6
Grading and Classification of Uveitis
John J. Huang, Paul A. Gaudio, and Eric J. Sigler
It is imperative that practitioners understand and are comfortable utilizing a standard classification system for uveitis. This chapter explains why this is so and how we classify uveitis for the purposes of clinical management.
WHY CLASSIFICATION IS IMPORTANT
The need for a standardized classification system stems from the fact that uveitis is not a single disease or even a collection of well-defined diseases. Rather, the term “uveitis” encompasses the entire range of inflammatory conditions of the uveal tract (i.e., the iris, ciliary body, and choroid). With a few exceptions, there are no pathologic or laboratory findings that define any form of uveitis, and no one clinical finding is common to all forms (although almost all forms involve cells in the normally cell-free aqueous and vitreous humors). Uveitis specialists therefore treat a wide range of diseases affecting one or many parts of one or both eyes and causing a variety of ocular complications over varying amounts of time. Historically, there were no widely accepted or established names for most of these clinical entities. As uveitis has developed as a subspecialty and the number of subspecialists has increased, practitioners have had difficulty describing and discussing their cases in terms that all could recognize, a fact that has hampered efforts to collaborate or share data or even to organize patients into groups of like entities for clinical trial purposes. A system of terms for describing and classifying uveitic diseases is thus useful to these efforts.
There is no universally accepted standard classification system for use in the clinical management of uveitis. In practice, as is typical of all fields of medicine, most uveitis specialists (including ourselves) utilize whatever system they learned from their teachers, often with slight modification. The result is that that there are currently several systems in common use, most of which resemble each other. The Standardization of Uveitis Nomenclature (SUN) Working Group, which was a workshop of uveitis specialists convened in 2004, endeavored to achieve consensus on the precise definition of various clinical findings for purposes of enabling collaborative research. This group did achieve consensus on many important issues, yet stopped short of recommending a complete system or a system optimized for clinical use. The classification scheme that we describe here uses terms that most practitioners would agree with, in a format that we and those who taught us find practical (Table 6.1). We note that this system is based heavily on and largely resembles what was handed down to us in training and is really not the fruit of our own creative efforts.
Table 6.1 Anatomic classification of uveitis based on Standardization of Uveitis Nomenclature (SUN) for reporting clinical data
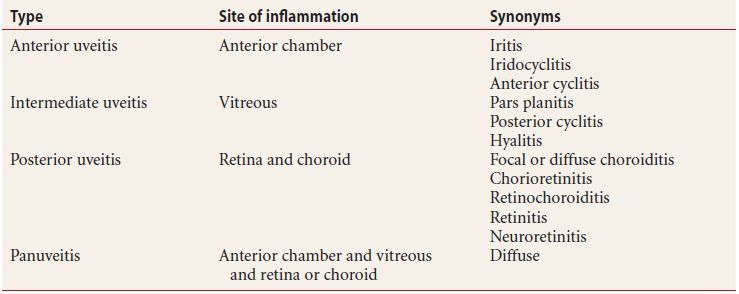
APPROACH TO CLASSIFICATION OF UVEITIS
We categorize all cases of uveitis in four respects:
- Disease course, meaning whether it is acute, chronic, or recurrent
- Laterality, meaning whether it is unilateral or bilateral
- Character, meaning whether it is granulomatous or nongranulomatous
- Main location in the eye, meaning anterior, intermediate, posterior, or diffuse (also termed panuveitis) if multiple locations are affected to similar degrees (see Table 6.2)
Table 6.2 Classification of uveitis
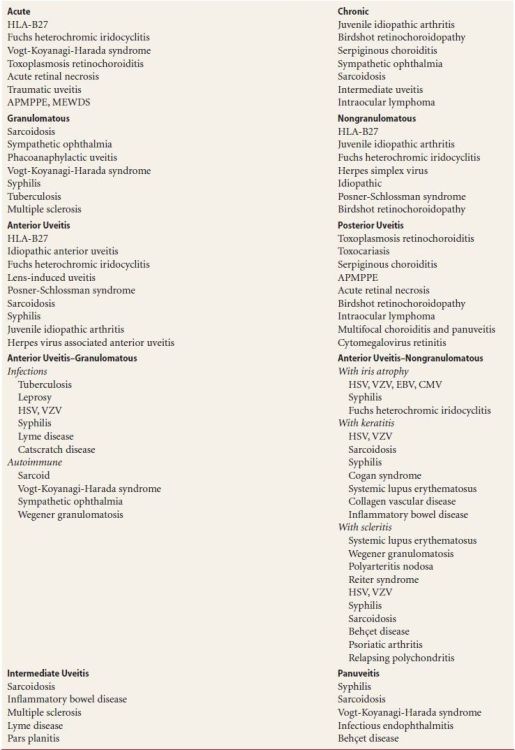
APMPPE, Acute posterior multifocal placoid pigment epitheliopathy; CMV, cytomegalovirus; EBV, Epstein-Barr virus; HLA, human leukocyte antigen; HSV, herpes simplex virus; MEWDS, Multiple evanescent white dot syndrome; VZV, varicella zoster virus.
In classifying a patient’s disease, the practitioner selects one term (in bold above) from each of these four categories and states them all in a sequence from 1 to 4 as numbered above, the result being a four-part description, (in which 48 descriptive permutations are possible).
This system enables grouping patients with similar diseases while distinguishing outliers. As an example, consider two children who could both be said to have “arthritis and uveitis.” More precisely, one child has “chronic, bilateral, nongranulomatous, anterior uveitis,” which is a form of uveitis most commonly associated with juvenile idiopathic arthritis (JIA). Practitioners hearing this description will generally understand that this is a child who probably has JIA. The other child has “chronic, bilateral, granulomatous, diffuse uveitis.” Practitioners hearing this description would certainly not envision a child with JIA, since JIA-associated uveitis is neither granulomatous nor diffuse. In fact, this child is more likely to have sarcoidosis, and this understanding would inform the workup and therapeutic approach quite substantially. In the absence of a classification system that brings this distinction to light, these children would have been grouped together, when in fact their diseases are certainly different. We define below the terms involved in this classification system.
DISEASE COURSE: ACUTE, RECURRENT, OR CHRONIC
In the first 3 months after the initial presentation of a patient’s first bout of uveitis, the condition is considered to be in the acute phase. After 3 months of disease activity or if treatment is necessary to control the inflammation after 3 months, the disease is termed chronic. Uveitis that has been inactive without treatment for at least 3 months and then recurs is termed recurrent. This 3-month period of inactivity without treatment is important, because uveitis that recurs within 3 months is considered to have not been truly inactive. The term chronic applies to both the initial, or acute episode, and the recurrent episodes that last more than 3 months. It will be apparent that a patient’s uveitis may be reclassified multiple times, changing between recurrent and chronic depending on the course of the inflammation. Note: all terms refer to both eyes considered together, not to either eye specifically. For example, consider a patient who had an episode of uveitis in one eye that resolved a year ago and now has a similar episode in the other eye: this patient has recurrent uveitis.
LATERALITY: UNILATERAL OR BILATERAL
We state whether the uveitic process affects one eye or both. In making this determination, all prior episodes of uveitis are counted, such that in the case of the patient mentioned just above, who had an episode of uveitis in one eye that resolved a year (or even many years) ago and now has a similar episode in the other eye; this patient has recurrent, bilateral uveitis, even though only one eye is currently inflamed. Additionally, the disease that is barely active in one eye and quite florid in the other is still considered bilateral, however asymmetric.
GRANULOMATOUS OR NONGRANULOMATOUS
Features that define a granulomatous presentation are large keratic precipitates (KP) and iris nodules. The presence of either of these features at any point in the disease process merits the designation granulomatous, in our view. Of all the terms used in our classification scheme, this one is the most challenging and is subject to interobserver variability, for several reasons. Firstly, KP appear in various sizes, ranging from huge “mutton-fat” lesions that no ophthalmologist would miss to stellate KP that might be confused with mere nongranulomatous clusters of cellular debris. Secondly, iris nodules are often difficult to see without a thorough examination of the iris stroma and anterior chamber (AC) angle. Thirdly, both KP and iris nodules may disappear after treatment is initiated but before it is completed. In Chapter 18, we describe clues indicating resolved granulomatous features that are helpful in making this determination. As above, all terms refer to both eyes considered together, not to either eye specifically, so that a patient with granulomatous disease in one eye and nongranulomatous inflammation in the other is nevertheless considered to have bilateral, granulomatous uveitis. In addition, uveitis that presented with KP or iris nodules even only once retains the designation granulomatous forever, regardless of whether subsequent episodes appear granulomatous in character or not (Figs. 6.1 and 6.2).
Figure 6.1 Granulomatous panuveitis with mutton-fat keratic precipitates in the anterior chamber, vitreous cells in the posterior segment and inflammatory debris over the inferior vitreous base.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


