19
Medical Management of Ocular Inflammation
Deanne Nakamoto and Paul A. Gaudio
OVERVIEW
We organize our therapeutic goals for uveitis management into the paradigm of establishing both immediate control and long-term control, choosing drugs based on their efficacy and tolerability. Drug classes that are well suited for immediate control may not be appropriate for long-term control, and vice versa. The focus of this chapter is an algorithm for the treatment of noninfectious uveitis.
- Imediate control refers to eliminating active inflammation right now, using therapy that may not be sustainable for the long term—often starting with high-dose corticosteroids in some form. Immediate control is the essential first step in managing ocular inflammation.
- Long-term control involves preventing inflammation from reactivating after it has been rendered inactive. It is made difficult by the fact that corticosteroids, which are almost always the therapy used to achieve immediate control, have numerous side effects making them unsuitable for long-term use. Long-term control thus requires finding the therapy that has the fewest side effects, but is still able to prevent disease recurrence. This may include low-dose corticosteroids, corticosteroid injections, implants, or immunosuppressive drugs. Most practitioners find long-term control to be the most challenging part of uveitis management.
In this chapter, we discuss the different classes of drugs that can be considered when formulating a therapeutic plan for immediate and long-term control.
ACHIEVING IMMEDIATE CONTROL
Corticosteroids for Immediate Control
No class of drugs is as rapid or as efficacious as corticosteroids in achieving an immediate control of inflammation. Thus, when patients present with ocular inflammation that we believe is not infectious, corticosteroids are the first drugs that we use. This drug class includes a number of different agents, which are delivered as eyedrops, periocular injections, intravitreal injections, oral preparations, or intravenous infusions.
Corticosteroid Eyedrops
- Pharmacology
- Regardless of the route of administration, corticosteroids have an anti-inflammatory and immunosuppressive effect.
- They decrease the production and migration of most immune cells via the inhibition of phospholipase A2, decreasing both prostaglandin and leukotriene production.
- Regardless of the route of administration, corticosteroids have an anti-inflammatory and immunosuppressive effect.
- Ophthalmic uses
- Anterior uveitis. Corticosteroid eyedrops, namely, prednisolone (acetate or phosphate) 1% or dexamethasone 0.1%, are most suitable for achieving immediate control of anterior uveitis (iritis or iridocyclitis).
- Episcleritis and conjunctivitis. Weak corticosteroids are to be used with caution in cases of episcleritis and conjunctivitis because of the risk of dependency.
- Anterior uveitis. Corticosteroid eyedrops, namely, prednisolone (acetate or phosphate) 1% or dexamethasone 0.1%, are most suitable for achieving immediate control of anterior uveitis (iritis or iridocyclitis).
- Administration
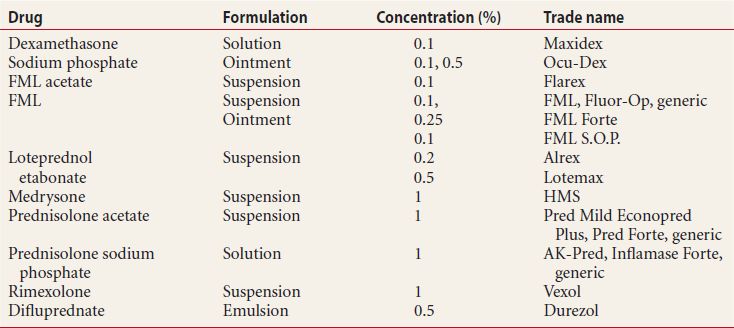
Table 19.1 shows the different topical steroids available today.
- Prednisolone acetate 1% is the most commonly used corticosteroid eyedrop in the United States, and hence is the most widely available. It is a suspension and thus must be shaken before use. The key to using topical corticosteroid eyedrops successfully is to dose them very frequently initially; the most common reason for failure to control inflammation when using these drugs is insufficient dosing. As a rule, we start them hourly when treating anterior uveitis, with a subsequent taper depending on the severity of the initial presentation. No difference in efficacy has ever been shown between generic versus name brand formulations of prednisolone acetate eyedrops. The main difference as we see it is in the packaging.
- Prednisolone sodium phosphate 1% is a solution and is equally as potent.
- Dexamethasone phosphate 0.1% solution is also available in the United States, but less widely used. To us, it appears as potent as prednisolone 1%.
- Fluorometholone (FML) 0.1% and 0.25% are less-potent corticosteroid preparations. They may be good choices for surface inflammation (e.g., episcleritis, pingueculitis, conjunctivitis), as they provide some anti-inflammatory effect while limiting the likelihood of the typical steroid side effects, discussed next.
- Difluprednate 0.5% is a much newer drug that is marketed as exceeding other topical corticosteroids in potency. Independent clinical trials are lacking, but we find it at least as effective as prednisolone, and possibly more so.
- Prednisolone acetate 1% is the most commonly used corticosteroid eyedrop in the United States, and hence is the most widely available. It is a suspension and thus must be shaken before use. The key to using topical corticosteroid eyedrops successfully is to dose them very frequently initially; the most common reason for failure to control inflammation when using these drugs is insufficient dosing. As a rule, we start them hourly when treating anterior uveitis, with a subsequent taper depending on the severity of the initial presentation. No difference in efficacy has ever been shown between generic versus name brand formulations of prednisolone acetate eyedrops. The main difference as we see it is in the packaging.
- Side effects
Topical steroids have numerous side effects that ultimately limit their usefulness for long-term control. These include the following:
- Intraocular pressure (IOP) elevation, which can occur at any time but most commonly starts somewhere after one month of therapy and may even begin years later. The likelihood and severity are greater with more frequent dosing, but all doses, even one drop daily, can cause this side effect. The IOP increase almost invariably resolves when the drops are stopped.
- Posterior subcapsular cataracts generally do not progress after the drops are stopped. There is a great deal of variability in how sensitive individuals are to this side effect, but we think that one should almost always expect to see it after 1,200 doses (equivalent to 4 drops per day for 10 months).
- Subconjunctival hemorrhages should be expected in patients using corticosteroid eyedrops chronically. They usually involve one vessel, which ruptures continually— such that patients have repeated hemorrhages in the same spot, until it scars over.
- Intraocular pressure (IOP) elevation, which can occur at any time but most commonly starts somewhere after one month of therapy and may even begin years later. The likelihood and severity are greater with more frequent dosing, but all doses, even one drop daily, can cause this side effect. The IOP increase almost invariably resolves when the drops are stopped.
Table 19.1 Topical corticosteroid drugs
Periocular Corticosteroid Injections
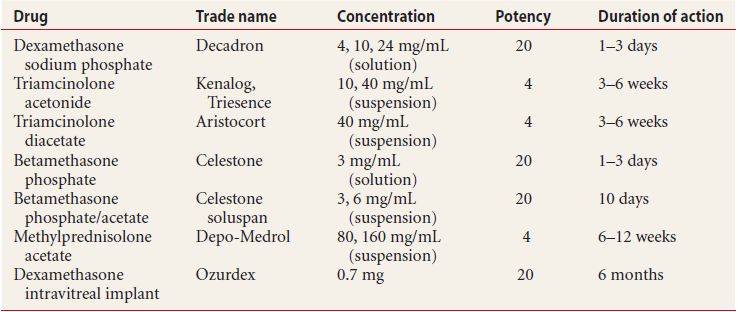
Once we have found topical steroids safe in a particular patient, we consider giving a periocular steroid injection for patients with significant residual inflammation. This modality of administration is useful for a sustained, local anti-inflammatory effect. A comparison of the different injectable corticosteroids is included in Table 19.2.
Table 19.2 Injectable corticosteroid preparations
- Ophthalmic uses
- Anterior uveitis that has responded to topical corticosteroids.
- Intermediate and posterior uveitis.
- Nonnecrotizing scleritis.
- Prophylactic inflammatory coverage in patients undergoing surgery with a previous history of uveitis.
- Anterior uveitis that has responded to topical corticosteroids.
- Administration
- Triamcinolone acetonide 40 mg/mL is the most commonly injected drug for ocular inflammation. For periocular injection, the commercially available product is manufactured for injection in joints and soft tissues, and ophthalmologic use is considered “off label.” Triamcinolone acetonide also comes in a 10 mg/mL formation, but we find no use for it since it requires a larger volume to get the same effect. In order to administer the drug
- A 27 gauge (g) needle on a 1 or 3 mL syringe is used to inject the drug, and it is important to draw the drug up out of the bottle into the syringe with a 27 g needle as well (if a larger needle is used to draw it up, large drug particles end up in the syringe and get caught in the 27 g needle on the way out). Lidocaine or any other injected local anesthetic is not necessary when injecting periocular triamcinolone;
- After injection, the drug is visible as a white plaque on the sclera. It will exert pharmacologic activity as long as it is visible—usually several months, but this activity declines as the drug deposit slowly dissolves and shrinks, so patients’ disease activity may “overpower” the residual drug, and require reinjection even while some drug is still visible;
- The injection site will be scarred after periocular triamcinolone injection. It may be difficult to repeat the injection in the same spot;
- For uveitis, a typical periocular injection is 20 mg in 0.5 mL, but some practitioners will use up to 40 mg in 1 mL;
- For scleritis, a typical injection is 4 mg in 0.1 mL per affected quadrant of anterior sclera (superotemporal, inferotemporal, etc.).
- A 27 gauge (g) needle on a 1 or 3 mL syringe is used to inject the drug, and it is important to draw the drug up out of the bottle into the syringe with a 27 g needle as well (if a larger needle is used to draw it up, large drug particles end up in the syringe and get caught in the 27 g needle on the way out). Lidocaine or any other injected local anesthetic is not necessary when injecting periocular triamcinolone;
- Dexamethasone phosphate 4 mg/mL is often helpful for a strong immediate therapeutic “kick” in severe anterior uveitis. This drug is rapidly absorbed into the eye and periocular tissues, with the duration of efficacy less than 24 hours.
- A typical dose is 1 mg in 0.25 mL.
- It is a solution, so if given alone it may be injected through a 30 g needle. As with other injectable corticosteroids, its use in or around the eye is off label.
- Dexamethasone injections hurt, so be sure to combine it with lidocaine 0.1 mL in the same syringe and inject slowly, or give the lidocaine beforehand (we use lidocaine 1% or 2% with 1:200,000 epinephrine).
- Dexamethasone can be combined with triamcinolone to enhance the immediate anti-inflammatory effect. To do this, we take a 1 mL syringe with a 27 g needle, draw triamcinolone 20 mg in 0.5 mL, then draw dexamethasone 1 mg in 0.25 mL into the same syringe, and lastly draw lidocaine 0.1 mL as well, place a new 27 g needle, and inject slowly.
- A typical dose is 1 mg in 0.25 mL.
- Betamethasone phosphate/acetate 6 mg/mL, widely known as Celestone, is an injectable medication. Its main advantage is that it is as potent as dexamethasone but its therapeutic effect lasts 1 to 2 weeks: long enough to get control of inflammation, but not long enough to create serious side effects. Here again, its use is off label.
- Betamethasone is partly a suspension, so it is drawn up and injected through 27 g needles. Betamethasone injections are quite painful, and this irritating effect often outlasts lidocaine. Add 0.2 ml of lidocaine 1% to 2% combined with bupivicaine 0.5% to 0.75% in the syringe before injecting.
- We are unaware of anyone combining betamethasone with another corticosteroid for injection.
- Betamethasone is partly a suspension, so it is drawn up and injected through 27 g needles. Betamethasone injections are quite painful, and this irritating effect often outlasts lidocaine. Add 0.2 ml of lidocaine 1% to 2% combined with bupivicaine 0.5% to 0.75% in the syringe before injecting.
- Methylprednisolone acetate 80 mg/mL (Depo-medrol) is a suspension that can be injected around the eye just like triamcinolone (see above). It lasts several months longer, but the injection sites tend to scar more densely than with other drugs.
- Side effects
- IOP elevation, as described for topical corticosteroids. In general, this ocular hypertension can be treated with drops. Most practitioners find that about one third of patients will exhibit a steroid response within 6 weeks (a tiny percentage will have a very brisk IOP elevation almost immediately after starting the drug), one third will have a delayed-onset steroid response after 6 weeks, and one third will be unaffected. Occasionally, the high IOP may be persistent and severe enough to require removal of repository triamcinolone or methylprednisolone.
- Posterior subcapsular cataracts, as with topical steroids. We may opt to avoid repeat injections for this reason in children, particularly in the amblyogenic age group.
- Hyperglycemia in patients with diabetes, which will persist for approximately 24 hours after dexamethasone injection or a bit more than 48 hours after triamcinolone injection. For patients in whom systemic absorption should be minimized, subconjunctival injections are superior to peribulbar injections.
- Injection site scarring may complicate repeat injection in the same spot.
- Subconjunctival hemorrhage, especially using the subtenon or subconjunctival approach. We avoid the cardinal clock hours (12, 3, 6, 9) when giving periocular injections, since trauma to branches of the anterior ciliary arteries that run in these clock hours can cause marked hemorrhage. Particularly, dexamethasone injections cause subconjunctival hemorrhages and patients should be warned beforehand to expect this.
- Pain, when injecting dexamethasone or betamethasone. These drugs need to be mixed with lidocaine when injected. Non-preserved triamcinolone may be slightly more uncomfortable than the standard commercially available formulation.
- Inadvertent penetrating globe trauma is always a risk factor.
- IOP elevation, as described for topical corticosteroids. In general, this ocular hypertension can be treated with drops. Most practitioners find that about one third of patients will exhibit a steroid response within 6 weeks (a tiny percentage will have a very brisk IOP elevation almost immediately after starting the drug), one third will have a delayed-onset steroid response after 6 weeks, and one third will be unaffected. Occasionally, the high IOP may be persistent and severe enough to require removal of repository triamcinolone or methylprednisolone.
- Medicolegal considerations
- Patients should be made fully aware that the use of corticosteroids for periocular injection is off label. These drugs are produced for the treatment of other diseases, and their use in ophthalmology is not approved by the U.S. Food and Drug Administration (FDA). This discussion should be documented in the medical record.
Intraocular Corticosteroid Injections
- Ophthalmic uses
- Severe posterior uveitis
- Macular edema
- Severe posterior uveitis
- Administration
- Triamcinolone acetonide 40 mg/mL is very effective in treating macular edema or severe uveitis. One formulation (Triesence, Alcon, Fort Worth, TX) is approved by the U.S. FDA. A typical injection is 2 to 4 mg in 0.05 to 0.1 mL injected through the pars plana, although larger amounts can be given in surgery, where the IOP is easily controlled.
- Dexamethasone intraocular injections are safe in doses up to 0.4 mg. The effect tends to be very short lived; however, this is generally only performed in the surgical setting, when closing cases in which a lot of postoperative inflammation is expected.
- Triamcinolone acetonide 40 mg/mL is very effective in treating macular edema or severe uveitis. One formulation (Triesence, Alcon, Fort Worth, TX) is approved by the U.S. FDA. A typical injection is 2 to 4 mg in 0.05 to 0.1 mL injected through the pars plana, although larger amounts can be given in surgery, where the IOP is easily controlled.
- Side effects
- IOP elevation is seen in about a third to half of patients. It almost always resolves as the drug dissolves, which takes anywhere between 4 to 10 weeks in non-vitrectomized eyes. This effect occurs much less in vitrectomized eyes, because the drug washes out of the eye much more quickly, usually after 2 weeks.
- Posterior subcapsular cataracts are common, the frequency ranging from 45% to 81% of eyes in published studies. Steroid responders are much more likely to develop steroid-related cataracts.
- Endophthalmitis is a potential complication of all intraocular procedures. The risk of this complication is under 1%. We minimize the risk by prepping the eyelids and conjunctiva with betadine, establishing a sterile field, using new bottles of drug each day, and swabbing the bottle tops with alcohol before each use.
- Pseudoendophthalmitis presents as a dense vitritis with hypopyon presenting 1 to 3 days following intravitreal injection. The examiner will recognize it because the anterior chamber will show a dense cellular reaction with almost no flare (as opposed to the fibrinoid reaction characteristic of infectious endophthalmitis). It clears without therapy over 1 to 8 weeks. Pseudoendophthalmitis was fairly common before the availability of non-preserved triamcinolone, but is see much less often now.
- Retinal toxicity is an devastating complication when injecting commercially available betamethasone and methylprednisolone into the vitreous, due to toxicity of the drug vehicle.
- Pain. Difficulty achieving local anesthesia should be anticipated when repeating pars plana injections in the same clock hour. For this reason, we rotate the injection site around different clock hours when administering repeat injections.
- Subconjunctival hemorrhage at the injection site, which tends to be mild.
- IOP elevation is seen in about a third to half of patients. It almost always resolves as the drug dissolves, which takes anywhere between 4 to 10 weeks in non-vitrectomized eyes. This effect occurs much less in vitrectomized eyes, because the drug washes out of the eye much more quickly, usually after 2 weeks.
Intravitreal Implants
Dexamethasone Intravitreal Implant (Ozurdex)
- Opthalmic uses
Dexamethasone is one of the most potent corticosteroid formulations and is very widely used in clinical medicine. Its clinical application in ophthalmology has been limited by its rapid clearance from the eye. A recent development in uveitis is the production and FDA approval of a biodegradable sustained-release dexamethasone intraocular implant (Ozurdex), which is effective in treating intraocular inflammation. Ozurdex was initially FDA approved for the treatment of macular edema associated with branch and central retinal vein occlusion.
- Administration
Ozurdex makes use of a solid polymer delivery system containing 0.7-mg dexamethasone that releases the drug over a 6 months period. Initially, the implant delivers a high-dose dexamethasone in the first 30 days with a sustained slower release in the following 5 months. The device comes preloaded in a single-use injector, the tip of which approximates the size of a 23-gauge needle. It can be injected through the pars plana as an office procedure, although the large size of the injector tip necessitates either biplanar injection or some modification of the standard technique.
- Clinical effects
The efficacy of ozurdex in the treatment of intermediate and posterior uveitis was demonstrated in a 225-patient multi center clinical trial comparing control with 0.35-mg and 0.7-mg dexamethasone. By week 6, both concentrations of ozurdex demonstrated clinically significant decrease in vitreous haze with an increased response at the higher dose, with 9% of the control vs. 43% of the 0.7-mg ozurdex patients with zero vitreous haze on examination. Ozurdex also demonstrated by 3 weeks 3 lines of visual acuity improvement in 33% of ozurdex patients compared to 4% of controls. This clinically significant visual improvement is maintained through week 26 of treatment. In addition, ozurdex treatment demonstrated significant and clinically relevant improvement in the quality of life measured by the National Eye Institute Visual Functioning Questionnaire-25.
- Side effects
Side effects are similar to all intraocular corticosteroid therapies and include IOP elevation during the 6-months life span of the implant and posterior subcapsular cataracts. Intraocular injections invariably incur the risk of endophthalmitis, conjunctival hemorrhage, and pain.
Note: On the completion of this manuscript, Ozurdex by Allergan is currently awaiting FDA approval for the treatment of uveitis. Ozurdex is expected to be FDA approved after publication of this handbook in March 2010.
- Medicolegal considerations
Patients should be made fully aware that intraocular corticosteroid injection carries the risk of acute damage to the intraocular structures during the injection procedure, as well as cataract and IOP elevation over the long term. We document this discussion carefully.
Oral Corticosteroids
- Ophthalmic uses
- Severe bilateral or recalcitrant uveitis. We use this if patients cannot tolerate periocular injections, or if disease is bilateral.
- Scleritis. Systemic corticosteroids are first-line therapy for scleritis.
- Trial therapy to prove corticosteroid efficacy. It is sometimes necessary or helpful to confirm that a patient’s inflammation is in fact immune mediated (i.e., not infectious) and thus treatable with corticosteroids before administering periocular corticosteroid repository injections. A short course of oral corticosteroids is useful for establishing this, without incurring the long-term risks associated with periocular injections.
- Severe bilateral or recalcitrant uveitis. We use this if patients cannot tolerate periocular injections, or if disease is bilateral.
- Administration
- Prednisone and prednisolone are available orally as pills in multiple sizes (1, 2.5, 5, 10, 20, 50 mg for prednisone. 5 mg for prednisolone) and as a liquid suspension (5 mg/5 mL for prednisone and 5 and 15 mg/mL for prednisolone). These two drugs are therapeutically equivalent and have the same enormous side effect profile. Prednisone is pharmacologically inactive and is converted at a 1:1 ratio to the active compound prednisolone.
- A starting dose of 1 mg per kg body weight should be used, which can be taken as a single daily dose after a substantial morning or noontime meal. This should be continued for at least a week before reevaluating the patient.
- Oral corticosteroids cause adrenal suppression after 1 week of therapy, and so after 7 days the dose should be lowered gradually to avoid adrenal insufficiency. The speed of the taper depends on the clinical circumstances, but a rapid taper would involve decreasing the dose by 10 mg each day (50 mg one day, 40 mg the next, etc.) until discontinuation. This approach is common when oral corticosteroids have been used to achieve immediate control, and a periocular injection is then given for longer duration of disease control. An example of a slower taper would be decreasing the daily prednisone dose by 10 mg every week, while monitoring to see how low the dose can be lowered before the inflammation recurs.
- If one anticipates continuing oral corticosteroid therapy at any dose for more than 2 weeks, we generally use concomitant bisphosphonate therapy. A basic prescription would be alendronate 10 mg per day. Note that bisphophonates are contraindicated in girls and in women of childbearing age.
- A starting dose of 1 mg per kg body weight should be used, which can be taken as a single daily dose after a substantial morning or noontime meal. This should be continued for at least a week before reevaluating the patient.
- Dexamethasone may be given orally, and is also available in multiple formulations.
- The drug is 6.25 times as potent as prednisone, so an equivalent starting dose is 0.16 mg/kg/day, with the same side effect precautions.
- Methylprednisolone is available orally as Medrol, although it has no advantage over prednisone/prednisolone and tends to be more expensive.
- This drug is 1.25 times as potent as prednisone. Thus, it is dosed at 0.8 mg/kg/day.
- It is available in a user-friendly “Medrol dose pack” in which the daily doses are packaged individually in tapering doses. Note that the tapering regimen in the Medrol dose pack, however, is too rapid to be practically useful in treating uveitis or scleritis, so we find little use for it.
- This drug is 1.25 times as potent as prednisone. Thus, it is dosed at 0.8 mg/kg/day.
- Prednisone and prednisolone are available orally as pills in multiple sizes (1, 2.5, 5, 10, 20, 50 mg for prednisone. 5 mg for prednisolone) and as a liquid suspension (5 mg/5 mL for prednisone and 5 and 15 mg/mL for prednisolone). These two drugs are therapeutically equivalent and have the same enormous side effect profile. Prednisone is pharmacologically inactive and is converted at a 1:1 ratio to the active compound prednisolone.
- Side effects
This topic could fill an entire library, since all patients experience side effects at some point in the course of oral steroid therapy. Very common early effects are the following:
- Mood alterations. Patients will complain of this after a few days of therapy, and it will resolve as the drug is tapered and discontinued.
- Cushingoid appearance. The onset of this varies from weeks to months, and it also is dose dependent, and will resolve when the drug is tapered and stopped.
- Osteopenia, as described above.
- Hyperglycemia. This side effect is expected in patients with diabetes, and modifications to their drug regimens should be made as necessary. We find it very helpful to communicate with our patients’ primary care physicians in these circumstances.
- Peptic ulcers. Patients with preexisting ulcers are poor candidates for oral corticosteroid therapy.
- Posterior subcapsular cataracts. These occur after prolonged therapy for considerably more time than most ophthalmologists use. They stop progressing if the drug is stopped.
- IOP elevation. Some patients will be sensitive to this, and it is important to keep this side effect in mind when evaluating patients who present with high IOP and who may be taking oral corticosteroids as treatment of non-ocular conditions.
In light of these many side effects, we are weary of using oral corticosteroids for prolonged periods, and if we anticipate needing more than 8 weeks of therapy, we almost invariably use either periocular depot injections, systemic immunomodulatory therapy, or both.
- Mood alterations. Patients will complain of this after a few days of therapy, and it will resolve as the drug is tapered and discontinued.
- Medicolegal considerations
Ophthalmologists have been held liable for maintaining patients on oral corticosteroids without documenting consideration of the side effects. Since it is easy to lose track, visit to visit, of how long patients have been taking their medications, we never prescribe refills with our oral corticosteroid prescriptions, and we review patients’ side effects and tolerance with every prescription renewal.
Intravenous Corticosteroids
- Ophthalmic uses
We consider intravenous corticosteroids extreme therapy, only to be used on uveitis patients in certain circumstances:
- Intraoperatively in patients at substantial risk of postoperative inflammation.
- Cases of imminent danger of visual loss and/or extreme pain (usually due to scleritis)
- Intraoperatively in patients at substantial risk of postoperative inflammation.
- Administration
- Methylprednisolone sodium succinate can be given as a bolus of 1,000 mg intravenously over 2 hours. This can be repeated daily to complete 3 days of therapy. For outpatients, this therapy requires the services of an emergency room or a drug infusion center. The clinical effects of the infusion generally manifest within 24 hours, although complete resolution should not be anticipated. We usually interpret failure to improve after 3 days of IV therapy as a need to reevaluate our diagnosis and consider infectious etiologies.
- Dexamethasone can be administered intravenously as a 200 mg bolus in the same manner as methylprednisolone. For both methylprednisolone and dexamethasone, one has the option of splitting the drug into half-dose boluses of 500 mg or 100 mg, respectively. We find little use for this approach, reasoning that full dose boluses are equally well tolerated, and that if we are putting the patient through the inconvenience of an infusion, then we should provide them with the full benefit.
- Methylprednisolone sodium succinate can be given as a bolus of 1,000 mg intravenously over 2 hours. This can be repeated daily to complete 3 days of therapy. For outpatients, this therapy requires the services of an emergency room or a drug infusion center. The clinical effects of the infusion generally manifest within 24 hours, although complete resolution should not be anticipated. We usually interpret failure to improve after 3 days of IV therapy as a need to reevaluate our diagnosis and consider infectious etiologies.
- Side effects
As a rule, almost all individuals can tolerate even very high doses of corticosteroids for a short duration, and thus intravenous corticosteroid boluses are generally well tolerated. In addition to the previously mentioned side effects of systemic steroids, we anticipate the following:
- Hyperglycemia in diabetic patients, and blood sugar monitoring with insulin sliding scales used as needed.
- Hypertension during infusions, which infusion centers generally know to look out for.
- Hyperglycemia in diabetic patients, and blood sugar monitoring with insulin sliding scales used as needed.
Corticosteroids in Pregnancy
In practice, ocular inflammation in pregnant women is rare, and many women with long histories of chronic uveitis observe that their disease becomes inactive during pregnancy, and will return afterward. If inflammatory control is necessary, consider the following:
- For immediate control
- Prednisone and prednisolone are generally safe to use, barring other contraindications like diabetes.
- Dexamethasone and betamethasone are the only corticosteroids that cross the placenta, and so we avoid these agents in all forms in pregnant women.
- Prednisone and prednisolone are generally safe to use, barring other contraindications like diabetes.
- For long-term control
- Inflammation limited to the anterior segment can be controlled indefinitely with prednisolone eyedrops.
- Posterior segment inflammation, however, cannot be controlled with topical medications, and periocular triamcinolone injections are not universally acknowledged as safe in pregnancy. Intravitreal triamcinolone, however, is theoretically safer, since the volume of drug is much less and is limited to the interior of the eye.
- Inflammation limited to the anterior segment can be controlled indefinitely with prednisolone eyedrops.
MAINTAINING LONG-TERM CONTROL
Corticosteroids for Long-Term Control: Eyedrops, Injections, and Implants
In some cases, corticosteroids are suitable for long-term control. The role of each modality along these lines is slightly different.
- Corticosteroids eyedrops are sometimes used for immediate control, after which a slow taper is followed by prolonged or permanent disease quiescence.
- Periocular triamcinolone injections can sometimes quiet an eye for several months. Patients like this may undergo three or four injections per year to maintain long-term control, and are often well served with such a regimen. It may be expected that they might require treatment of cataracts and glaucoma after a few years.
- Dexamethasone intravitreal implant (Ozurdex) is a FDA approved biodegradable implant for the treatment of intermediate and posterior uveitis. Dexamethasone is released into the vitreous cavity over a six months period. IOP elevation and cataract formation should be expected.
- Fluocinolone acetonide implants (Retisert) (0.59 mg) have been found to be very effective in reducing the frequency and severity of uveitis recurrences and the amount of adjunctive treatment needed. Typically, the duration of action is about 2 years. More than half of recipients sustain an increase in IOP more than 10 mm Hg, and cataracts are invariably expected to worsen over time.
Immunomodulatory Drugs
While some patients can maintain long-term control of their ocular inflammation with corticosteroids alone, patients with chronic disease of any severity often benefit from steroid sparing immunomodulatory drugs. Chemotherapeutic anticancer agents, immunosuppressive drugs, and “biologic” drugs (usually synthesized antibodies or cytokine receptors) can play a useful role in the long-term management of uveitis and scleritis. They can eliminate the need for a prolonged corticosteroid course, which often is fraught with an even greater side effect profile and more immunosuppression than these drugs.
INDICATIONS FOR IMMUNOMODULATORY DRUGS
For patients needing long-term control of their ocular inflammation, we consider using immunomodulation in three different scenarios:
- Steroid intolerance, usually due to either IOP elevation or cataract formation.
- Disease in multiple organ systems, such as children with juvenile idiopathic (juvenile rheumatoid) arthritis who have iritis and arthritis, or patients with sarcoid uveitis who have active pulmonary (or any bodily) inflammation.
- Certain very severe uveitic entities are an indication for immediate immunomodulatory therapy, namely
- Sympathetic ophthalmia
- Vogt-Koyanagi-Harada syndrome
- Behcet disease
- Rheumatoid scleritis
- Sympathetic ophthalmia
FACTORS IN CHOOSING AN IMMUNOMODULATORY DRUG
Practitioners vary in their approach to choosing immunosuppressives and when to use which drug. Nearly all, however, would agree that four factors merit consideration:
- Severity of the inflammation.
- Type of inflammation, that is, uveal tract inflammation, vasculitis, or scleritis/keratitis (we group scleritis and keratitis together for these purposes).
- Associated systemic diseases, or in idiopathic inflammation, laboratory findings that may point toward treatment for one sort of systemic disease or another (the presence of antinuclear antibodies, for example, would cause us to choose drugs that treat systemic lupus erythematosis [SLE], while elevated rheumatoid factor antibodies would call for drugs for rheumatoid arthritis).
- Patient age and family planning issues.
BASIC GROUND RULES FOR IMMUNOMODULATORY DRUGS
- Patients are reasonable candidates for these agents if they are capable of adhering to sometimes complicated treatment and laboratory regimens, they understand the risks and benefits of therapy, and they want to take the drug.
- The pros and cons of immunomodulatory therapy versus corticosteroids must be carefully considered. While the patient can avoid the side effects of corticosteroids by using this therapy, these drugs all carry their own side effects, they take several weeks to show an effect, and they are less reliably effective than corticosteroids. They are not approved by the FDA for eye disease, and all use is considered “off label.” Document this discussion in the patient’s chart, and consider an informed consent.
- We never try to convince hesitant patients to use immunomodulatory therapy, since we find that reticent patients who do start the agents then tend to blame the drug for nearly all of their adverse symptoms and ailments. In our view, the patient’s anxiety and the medicolegal risk to the doctor outweigh the potential benefits of this form of therapy.
- In following, patient anxiety is a sufficient reason to stop an immunosuppressive agent. We never insist that a patient continue these drugs if he or she believes that it may be causing an unpleasant side effect (no matter how implausible the patient’s claim seems). While we feel free to give our opinion on the patient’s assertion, ultimately the decision to stop the drug rests squarely with the patient or his or her parents.
- Patients taking immunosuppression should receive killed influenza vaccines, and any other vaccines that they receive must also be killed. These patients should NEVER receive live vaccines.
- Male and female patients taking these drugs should be using birth control. We document this discussion and the method of birth control being used. Patients should wait for 3 months after stopping these drugs before attempting to conceive.
- Standard baseline laboratory tests for immunosuppression are a complete blood count, CBC, hepatic and renal function tests. For cyclophosphamide, we also include urinalysis. For cyclosporine and tacrolimus, we include blood pressure.
- Always keep the patient’s internist or primary care doctor well informed regarding your use of these drugs. You will very likely need this colleague’s help if your patient develops drug-related complications.
- Patients who have even minor infections while taking immunosuppressive drugs should stop the drug until their symptoms have resolved. We enlist our internist and pediatrician colleagues in getting these ailments monitored and treated promptly.
- In following, patient anxiety is a sufficient reason to stop an immunosuppressive agent. We never insist that a patient continue these drugs if he or she believes that it may be causing an unpleasant side effect (no matter how implausible the patient’s claim seems). While we feel free to give our opinion on the patient’s assertion, ultimately the decision to stop the drug rests squarely with the patient or his or her parents.
IMMUNOMODULATORY DRUGS AND THEIR USES
In this section, we discuss the more common immunomodulatory drugs used in uveitis management.
Methotrexate
- Pharmacology
- Methotrexate inhibits DNA replication by blocking the action of dihydrofolate reductase.
- The immunosuppressive effect appears to involve a number of other biochemical pathways in addition, none of which are as clearly understood.
- Methotrexate inhibits DNA replication by blocking the action of dihydrofolate reductase.
- Ophthalmic uses
- Chronic uveitis or scleritis/keratitis with a negative workup. The most common indications are steroid intolerance. A fairly typical patient is one who is experiencing early cataracts or IOP elevation from topical or periocular corticosteroids, or inflammation in the setting of systemic disease.
- Sarcoidosis, rheumatoid arthritis, systemic lupus erythematosus, or juvenile idiopathic arthritis–associated inflammation. The drug has a long track record of safety in children, and does not impair development.
- Chronic uveitis or scleritis/keratitis with a negative workup. The most common indications are steroid intolerance. A fairly typical patient is one who is experiencing early cataracts or IOP elevation from topical or periocular corticosteroids, or inflammation in the setting of systemic disease.
- Administration
- The drug is taken weekly. We typically start with 15 mg per week in adults, or 0.5 mg/kg/week in children, and we also prescribe folic acid 1 mg per day to minimize side effects.
- One should allow 8 weeks for the drug to take effect. A common approach is to start oral corticosteroids or give a periocular corticosteroid injection when starting methotrexate, anticipating that the immunosuppressive drug will be taking effect as the corticosteroids are tapered or the injection begins to wear off. If after 8 weeks, we still observe inadequate effect from the drug, we increase the dose by 5 mg per week (to 20 mg per week, or up to 0.65 mg/kg/week in children) and wait a further 6 weeks for drug effect. If still not effective, we find another drug.
- Occasionally, methotrexate 20 mg per week will have a positive but incomplete effect, in which case we increase the drug still further. The maximum dose is 25 mg per week (or up to 0.8 mg/kg/week in children).
- If the drug is working, we usually recommend that patients plan on taking it for minimum of 2 years before discontinuing it and monitoring for disease recurrence.
- The drug is taken weekly. We typically start with 15 mg per week in adults, or 0.5 mg/kg/week in children, and we also prescribe folic acid 1 mg per day to minimize side effects.
- Ancillary tests
- At baseline, 2 weeks, 4 weeks, and every 6 to 8 weeks thereafter, we check:
- Alanine aminotransferase (ALT) and aspartate aminostransferase (AST) If the AST or ALT becomes elevated in excess of 50% over the upper limit of normal, lower the drug dose by 2.5 mg per week, and recheck the labs in 4 weeks. If the AST or ALT does not normalize, then stop the drug. Obviously, marked transaminase elevation (3× the upper limit of normal) at any time necessitates stopping the drug.
- Creatinine should be normal before starting methotrexate, and should not be affected by methotrexate itself, although an increase for any reason merits stopping the drug.
- White blood cell (WBC) count may decrease slightly when taking methotrexate, although a WBC count below 4,000 cells/μL indicates lowering the drug dose.
- Alanine aminotransferase (ALT) and aspartate aminostransferase (AST) If the AST or ALT becomes elevated in excess of 50% over the upper limit of normal, lower the drug dose by 2.5 mg per week, and recheck the labs in 4 weeks. If the AST or ALT does not normalize, then stop the drug. Obviously, marked transaminase elevation (3× the upper limit of normal) at any time necessitates stopping the drug.
- At baseline, 2 weeks, 4 weeks, and every 6 to 8 weeks thereafter, we check:
- Side effects
- Myalgias and loss of appetite for a few days after the first few doses. If this symptom persists, lowering the drug by 2.5 mg per week will often alleviate it.
- Oral ulcers are a severe side effect that merits the discontinuation of methotrexate.
- GI upset.
- Transaminase elevation (roughly 15% of patients) is the most common reason for stopping the drug. Patients should refrain from alcohol consumption while on methotrexate.
- Pneumonitis is also a known side effect. All patients on methotrexate who develop a cough need an evaluation urgently.
- Birth defects. Methotrexate is teratogenic, and patients (both men and women) should be on birth control while on the drug.
- Beta-lactam antibiotics (penicillins) are contraindicated in patients taking methotrexate.
- Myalgias and loss of appetite for a few days after the first few doses. If this symptom persists, lowering the drug by 2.5 mg per week will often alleviate it.
Azathioprine (Imuran)
- Pharmacology
- This inhibitor of purine formation has been around since the 1960s, and is generally stronger than methotrexate. It is probably the most versatile drug in the immunosuppressive armamentarium for uveitis.
- Ophthalmic uses
- Uveitis or scleritis that has not responded to methotrexate.
- Retinal vasculitis.
- Uveitis or scleritis that has not responded to methotrexate.
- Administration
- We start at 50 mg in adults. The drug is taken daily in 1 or 2 doses, and usual dose is 2 mg/kg/day. We usually split the dose (morning and evening) when it exceeds 75 mg. Azathioprine comes as 50 mg tablets, which can be split.
- In order to establish the appropriate dose, be prepared to titrate the drug against the WBC count. Start at 50 mg per day, and recheck the labs in 1 week. If the WBC count drops at this low dose, stop the drug. If not, increase to 75 mg per day and recheck labs again in 1 to 2 weeks. Repeat this cycle up to a dose of approximately 2 mg/kg/day. If the labs hold steady at this dose for 1 to 2 weeks, check again after a month, and if still stable then check every 6 to 8 weeks. If the WBC count drops below 5.0 (× 1,000 cells/μL) at any point, do not increase the dose. If it drops below 4.0, decrease the dose by 25 mg and recheck in 1 week.
- Allow 8 weeks for the drug to take effect at the maximum or highest tolerated dose—one should be able to either taper daily corticosteroids or allow a periocular injection to wear off without disease recurrence.
- If there is inadequate effect, or the drug is not well tolerated, then stop the drug or add cyclosporine.
- We start at 50 mg in adults. The drug is taken daily in 1 or 2 doses, and usual dose is 2 mg/kg/day. We usually split the dose (morning and evening) when it exceeds 75 mg. Azathioprine comes as 50 mg tablets, which can be split.
- Ancillary tests
- Check at baseline, then every 1 to 2 weeks until dose is established, then every 6 to 8 weeks.
- WBC See above.
- AST and ALT
- Thiopurine methyltransferase We check this at baseline to predict a patient’s liver tolerance for this drug. Higher values indicate a better prognosis.
- WBC See above.
- Check at baseline, then every 1 to 2 weeks until dose is established, then every 6 to 8 weeks.
- Side effects
- Liver and bone marrow toxicity.
- Nausea—by far the most common reason for discontinuation.
- Secondary malignancy, a risk that has been established in renal transplant recipients, but not in those with non-transplant patients. In any case, we avoid the drug in children for this reason.
- Premature and small for gestational age babies. We avoid azathioprine in pregnancy, although our internal medicine colleagues sometimes do not.
- Drug interactions. Allopurinol and azathioprine are a potentially fatal drug combination.
- Liver and bone marrow toxicity.
Mycophenolate Mofetil (Cellcept)
- Pharmacology
- This drug impairs de novo purine synthesis by blocking the enzyme inosine monophosphate dehydrogenase, forcing cells to use the DNA salvage pathway, which lymphocytes do not have. It thus lowers lymphocyte levels.
- Ophthalmic uses
- Severe uveitis or retinal vasculitis. We often use this as first line treatment.
- Scleritis with an elevated ANA. This drug is used to treat SLE.
- Idiopathic uveitis. We use it as a second line drug in patients with idiopathic uveitis in whom methotrexate has not been effective.
- Severe uveitis or retinal vasculitis. We often use this as first line treatment.
- Administration
- Mycophenolate comes as 250 or 500 mg tablets. Start with 500 mg twice daily for the first week, then double to the typical dose in adults of 1,000 mg twice daily.
- Allow 8 weeks for the drug to take effect. If disease recurs when tapering daily corticosteroids or after a periocular corticosteroid injection wears off, then increase the dose in 500 mg per day increments.
- Maximum dose is 3 g daily, after which there is a greater risk of leukopenia and opportunistic infections. The full dose in children is 600 mg per m2 body surface area. We do not increase the dose in children (we find another drug).
- The drug should be taken on an empty stomach.
- Mycophenolate comes as 250 or 500 mg tablets. Start with 500 mg twice daily for the first week, then double to the typical dose in adults of 1,000 mg twice daily.
- Ancillary tests
- CBC. Check at baseline, 2 weeks, 4 weeks, then every 6 to 8 weeks. The WBC count should drop somewhat after 6 weeks, particularly the lymphocyte portion. Stop the drug if absolute lymphocyte count goes below 750 cells/μL.
- Liver function tests (LFTs). Check at baseline, then every 2 to 3 months.
- CBC. Check at baseline, 2 weeks, 4 weeks, then every 6 to 8 weeks. The WBC count should drop somewhat after 6 weeks, particularly the lymphocyte portion. Stop the drug if absolute lymphocyte count goes below 750 cells/μL.
- Side effects
- Bone marrow and liver toxicity.
- Secondary malignancy, but much less so than azathioprine.
- Gastrointestinal upset. The drug causes loose stools when patients first start it. This drug is otherwise very well tolerated, with gastrointestinal upset being the only occasional complaint.
- Bone marrow and liver toxicity.
Cyclosporine (Neoral)
- Pharmacology
- This drug decreases lymphocyte activity and proliferation by inhibiting calmodulin, an intracellular enzyme involved in interleukin-2 synthesis, as well as by blocking the receptors for T-cell activation.
- Ophthalmic uses
- Severe uveitis or retinal vasculitis. We have had some success in using it as a first-line single agent, and we generally end up combining it with methotrexate, azathioprine, or mycophenolate. One reasonable approach is to start cyclosporine after one of these agents has had an incomplete effect, and if cyclosporine alone also works poorly, then add back one of these agents.
- Administration
- The drug comes as 25 and 100 mg gel caps. We insist on the Neoral formulation, which is a modification of the earlier version of the drug, called Sandimmune. The drug is given in split doses, 12 hours apart. If we are using the drug as a single agent, we start at 4 mg/kg/day, and if we are combining the drug we use 2.5 mg/kg/day.
- Maximum dosage is 5 mg/kg/day.
- Allow 8 weeks for the drug to take effect, as with the other agents discussed above. Increase the drug in 1 mg/kg/day increments up to just over 4 mg/kg/day as tolerated before declaring the drug a failure. One can add methotrexate, azathioprine, or mycophenolate if this occurs.
- Maximum dosage is 5 mg/kg/day.
- The drug comes as 25 and 100 mg gel caps. We insist on the Neoral formulation, which is a modification of the earlier version of the drug, called Sandimmune. The drug is given in split doses, 12 hours apart. If we are using the drug as a single agent, we start at 4 mg/kg/day, and if we are combining the drug we use 2.5 mg/kg/day.
- Ancillary tests
Check labs at baseline, 2 and 4 weeks, and every 6 to 8 weeks:
- CBC. Avoid low WBC counts, which are unusual with this drug.
- Creatinine. Pay attention to the baseline creatinine. If this rises more than 30%, then decrease the drug by 1 mg/kg/day and recheck after a month and be sure that the creatinine normalizes. If not, lower the drug again. If the creatinine remains elevated at a daily dose of 2.5 mg per kg, then stop the drug.
- Calcium and Magnesium. Significant decreases warrant stopping the drug.
- Blood pressure. Check it at each visit. If blood pressure rises over 140/90, then make the same modifications or get help for lowering the blood pressure pharmacologically.
- CBC. Avoid low WBC counts, which are unusual with this drug.
- Side effects
- Nephrotoxicity.
- Hypertension.
- Hirsutism.
- Gingival hyperplasia.
- Drug interactions. A very large number of drugs interact with cyclosporine because it is metabolized by the CYP450 enzyme, and we direct patients to the package insert and a variety of Web sites to check for drug interactions. Grapefruit and grapefruit juice also interfere with this drug’s metabolism.
- Nephrotoxicity.
Tacrolimus (Prograf, Formerly FK 506)
- Pharmacology
- This drug is a close cousin of cyclosporine, working through the same mechanism by decreasing lymphocyte activity and proliferation.
- Ophthalmic uses
- Experience with this drug in eye disease is limited. We would consider this drug in cases where cyclosporine affected some but incomplete control, and other therapeutic options were limited, or when cyclosporine caused electrolyte imbalance.
- Administration
- The drug is available as 1 and 5 mg capsules, and it is dosed once daily, 0.15 to 0.3 mg per day.
- Ancillary tests
- Check blood pressure, renal and hepatic functions, and a CBC before starting the drug, and then 2 and 4 weeks later, and every 8 weeks thereafter.
- Side effects
- Nephrotoxicity
- Hypertension
- Nephrotoxicity
Voclosporin (Luveniq)
- Pharmacology
- Voclosporin is a calcineurin inhibitor in the class of cyclosporine and is the first oral immunosuppressive drug to be approved in the United States for the treatment of uveitis. This agent has been demonstrated to be highly potent in animal models of autoimmune disease and uveitis. One main difference between voclosporin and earlier generation calcineurin inhibitors is this drug’s greater binding affinity for calcineurin phosphatase and its target molecule. The overall pharmacokinectic and pharmacodynamic properties of this agent suggest that it may be more potent and safer than current calcineurin inhibitors for long-term immunomodulatory therapy.
- Ophthalmic uses
- Voclosporin was recently evaluated in clinical trials as treatment of active posterior and anterior uveitis and in the maintenance and control of quiescent uveitis. Three different doses of voclosporin, 0.2, 0.4, and 0.6 mg/Kg twice daily, were evaluated. The 0.4-mg/kg twice-daily dose was superior to placebo in reducing active posterior segment inflammation at both 16 weeks and 24 weeks and effected a 50% reduction in the rate of inflammatory exacerbation by 26 weeks in subjects with medically controlled posterior segment disease. These differences were statistically significant.
- Administration
- The recommended dose is 0.4 mg/kg twice daily. Higher doses may be used and may be more effective, but they appear also to have more side effects and require more frequent laboratory testing.
Allow 4-6 weeks of therapy for the drug to show full efficacy.
- The recommended dose is 0.4 mg/kg twice daily. Higher doses may be used and may be more effective, but they appear also to have more side effects and require more frequent laboratory testing.
- Ancillary tests
- Check complete blood count (CBC) and serum creatinine at baseline and then every 4-6 weeks.
- Avoid low WBC counts to decrease the risk of systemic infection.
- Creatinine elevation necessitates a decreased dose.
- Blood pressure should be checked at each visit, and sustained significant elevation necessitates decreasing the voclosporin dose or the initiation of anti hypertensive therapy.
- Check complete blood count (CBC) and serum creatinine at baseline and then every 4-6 weeks.
- Side effects
- Lymphopenia
- Decreased renal function
- Increased blood pressure
- Hirsutism
- Gingival hyperplasia
- Lymphopenia
Note: On the completion of this manuscript, Luveniq by Lux Bioscience is currently awaiting FDA approval for the treatment of uveitis. Luveniq is expected to be FDA approved after publication of this handbook in March 2010.
Cyclophosphamide (Cytoxan)
- Pharmacology
- Along with chloramubucil (see below) this drug is an alkylating agent, with origins in the search for toxic chemical weaponry early last century. It is a powerful immunosuppressive, that works by cross-linking DNA and thereby preventing it from replicating.
- Ophthalmic uses
- Severe ocular inflammatory disease of any sort that has failed to respond to other drugs. In the United States, for the most part, it is a second or third line drug. Outside the United States, cyclophosphamide tends to be cheap and widely available, so many patients with severe uveitis benefit from it where other drugs are not available.
- Wegener granulomatosis and other systemic vasculitides, where it is used as a first line agent everywhere.
- Severe ocular inflammatory disease of any sort that has failed to respond to other drugs. In the United States, for the most part, it is a second or third line drug. Outside the United States, cyclophosphamide tends to be cheap and widely available, so many patients with severe uveitis benefit from it where other drugs are not available.
- Administration
- The drug can be given orally or intravenously. The oral formulation is available as 25 and 50 mg tablets. The oral route is generally more potent, but the side effects are more difficult to control. We therefore prefer to use the intravenous route where possible.
- If labs are unremarkable, start 1 mg/kg/day in a single dose. Titrate the dose in 25 mg per day increments until the WBC count is between 3,000 and 4,000 cells/μL.
- The intravenous formulation is given monthly. We usually use a starting dose of 1 g per m2 body surface area (some practitioners start with 650 mg per m2 and increase the dose by 25% increments). Use of this agent requires collaboration with a chemotherapy infusion center. Some infusion centers will have you write the infusion order, while some centers require a patient to be under the care of an oncologist or rheumatologist. All centers have very helpful standard regimens regarding piggy-backing normal saline, using acetaminophen concomitantly, etc.
- The ideal dose is one which causes a WBC nadir of 3500 cells/μL. Be sure to check the WBC nadir and a urinalysis 12 (TWELVE!) days after the infusion—this timing is important, since the WBC count changes rapidly.
- Once the optimal dose has been determined, we expect to see a clinical response within 3 weeks, otherwise we stop the drug. We continue the drug at that dose for 3 to 6 months depending on disease severity, patient tolerance, and cumulative dose. If no clinical response is evident despite a low white count, stop the drug.
- Cyclophosphamide is not by itself anti-inflammatory, so corticosteroids will be needed to bring the inflammation under control before the immunosuppressive effect will be apparent. One should be able to taper corticosteroids if cyclophosphamide is working. We try to discontinue oral corticosteroids when starting the drug to avoid the confounding effects on WBC, opting for IV pulse corticosteroids at the time of infusion.
- If using the IV route, give mesna, a drug that binds to the bladder-toxic metabolite and thereby lowers the risk of bladder toxicity. The mesna dose is 20% of the cyclophosphamide dose, given as a push or as a drip.
- Cyclophosphamide is not by itself anti-inflammatory, so corticosteroids will be needed to bring the inflammation under control before the immunosuppressive effect will be apparent. One should be able to taper corticosteroids if cyclophosphamide is working. We try to discontinue oral corticosteroids when starting the drug to avoid the confounding effects on WBC, opting for IV pulse corticosteroids at the time of infusion.
- The drug can be given orally or intravenously. The oral formulation is available as 25 and 50 mg tablets. The oral route is generally more potent, but the side effects are more difficult to control. We therefore prefer to use the intravenous route where possible.
- Ancillary tests
Check at baseline, and every 2 weeks:
- CBC. Titrate dose as above according to WBC. If given IV, check WBC exactly 12 days after the infusion. Remember that daily oral corticosteroids will increase a patient’s WBC count, and so if prednisone is used concomitantly, the WBC count will fall as prednisone is tapered. Paradoxically, this confounding effect often causes us to use more cyclophosphamide in patients taking prednisone.
- LFTs.
- Creatinine.
- Urinalysis.
- CBC. Titrate dose as above according to WBC. If given IV, check WBC exactly 12 days after the infusion. Remember that daily oral corticosteroids will increase a patient’s WBC count, and so if prednisone is used concomitantly, the WBC count will fall as prednisone is tapered. Paradoxically, this confounding effect often causes us to use more cyclophosphamide in patients taking prednisone.
- Side effects
- Hemorrhagic cystitis.
- Bladder cancer. We avoid cumulative doses greater than 100 g due to the risk of bladder cancer.
- Leukopenia.
- Gonadal dysfunction.
- Nausea. IV cyclophosphamide is highly emetogenic. Antiemetic regimens vary slightly, but we generally use
- An antiemetic regimen for 3 days, either ondansetron 8 mg orally every 8 hours starting at the time of infusion and continuing for 3 days or aprepitant 80 mg orally during the infusion and 40 mg per day for 2 more days.
- Dexamethasone 8 mg orally at the time of infusion (we often give more for an immediate anti-inflammatory “hit.”
- Lorazepam 1 to 2 mg orally at bedtime the evening after infusion and for two additional evenings.
- An antiemetic regimen for 3 days, either ondansetron 8 mg orally every 8 hours starting at the time of infusion and continuing for 3 days or aprepitant 80 mg orally during the infusion and 40 mg per day for 2 more days.
- Hemorrhagic cystitis.
- Hair loss.
- Fatigue.
- Cimetidine and allopurinol affect cyclophosphamide metabolism substantially enough that we avoid combinations with either of these drugs.
- Triamcinolone acetonide 40 mg/mL is the most commonly injected drug for ocular inflammation. For periocular injection, the commercially available product is manufactured for injection in joints and soft tissues, and ophthalmologic use is considered “off label.” Triamcinolone acetonide also comes in a 10 mg/mL formation, but we find no use for it since it requires a larger volume to get the same effect. In order to administer the drug
Chlorambucil (Leukeran)
- Pharmacology
- This drug is an alkylating agent similar to cyclophosphamide.
- Administration
- Chlorambucil is available as 2 mg tablets, and the usual effective dose is close to 0.1 mg/kg/day.
- To start the drug, confirm that baseline labs are normal and prescribe 4 mg per day for the first week.
- Based on the WBC, titrate the dose upward in 2 mg increments until the WBC count falls to 3,000 to 4,000 cells/μL. Here again, remember that prednisone or oral prednisolone will elevate the WBC count slightly, so if it is tapered, the chlorambucil dose may (paradoxically) need adjustment downward. A desired clinical effect would be the withdrawal of corticosteroids without disease recurrence.
- We continue the drug for 3 months if the desired effect is achieved. If patients’ disease is not controlled after 3 weeks despite a low white count, then find another drug.
- Chlorambucil is available as 2 mg tablets, and the usual effective dose is close to 0.1 mg/kg/day.
- Ancillary tests
- Check a CBC labs at baseline and then weekly until the WBC count is stable, then every 2 weeks.
- Side effects
- Bone marrow suppression
- Gonadal dysfunction
- Secondary malignancy
- Bone marrow suppression
Infliximab (Remicade)
- Pharmacology
- This agent is part of a class of drugs called “biologics,” so named because they are manufactured antibodies or receptors targeting and/or mimicking a variety of immune-signaling molecules such as cytokines and cytokine receptors. A number of such agents have been developed to treat immune-mediated diseases. Infliximab is a mouse-human chimeral IgG antibody against TNF-α.
- Ophthalmic uses
- Recalcitrant noninfectious uveitis of almost any form, usually after at least methotrexate not been effective and other options are undesirable.
- This agent is part of a class of drugs called “biologics,” so named because they are manufactured antibodies or receptors targeting and/or mimicking a variety of immune-signaling molecules such as cytokines and cytokine receptors. A number of such agents have been developed to treat immune-mediated diseases. Infliximab is a mouse-human chimeral IgG antibody against TNF-α.
- Administration
- The drug is given intravenously, and so one needs a relationship with an infusion center for this.
- A typical starting dose for eye disease is 5 mg per kg, repeated after 2 weeks.
- If this introductory regimen was at least partly effective, we repeat the infusion every 4 weeks thereafter, titrating the dose to 8 or even 10 mg per kg as needed.
- Initially, we examine patients right before their monthly infusions, and increase the dose if the inflammation has recurred at that point.
- Infliximab is expensive (more than 200× the cost of methotrexate). Third party payors have variable policies regarding its use.
- The drug is given intravenously, and so one needs a relationship with an infusion center for this.
- Ancillary testing
- Before starting, check purified protein derivative (PPD) for latent tuberculosis.
- Side effects
- Secondary infections. The drug can enable the reactivation of latent tuberculosis, and this must be ruled out before starting the drug.
- Activation of multiple sclerosis, lupus-like reactions, or malignancies have been reported. Any personal or family history of these is a contraindication to using infliximab.
- Secondary infections. The drug can enable the reactivation of latent tuberculosis, and this must be ruled out before starting the drug.
Adalimumab (Humira)
- Pharmacology
- This antibody is a humanized version of infliximab (which is part mouse).
- Ophthalmic uses
- Recalcant non-infectious uveitis. Reports of its use in uveitis are rare, but encouraging. It is used in the same setting as infliximab, but has the advantage being given subcutaneously, so patients can take it at home, 40 mg every 2 weeks or even every week if necessary. We would consider it in patients unable to take infliximab due to infusion reactions or anti-infliximab antibodies. There has not been a study comparing the efficacy and adverse events of the two therapies, although we believe adalimumab to be somewhat less reliably effective for uveitis.
Daclizumab (Zenapax)
- Pharmacology
- This biologic agent is a humanized antibody (being “humanized” makes it less likely to induce infusion reactions) to the interleukin 2 (IL-2) receptor, which is present on T lymphocytes. This receptor is important in T lymphocyte activation.
- Ophthalmic uses
- Birdshot retinopathy. This drug has not been widely used, but published reports suggest that it is reasonably efficacious (58% to 80% efficacy rates) in treating birdshot retinochoroidopathy.
- Posterior uveitis. One would consider this drug in posterior segment uveitis that is refractory to more conventional immunosuppression.
- Birdshot retinopathy. This drug has not been widely used, but published reports suggest that it is reasonably efficacious (58% to 80% efficacy rates) in treating birdshot retinochoroidopathy.
- Administration
- The drug is given intravenously, 1 mg per kg every 2 weeks for 3 doses. Efficacy should be apparent by this point, and if it is, then the dosing interval can be stretched to every 3 or 4 weeks for 6 months.
Other Immunomodulatory Agents
Interferon-α, anakinra, and rituximab are biologic drugs that have been used in the occasional patient with ocular inflammatory disease, with variable amounts of success. Rituximab is probably the most promising, but none has a long track record at this point.
A handful of candidate immunosuppressive drugs are used in treating other diseases but have not been found especially useful in uveitis, so we avoid them. These include sirolimus (Rapamune), etanercept (Enbrel), and leflunomide (Arava).
Nonsteroidal Anti-inflammatory Agents
As far as we can tell, aside from the perioperative setting, topical nonsteroidal anti-inflammatorys (NSAIDs) have no role at all in the treatment of uveitis. We have yet to observe a patient in whom these drops affect the control of anything more than trivial inflammation. In rare cases, oral NSAIDs are helpful in the treatment of uveitis. We find its utility limited to the scenario in which a patient who is almost—but not quite—controlled on an anti-inflammatory regimen, and requires just a tiny extra therapeutic “push” to keep the disease at bay. In addition, NSAID are utilized to lower the dose of corticosteroids to minimize side effects such as elevated IOP, weight gain, diabetes, and hypertension.
- Pharmacology
- NSAIDs are drugs that interfere with the oxygenation of arachodonic acid by inhibiting cyclooxygenase, an enzyme that is central to the biochemical process that mediates inflammation.
- These drugs have analgesic, anti-inflammatory, and antipyretic properties that make them among the most commonly prescribed drugs worldwide.
- NSAIDs are drugs that interfere with the oxygenation of arachodonic acid by inhibiting cyclooxygenase, an enzyme that is central to the biochemical process that mediates inflammation.
- Administration
- Topical NSAIDS. These agents are generally safe for long-term use, although they may irritate the cornea and rarely cause corneal melting. They are dosed four times a day. Available formulations include the following:
- Ketorolac (Acular) 0.4% and 0.5%.
- Diclofenac (Voltaren) 0.1%.
- Bromfenac (Xibrom) 0.09%.
- Nepafenac (Nevanac) 0.1%.
- Flurbiprofen sodium (Ocufen) 0.03%
- Ketorolac (Acular) 0.4% and 0.5%.
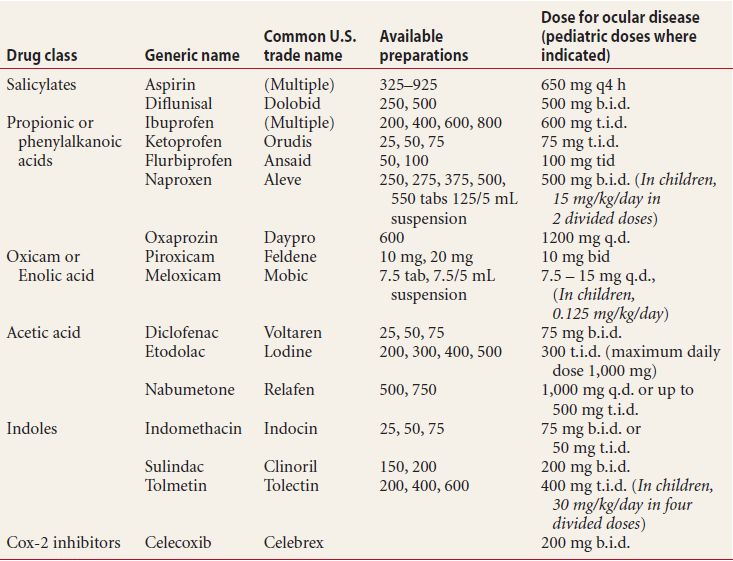
- Oral NSAIDs. A listing of available oral NSAIDs is included in Table 19.3. The dosing for oral NSAIDs is typically higher than for most other indications. Some common regimens are the following:
- Indomethacin 150 mg per day split into two or three doses.
- Diflunisal 500 mg two times per day.
- Tolmetin 1200 mg per day split into two or three doses.
- Naproxen 500 mg two times per day or
- Meloxicam (Mobic) 7.5 mg per day
- Indomethacin 150 mg per day split into two or three doses.
- Topical NSAIDS. These agents are generally safe for long-term use, although they may irritate the cornea and rarely cause corneal melting. They are dosed four times a day. Available formulations include the following:
- Indications
- Prevention of intraoperative miosis. Topical NSAIDs have long been used preoperatively for this indication in order to block the miotic effect of prostaglandins that are released during surgery. This is the only indication for which we use topical NSAIDs.
- Treatment and prevention of cystoid macular edema.
- Scleritis and episcleritis. These conditions respond to systemic NSAIDs. NSAIDs are a good choice for mild to moderate nonnecrotizing scleritis before steroids or immunosuppressants are tried.
- Uveitis. Adding oral NSAIDs can occasionally allow one to avoid changing to a more intensive form of therapy. Some practitioners advocate oral NSAIDs as a means of reducing the amount of corticosteroids needed for the long-term control of uveitis, and in the right circumstances, we find them useful for this purpose.
- Prevention of intraoperative miosis. Topical NSAIDs have long been used preoperatively for this indication in order to block the miotic effect of prostaglandins that are released during surgery. This is the only indication for which we use topical NSAIDs.
- Side effects
- Gastritis. We have patients take NSAIDs with their largest meal of the day.
- Peptic ulcers.
- Prolonged bleeding time due to decrease in platelet production.
- Renal insufficiency. These drugs are not very suitable for long-term use.
- Gastritis. We have patients take NSAIDs with their largest meal of the day.
Table 19.3 NSAID drugs commonly used to treat ocular inflammation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


