17
Drug-induced Uveitis
John J. Huang
INTRODUCTION
Drug-induced uveitis is an uncommon adverse reaction to both topical and systemic medical therapy. While an extensive list of medications has been reported to be associated with intraocular inflammation, the medications in this chapter are administered systemically or topically with cause and effect with uveitis proven or highly probable (Table 17.1). Medication-induced uveitis is often overlooked by ophthalmologists in the differential diagnosis of patients with ocular inflammation. A high index of suspicion is often required in patients on a variety of systemic and topical medical therapies. A thorough workup for infectious and noninfectious etiologies should be performed to rule out possible common causes of uveitis. Familiarity with the listed common medications traditionally associated with uveitis can greatly aid in this diagnosis of exclusion. The treatment of drug-induced uveitis will require cessation of the offending drug, in addition to the aggressive use of topical or systemic corticosteroid therapy. To further confirm the diagnosis, rechallenge with the suspected drug should be performed after resolution of the initial course of inflammation. Flare-up of the ocular inflammation after reinitiation of the possible offending drug often confirms the cause and effect of the drug-induced uveitis (Table 17.2).
Table 17.1 Pathogenesis of drug-induced uveitis
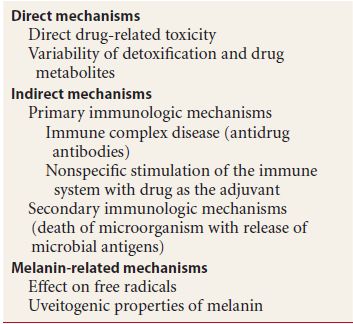
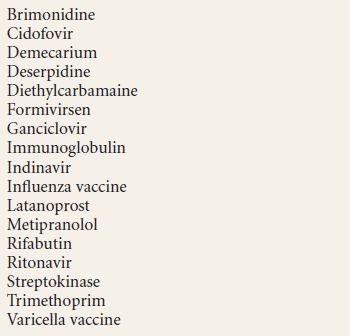
Table 17.2 Medication-induced uveitis
Naranjo proposed seven different criteria to establish causality in adverse drug reactions.
- The reaction is a frequently described event that is well documented.
- Recovery occurs upon withdrawal of the offending drug.
- Other possible causes for the event have been excluded.
- The reaction becomes more severe when the dose of the drug is increased.
- The adverse event is documented by objective evidence.
- Similar effects can occur in a given patient with similar drugs.
- The event should recur on rechallenge with the suspected drug.
BIPHOSPHONATES-ASSOCIATED UVEITIS
Biphosphonates are inhibitors of bone resorption that are commonly used in the management of osteoporosis, Paget disease, and malignancy-induced hypercalcemia. Two of these agents, oral risedronate, a third- generation biphosphonate, and intravenous infusion of pamidronate have been associated with anterior uveitis. The majority of the cases have been associated with intravenous infusion of pamidronate disodium. Most clinical symptoms develop within 24 to 48 hours of initiating treatment. The compound has been associated with the release of interleukins 1 and 6, leading to a possible type III hypersensitivity reaction and ocular inflammation. Systemically, both risedronate and pamidronate have been associated with low-grade fever and flulike symptoms early in the treatment course.
Clinical Findings
- Anterior uveitis is usually mild and easily treated with topical corticosteroids.
- Transient conjunctivitis.
- Episcleritis.
- Scleritis.
- Orbital inflammation and myositis of the extraocular muscles.
Treatment
- Cessation of therapy
- Topical corticosteroids for mild inflammation
- Oral corticosteroids for severe inflammation
CIDOFOVIR-ASSOCIATED UVEITIS
Cidofovir is a nucleotide analogue that inhibits viral DNA polymerase. Its efficacy and safety have been demonstrated for the treatment of cytomeglovirus (CMV) infection in patients with AIDS. Case series of intravitreal injection of cidofovir have been effective in preventing the relapse of CMV retinitis. Ocular inflammation has been described in patients receiving intravenous and intravitreal injection of cidofovir. These initial observations were independent of whether patients were treated with highly active antiretroviral therapy, especially protease inhibitor therapy. Severe hypotony with irreversible vision loss occurred in 1% of injections and 3% of eyes, and transient hypotony with recovery of vision loss in 14% of eyes. Intravenous cidofovir produces similar changes usually after 5 days of treatment with possible bilateral presentation. The typical case of uveitis and hypotony will resolve in 2 weeks with treatment.
Cidofovir causes hypotony by damaging the nonpigmented epithelium of the ciliary body. In severe cases, this can lead to ciliary body atrophy.
Clinical Findings
- Nongranulomatous anterior uveitis with severity of uveitis dependent on frequency and dose of medication
- Hypotony
- Posterior synechie
- Cataract formation
- Hypotony maculopathy
- Cystoid macular edema
Treatment
- Oral probenecid
- Topical corticosteroids for anterior uveitis
- Topical cycloplegics
- Cessation of cidofovir therapy
METIPRANOLOL-ASSOCIATED UVEITIS
Metipranolol is a nonselective beta-blocker that lowers intraocular pressure by decreasing aqueous production. The drug was introduced in 1986 to treat glaucoma at three different concentrations of 0.1%, 0.3%, and 0.6%. In 1991, overall 60 cases of metipranolol-associated granulomatous uveitis were described in a dose-dependent fashion. Most cases developed after 7 to 31 months on metipranolol therapy. Rechallenge after the resolution of inflammation caused recurrence of disease within 4 to 14 days. All uveitis patients responded well to topical corticosteroids and cycloplegics within weeks of treatment.
Clinical Findings
- Granulomatous anterior uveitis with large mutton fat keratic precipitates, no busacca, or koeppe nodule
- Rare cases of nongranulomatous anterior uveitis
- Significantly increased intraocular pressure during uveitis episodes
Treatment
- Discontinue metipranolol therapy
- Topical corticosteroid therapy
- Topical cycloplegics
ORAL CONTRACEPTIVES–ASSOCIATED UVEITIS
Oral contraceptives are hormonal analogues used in the treatment of menopausal symptoms, uterine bleeding, dysmenorrhea, amenorrhea, and most commonly for birth control. Isolated cases of anterior and posterior uveitis associated with oral contraceptive use have been described.
Clinical Findings
- Anterior uveitis
- Posterior uveitis
- Retinal vasculitis
Treatment
- Discontinue oral contraceptives
- Topical corticosteroids for anterior uveitis
- Oral corticosteroids or posterior uveitis and retinal vasculitis
RIFABUTIN-ASSOCIATED UVEITIS
Rifabtuin is a lipophilic semisynthetic derivative of rifamycin and rifampin, and is used as oral prophylactic treatment of disseminated Mycobacterium avium complex infections in patients with AIDS. Additional applications include refractory cases of pulmonary tuberculosis and inflammatory bowel disease. Rifabutin-associated intraocular inflammation is one of the most well-documented form of drug-induced uveitis. In 1990, several cases of AIDS patients treated with rifabutin developed reversible cases of arthralgia, arthritis, and uveitis. The uveitis ranged from mild anterior uveitis to severe panuveitis. The cases responded well to corticosteroid therapy and discontinuation of the rifabutin after 6 to 10 weeks. The use of rifabutin at 600 mg daily produces uveitis in 8% of cases. Uveitis can develop between 2 weeks and 9 months while on therapy. It is clear that rifabutin-associated uveitis is dose related with lower incidence at lower maintenance doses. Concomitant use of fluconazole and clarithromycin, both processed by the hepatic microsomal cytochrome P-450, may lead to elevated levels of rifabutin and an increased risk of uveitis.
Clinical Findings
Systemic Findings
- Diffuse polyarthralgia (19%)
- Gastrointestinal symptoms (42%)
- Abnormal liver enzymes (12%)
- Decrease level of total blood count (100%)
- Transient skin rash
Ocular Findings
- Unilateral or bilateral nongranulomatous anterior uveitis
- Panuveitis
- Rare hypopyon formation
Treatment
- Discontinue rifabutin
- Aggressive topical corticosteroids for anterior uveitis
- Oral corticosteroids for severe bilateral panuveitis
- Subtenons triamcinolone injections patients intolerant to systemic corticosteroids
SULFONAMIDE-ASSOCIATED UVEITIS
Systemic sulfonamides are commonly used antibiotic used for the treatment of Gram-positive and some Gram-negative bacteria. The combination trimethoprim-sulfamethoxazole (TMP-SMX) is use for the treatement of urinary tract infection, toxoplasmosis, cat-scratch disease, and Pneumocystis carinii. Sulfa-related medical therapies have been associated with idiosyncratic hypersensitivity reaction of Steven-Johnson syndrome. Its association with uveitis is often overlooked and not recognized. Ocular inflammation associated with sulfonamides are always anterior uveitis, develop within 1 to 8 days of initiation of therapy. The ocular inflammation is often bilateral. The anterior uveitis recurred within 24 hours upon rechallenge with TMP-SMX.
Clinical Findings
- Nongranulomatous anterior uveitis
- Rare posterior uveitis and retinal vasculitis
Treatment
- Discontinuation of sulfonamides
- Topical corticosteroids
- Topical cycloplegics
- Oral corticosteroids in cases with posterior uveitis and retinal vasculitis
VACCINES (BACILLE CALMETTE-GUERIN)
The Bacille Calmette-Guerin (BCG) vaccine was approved in the United States for the immunization of tuberculosis and the treatment of bladder carcinoma. Augmentation of the immune response against the Mycobacterium tuberculosis and malignant cells are presumed immunologic mechanism of action. Case reports of bilateral anterior uveitis, extensive loss of iris pigmentation, and vitiligo at the injection site after BCG treatment for malignancies have been reported. There was no evidence of vitritis and posterior uveitis. The uveitis was treated successfully with topical corticosteroids and cycloplegics, with resolution of inflammation in weeks to months. A similar uveitis can be induced in the animal model if BCG and uveal tissue are injected in the guinea pigs.
Clinical Findings
Systemic Findings
- Arthritis
- Vitiligo at the location of BCG injection
Ocular Findings
- Nongranulomatous anterior uveitis
- Iris atrophy and loss of iris pigmentation
Treatment
- Topical corticosteroids
- Topical cycloplegics
VACCINE (INFLUENZA)
Influenza vaccination has been associated with uveitis in several patient case reports. One of the patients did not have any history of uveitis, while four other patients did have previous history of uveitis or complicated cataract surgery. Patients developed anterior uveitis, vitritis, and optic neuritis. The vaccination may act as a nonspecific stimulant of the immune response leading to the activation of existing uveitis and possibly triggering new inflammation. The anterior uveitis can be successfully treated with topical corticosteroids, while the posterior uveitis required systemic corticosteroids.
Clinical Findings
- Anterior uveitis
- Vitritis
- Optic neuritis
Treatment
- Topical corticosteroids for anterior uveitis
- Systemic corticosteroids for vitritis and optic neuritis
TUBERCULIN (PURIFIED PROTEIN DERIVATIVE) SKIN TEST
Tuberculin skin test is commonly used to determine prior exposure to the organism M. tuberculosis. Panuveitis has been reported in patients 2 weeks after tuberculin challenge. The time course suggests a cell-mediated immune response of a type IV delayed hypersensitivity reaction. Additional case reports of patients with known history of positive tuberculin test present with a clinical picture of multifocal choroiditis and Vogt-Koyanagi-Harada syndrome after repeat tuberculin skin testing.
Clinical Findings
- Anterior uveitis
- Vitritis
- Choroiditis
- Serous retinal detachment
Treatment
- Topical corticosteroids.
- Systemic corticosteroids.
- In patients with a positive tuberculin skin test, consider systemic antimycobacterial medication such as isoniazid as well.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


