thickness and/or the presence of a circular incision in Bowman’s membrane)
- 11 patients (13 eyes) with hyperopia induced by LASIK
‡ Presented at the American Society of Cataract and Refractive Surgery Symposium on Cataract, Intraocular Lens, and Refractive Surgery: April 1999; Seattle.
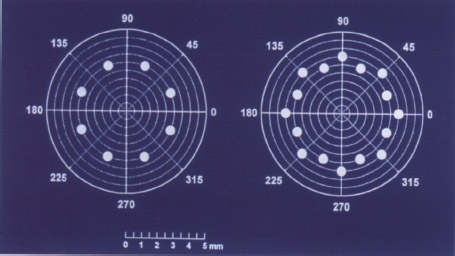
Figure 10-2 One- and two-ring patterns used in early noncontact Ho:YAG LTK studies.
Complications
Sight-Threatening
- irregular astigmatism
- In Summit FDA trials, 9% of patients lost at least two lines of BCVA in one year, which resolved over time.
- U.S. and international studies performed with the Sunrise Corneal Shaping System have reported no treatment-induced loss of more than two lines of BCVA.
- In Summit FDA trials, 9% of patients lost at least two lines of BCVA in one year, which resolved over time.
- visual aberrations (e.g., glare, loss of contrast sensitivity, decreased night vision)
- In the Sunrise series, patients had no mean loss of contrast sensitivity, no loss of glare acuity, and did not complain of decreased night vision.
- visually significant corneal scarring
- By 3 to 5 years postoperatively, treatment sites are not visible to the naked eye and are barely perceptible even by slit-lamp biomicroscopy.
- Visual symptomatology because of the presence of the spots has not been reported.
- By 3 to 5 years postoperatively, treatment sites are not visible to the naked eye and are barely perceptible even by slit-lamp biomicroscopy.
- endothelial cell loss
§ Presented at the American Society of Cataract and Refractive Surgery Symposium on Cataract, Intraocular Lens, and Refractive Surgery: April 1999; Seattle.
- infection (theoretically possible but no reports exist)
Non-Sight-Threatening
- undercorrection (caused by inadequate initial treatment or regression of effect)
- The high incidence of regression led to abandonment of the Summit trials.
- Efficacy is limited to adults older than 40 years who have hyperopia to 2.S D (potentially extended to 4.0 D).
- The high incidence of regression led to abandonment of the Summit trials.
- overcorrection
- Required in the first 3 to 6 months to compensate for early regression.
- Long-term overcorrection is uncommon.
- Required in the first 3 to 6 months to compensate for early regression.
- increased astigmatism
- In the phase III Sunrise study, induced manifest refractive cylinder of more than 2.00 D occurred in only 0.9% of eyes, which is well below the FDA threshold of 5%.
- RCEs
- Theoretically possible as a result of epithelial injury, but none have been reported.
FUTURE DIRECTIONS
Despite an experimental history of more than 100 years, Ho:YAG LTK is in its clinical infancy. Clinical studies are in progress in the United States to assess the role of noncontact Ho:YAG LTK in treating presbyopia by inducing myopia in an emmetropic eye. Work is underway to develop treatment patterns that can be used for correcting astigmatism.
Sunrise has developed a new noncontact laser, the Hyperion, to replace the Corneal Shaping System (Fig. 10-5); this new device has multiple advantages, including eye tracking, automatic delivery of the second ring without refocusing, and extraordinary programmability for spot placement and energy level.

Figure 10-5 The Hyperion laser, which is the new noncontact Ho:YAG laser manufactured by Sunrise.
A continuous-wave diode laser that emits energy at 1.885 μm (Rodenstock, Inc.) is now available in Europe and under clinical investigation for the treatment of hyperopia and hyperopic astigmatism. Finally, a nonlaser technology, radiofrequency thermal keratoplasty, is in the early stages of FDA study for treatment of low hyperopia.
As we better understand the response of the cornea to thermal change, devices, and treatment, we should expect improved parameters to further enhance the magnitude and stability of refractive change that can be produced by Ho:YAG LTK. We believe that Ho:YAG LTK is on the verge of becoming an integral part of the refractive surgical armamentarium.
Suggested Readings
Bende T, Jean B, Oltrup T. Laser thermal keratoplasty using a continuous wave diode laser. J Refract Surg. 1999;15:154-158.
Cavanaugh TB, Durrie DS. Holmium YAG laser thermokeratoplasty: synopsis of clinical experience. Semin Ophthalmol 1994;9:110-116.
Durrie DS, Schumer J, Cavanaugh TB. Holmium laser thermokeratoplasty for hyperopia. J Refract Corneal Surg. 1994;10:S277-S280.
Feldman ST, Ellis W, Frucht-Pery J, Chayet A, Brown SI. Regression of effect following radial thermokeratoplasty in humans. J Refract Corneal Surg. 1989;5:288-291.
Gasset AR, Kaufman HE. Thermokeratoplasty in the treatment of keratoconus. Am J Ophthalmol. 1975;79:226-232.
Ismail MM, Alió JL, Pérez-Sntonja JJ. Non-contact thermal keratoplasty to correct hyperopia induced by laser in situ keratomileusis. J Refract Surg. 1998;24:1191-1194.
Ismail MM, Pérez-Sntonja JJ, Alio JL. Laser thermal keratoplasty after lamellar corneal cutting. J Refract Surg. 1999;25:212-215.
Koch DD, Abarca A, Villarreal R, et al. Hyperopia correction by noncontact holmium: YAG laser thermal keratoplasty: clinical study with 2-year follow-up. Ophthalmology. 1996; 103:731-740.
Koch DD, Kohnen T, McDonnell PJ, Menefee RF, Berry MJ. Hyperopia correction by noncontact holmium:YAG laser thermal keratoplasty: U.S. phase IIa clinical study with 2-year follow-up. Ophthalmology. 1997;104:1938-1947.
McDonnell PJ, Garbus J, Romero N, Rao A, Schanzlin DJ. Electrosurgical keratoplasty: clinicopathologic correlation. Arch Ophthalmol. 1988;106:235-238.
Moriera H, Campus M, Sawusch MR, McDonnell JM, Sand B, McDonnell PJ.
Holmium laser keratoplasty. Ophthalmology. 1993;100:752-761.
Neumann AC, Fyodorov S, Sanders DR. Radial thermokeratoplasty for the correction of hyperopia. J Refract Corneal Surg. 1990;6:404-412.
Peyman GA, Larson B, Raichand M, Andrews AH. Modification of rabbit corneal curvature with the use of carbon dioxide laser burns. Ophthalmic Surg. 1980;11:325-329.
Pop M. Laser thermal keratoplasty for the treatment of photorefractive keratectomy over-corrections: a 1-year follow-up. Ophthalmology. 1998;105:926-931.
Rowsey JJ, Doss JD. Preliminary report of Los Alamos keratoplasty techniques. Ophthalmology. 1981;88:755-760.
Seiler T. Ho:YAG laser thermokeratoplasty for hyperopia. Ophthalmol Clinics North Am. 1992; 5:773-780.
Seiler T, Matallana M, Bende T. Laser thermokeratoplasty by means of a pulsed holmium:YAG laser for hyperopic correction. J Refract Corneal Surg. 1990;6:335-339.
Stringer H, Parr J. Shrinkage temperature of eye collagen. Nature. 1964;204:1307.
Thompson VM. Holmium:YAG laser thermokeratoplasty for correction of astigmatism. J Refract Corneal Surg. 1994;10:S293.
Vinciguerra P, Azzolini M, Radice P, Epstein D, Kohnen T, Koch DD. Comparison of radial and staggered treatment patterns for the correction of hyperopia in noncontact holmium:YAG laser thermal keratoplasty. J Cataract Refract Surg. 1998;24:21-30.
Yanoff M. Holium laser hyperopia thermokeratoplasty update. Eur J Implant Refract Surg. 1995;7:89-91.
Zhou Z, Ren QS, Simon G, Parel JM. Thermal modeling of laser photothermo-keratoplasty (LPTK). SPIE Proc. 1992;1644:61-71.
< div class='tao-gold-member'>



