Experience with the IVI Medennium Phakic Intraocular Lens
CHAPTER CONTENTS
The Posterior Chamber Phakic Lens
THE POSTERIOR CHAMBER PHAKIC LENS
The concept of a purely posterior chamber (PC) phakic refractive lens (PRL) originated in the former Soviet Union. The first PRL consisted of a completely new nontoxic silicone material that had a higher refractive index than the previous Mushroom model (named after its mushroom shape visible on cross section) and was completely different in its configuration, parameters, and mechanism of fixation (the Mushroom model was pupil fixated; Fig. 17-1). This lens was the prototype of all other PC PRLs that are available today (Fig. 17-2).
Specifications
- intended for implantation in the PC laying on the zonular fibers
- optical zone (OZ) diameter = 5.0 mm
- total length = 11.3 mm
Advantages
- safety
- predictable results
- reversibility of procedure
- not expensive for the doctor or patient
- helps to achieve immediate and stable refractive effect
- helps to increase uncorrected visual acuity (UCVA) and best corrected visual acuity (BCVA)
- reversibility of procedure
Figure 17-1 An example of the Mushroom model.
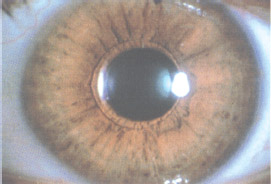
Figure 17-2 First model PRL with pupillary capture.
Indications
- high myopia (≥ −10.0 D)
The IVI MEDENNIUM Phakic Refractive Lens
IVI Medennium, Inc. (originally in Cincinnati, OH, but now in Irvine, CA), produces the PC PRL that we have been using for the past 6 years. A U.S. Federal Drug Administration study application is now in progress. We have implanted 483 Medennium lenses (three generations) since 1987 (Table 17-1).
| Generation | No. of Implants | Years of Use |
|---|---|---|
| I | 97 | 1987-1990 |
| II | 224 | Since 1990 |
| III | 162 | Since 1996 |
Specifications
- made of silicone
- refractive index = 1.46
- OZ diameter = 4.5 to 5.5 mm (depends on the optic power of the lens)
- soft, elastic, and hydrophobic
Advantanges
- implantation easy through a 3.0- to 3.5-mm clear corneal incision
- no contact between lens and anterior capsule of the crystalline lens
- easy removal if necessary
Indications
- hyperopia (+3.0 to +15.0 D but correction possible for ≤ +23.0 D)
- myopia (−3.0 to −24.0 D)
Complications
- no synechiae at long-term follow-up
- decentration in the earlier, smaller models (most common complication but not observed after changing the size parameters of the PRL in successive generations)
- cataract formation
- pigmentary glaucoma (potential, not seen)
ANALYSIS OF CLINICAL DATA
The remainder of this chapter discusses our experience with second- and third-generation IVI Medennium PRLs (Fig. 17-3). Here we analyze clinical data for 122 implants in 72 patients (aged 9-53 years), which were collected in our day-hospitals in Milano and Bari, Italy, since 1994.
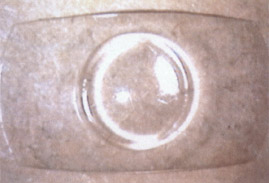
Figure 17-3 Overall design of the latest model of the silicone Russian PRL.
Preoperative Considerations
Inclusion Criteria
- myopia (110 cases; Table 17-2)
- −6.00 to −23.00 D (present treatable errors)
- −4.00 to −25.00 D (future treatable errors)
- −6.00 to −23.00 D (present treatable errors)
- hyperopia (12 cases; see Table 17-2)
- +3.00 to +16.00 D (+16.00 D maximum)
- safer to limit to +11.00 D [unless there is a deep anterior chamber (AC) because the AC of hyperopic patients is usually shallow]
- +3.00 to +16.00 D (+16.00 D maximum)
- unilateral high myopia with amblyopia in children (7 cases; see Pediatric Usage)
- patient age 11 to 14 years
- scleral reinforcement surgery recommended for progressive myopia
- patient age 11 to 14 years
- combined astigmatism (13 cases)
- more than 3.75 D [if > 1.00 D, PRL implantation followed by additional astigmatic keratectomy (AK) no sooner than 1 month later]
- keratoconus with a high myopic component (1 case)
- refractive errors (2 cases) from radial keratectomy (RK), photorefractive keratotomy (PRK), and laser in situ keratomileusis (LASIK)
- replacement of earlier model of the PRL (2 cases of dislocation)
| Preoperative Refraction | Percent of Total Study Population |
|---|---|
| Myopic patients (110 cases) | |
| −5.0 to −7.0 D | 16 |
| −7.0 D to −10.0 D | 37 |
| >−10.D | 47 |
| Hyperopic patients (12 cases) | |
| +3.5 to +5.0 D | 67 |
| +5.0 to + 8.0 | 22 |
| > +8.0 D | 11 |
Exclusion Criteria
- a clouded or nontransparent cornea
- cataracts
- lens subluxation
- glaucoma or ocular hypertension
- a shallow AC (<2.7 mm)
- vitreo/retinal problems that preclude good vision or require posterior segment intervention
- previous ocular surgery (e.g., vitreo/retinal surgery or glaucoma filtration)
- patient age more than 60 years
- diabetic retinopathy
POWER CALCULATION Accurate measurement of the precise refraction of the eye, axial length, and corneal power are imperative for proper use of the various methods of calculation.
The Russian Method: Vertex Chart
- Use the spherical equivalent of the most accurate refraction of the eye to interpolate the power of the IVI Medennium PC PRL.
- These powers are based on a simple vertex correction from 12 mm to the corneal plane.
- Although this method does not make intuitive sense optically, our experience to date shows it to be remarkably accurate.
The Holladay Refraction Formula
- Jack Holladay published a formula in the American Journal of Ophthalmology in 1993 for calculating the power of an intraocular lens (IOL) for an aphakic eye, ametropic pseudophakic eye (piggyback IOL), or PRL for a phakic eye.
- This method does not require measurement of the axial length but does need the corneal power, preoperative refractive error, desired postoperative refractive error, and the vertex distance of both.
- To obtain emmetropia, the formula is:
PRL =
1336/[(1336/{103/[(103/RPRE) – V]} + K)] – ELP – 1336/[(1336/K)- ELP ]
where RPRE = preoperative prescription; V = vertex of RPRE; K = average K; and ELP = estimated AC depth of PRL.
- To obtain ametropia, the formula is more complex:
PRL =
1336/[(1336/{103/[(103/RPRE) – V]} + K)] – ELP – 1336/[(1336/{103/ [(103/RPO) – V]}+K)] – ELP
where RPO = desired postoperative prescription; V = vertex of RPO.
Medications
- Begin instillation of antibiotics drop [Tobradex (Alcon, Fort Worth, TX)] after removing contact lenses 36 to 24 hr before surgery.
Surgical Considerations
Iridectomy
- Perform a surgical or YAG iridectomy.
- surgical iridectomy at the same time as PRL implantation
- Perform the basal iridectomy at the 12:00 position on the eye.
- Perform the procedure after inserting the PRL.
- You must perform a complete iridectomy. (Carefully check that the pigment layer has been cut through, ensuring that the crystalline lens has not been damaged.)
- Perform the basal iridectomy at the 12:00 position on the eye.
- laser iridectomy prior to PRL implantation
- Perform two iridectomies with an yttrium-aluminum-garnet (YAG) laser about 2 weeks before PRL implantation at 11:00 and 1:00 on the eye.
- Avoid making the iridectomies too large.
- Make the iridectomies as peripheral as possible because light and additional images pass through them.
- One of our patients complained about night glare. (The iridectomy was large and located near the pupil edge; we sutured it and patient complaints decreased.)
- Avoid making the iridectomies too large.
- Perform two iridectomies with an yttrium-aluminum-garnet (YAG) laser about 2 weeks before PRL implantation at 11:00 and 1:00 on the eye.
Medications
- We recommend balanced saline solution (BSS) for irrigation.
- Use low-density viscoelastic.
- Administer 25 mg of oral acetazolamide 30 min before surgery.
- Mydriatics facilitate maximum pupil dilatation during surgery.
- We never use atropine because the pupil needs to constrict rapidly immediately after surgery.
- We use phenylephrine and cyclopentolate.
- We never use atropine because the pupil needs to constrict rapidly immediately after surgery.
- The miotic acetylcholine in the AC aids pupil constriction after insertion.
- Inject corticosteroid subconjunctivally and 4.0 mg of cortisone intramuscularly at the end of the procedure (optional).
- Instill topical pilocarpine (at the end of surgery).
- Instill antibiotic drops (at the end of surgery).
Anesthesia
- Retrobulbar or peribulbar anesthesia was used exclusively and is now especially recommended.
- Topical anesthesia is not recommended.
- It is very important that the eye not move at all during the sensitive period of haptic placement behind the iris using the spatula.
- Sudden unexpected movement of the eye may result in damage to the crystalline lens and cause a cataract.
- It is very important that the eye not move at all during the sensitive period of haptic placement behind the iris using the spatula.
Instrumentation
- a clear cornea incision blade (diamond or stainless steel; 3.0-3.2 mm)
- wide Dementiev forceps (for PRL implantation; Janach Co., Italy)
- Dementiev PRO spatula-manipulator (Janach Co.)
- standard set of iris scissors and iris forceps (for manual iridectomy)
- standard lid speculum
- eye fixation forceps
- fine forceps
Methods
- handling the implant
- After opening the sterile plastic container that holds the PRL, pick up the PRL using the special forceps.
- Ensure that the lens does not touch the skin, conjunctiva, lids, lashes, or epithelium of the cornea because certain microelements are attracted to and become deposited on the lens surface.
- Grasp the implant with the forceps in the correct position (longitudinal).
- Verify positioning by ensuring that the anterior surface of the lens is up and the posterior surface is down.
- The PRL has a similar convexity (curvature) that parallels that of a natural lens.
- Do not squeeze the PRL too hard because it is easily damaged.
- Do not fold the lens because it folds itself during insertion.
- After confirmation of correct grasping and orientation of the PRL in the forceps, irrigate profusely with BSS in a syringe.
- Inspect the PRL carefully.
- Remove any foreign particulate matter or fibers that may have become attached to its surface with fine forceps.
- The PRL is now ready for insertion.
- After opening the sterile plastic container that holds the PRL, pick up the PRL using the special forceps.
- making the incision
- Do not begin surgery if the diameter of the pupil is less than 5.0 mm.
- Usually place the incision at the temporal cornea.
- Our experience recommends performing a clear corneal, self-sealing incision 3.0 to 3.2 mm wide.
- Use a type of incision for self-sealing cataract surgery that allows nonsutured closure of the wound.
- Use a diamond or stainless-steel blade to make the incision.
- Use any method of fixation to ensure that the blade does not contact the anterior lens capsule (pupil is widely dilated).
- Do not begin surgery if the diameter of the pupil is less than 5.0 mm.
- viscoelastic insertion
- Immediately fill the AC with viscoelastic substance to achieve a chamber at least 3.0 mm deep.
- Also place some viscoelastic under the iris to make more room for lens insertion in the PC.
- Immediately fill the AC with viscoelastic substance to achieve a chamber at least 3.0 mm deep.
- paracentesis
- Create an additional entry point for the lens manipulator that facilitates positioning of the PRL in the PC.
- Make this incision with a stainless-steel or diamond knife.
- We create an incision no larger than 1.0 to 1.5 mm and place it at the 12:00 position.
- Hold the knife perpendicular to the corneal surface.
- Make the cut at the limbus, so that the iridectomy is more basal so light does not pass through the iridectomy, the upper lid covers the iridectomy (fewer halos), and the iridectomy does not become blocked by the edge of the PRL (pupillary block).
- Create an additional entry point for the lens manipulator that facilitates positioning of the PRL in the PC.
- lens insertion
- This is the most important and delicate step of the procedure.
- Do not (1) damage the implant because it is very soft, thin, and rather expensive (Fig. 17-4), (2) damage the anterior capsule with the forceps, or (3) touch the endothelium with the implant or forceps.
- Grasp the implant with the special forceps that are designed to protect the OZ of the PRL (only the haptic area of the implant touches the forceps).
- Insert the PRL through a 3.0- to 3.2-mm incision without any additional folding.
- After inserting the implant into the AC, gently open the forceps to release the lens.
- The eye must make no unexpected sudden movements during this crucial maneuver.
- If the PRL is upside down, it is necessary to remove it.
- This is the most important and delicate step of the procedure.
- retro-iris placement and centration
- Manipulate the peripheral edges of the PRL under the iris.
- Using the spatula-PRL manipulator (entered from the paracentesis at 12:00), move the two lateral edges of the lens under the pupil margin and under the iris.
- Pay maximum attention to the amount of pressure that you exert on the crystalline lens capsule (too much pressure will damage the anterior capsule and cortex).
- Try to fold the PRL with the spatula and then release it under the iris to avoid damage to the zonular fibers.
- When all four “feet” are satisfactorily under the iris, gently center the PRL OZ using the spatula-PRL manipulator (Fig. 17-5).
- Manipulate the peripheral edges of the PRL under the iris.
- iridectomy
- We recommend injecting acetylcholine solution into the AC to constrict the pupil as much as possible before performing the iridectomy.
- We prefer to perform the iridectomy at 12:00 through the paracentesis site.
- Make the iridectomy as peripheral as possible to decrease the risk of blockage by the PRL.
- If bleeding occurs during this step, we prefer to reinject viscoelastic as a tamponade in the area of bleeding.
- After an appropriate waiting period (and clotting has occurred), remove the viscoelastic.
- Make the iridectomy as peripheral as possible to decrease the risk of blockage by the PRL.
- We recommend injecting acetylcholine solution into the AC to constrict the pupil as much as possible before performing the iridectomy.
- viscoelastic removal
- Try to remove all the viscoelastic by irrigation with BSS.
- If you are unable to remove all the viscoelastic, remove as much as possible and do not leave any in the AC or PC.
- Viscoelastic in the AC or PC may lead to (1) a postoperative increase in IOP or (2) viscoelastic crystallization between the anterior capsule and the posterior surface of the implant.
- You may use irrigation/aspiration if irrigation alone does not remove enough of the viscoelastic, but do not damage the endothelial cells.
- Try to remove all the viscoelastic by irrigation with BSS.
- Suturing the incision is unnecessary.
- At the conclusion of the procedure, we prefer to inject cortisone solution subconjunctivally at 12:00 and feel it helps to close the paracentesis by the conjunctiva.
- Placing a patch on the eye is not obligatory.
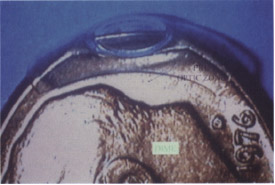
Figure 17-4 Example of the size and thickness of the silicone PRL compared with a dime.

Figure 17-5 IVI-Medennium PRL well-centered in the PC with 20/20 UCVA.
Operative Complications
- damage to the PRL
- may occur during insertion into the AC if you do not use special forceps
- may also happen during release and manipulation of the PRL under the iris
- may occur during insertion into the AC if you do not use special forceps
- bleeding
- uncommon
- may occur during the manual surgical iridectomy
- uncommon
- iris damage
- lens damage
- the worst complication possible during the actual procedure
- possible at many points in surgery: (1) during corneal incisions because of sudden knife insertion or eyeball movement; (2) during paracentesis because of insufficient viscoelastic in the AC, too quick blade movement, or eyeball movement; (3) during implant insertion because of contact between the forceps and the anterior capsule of the lens; (4) during implant manipulation because of pushing the implant on the lens; and (5) during viscoelastic removal because of inadvertent movement of irrigation or aspiration needle or excessively forceful BSS irrigation
- remedy with phacoemulsification with IOL implantation
- the worst complication possible during the actual procedure
- endothelial cell damage
- from inadequate viscoelastic protection
- from silicone in the PRL (no published data)
- endothelium damage not noticed even when edge of PRL touches the endothelium (personal experience) perhaps because of the high endothelial cell density in younger patients
- from inadequate viscoelastic protection
- zonular fiber damage
- necessary to remember that a large number of zonular fibers stretch across the anterior periphery of the lens capsule
- may result from pushing the implant too strenuously under the iris
- may lead to implant dislocation and OZ decentration
- necessary to remember that a large number of zonular fibers stretch across the anterior periphery of the lens capsule
Postoperative Considerations
Medications
- cortisone and antibiotic drops (Tobradex) 5 to 6 times a day for 7 to 10 days
- mydriatic drops 3 to 4 times a day for 3 days (do not use atropine) with 3 to 4 hr action (not complete pupil dilation)
- Diamox tablets (250 mg) twice a day on the first postoperative day and then 125 mg twice a day for 2 to 3 days
- You may notice a transitory increase in IOP the first postoperative day, which means that viscoelastic was not completely removed from the AC or PC.
- If the IOP is more then 20 mmHg, increase the dosage of Diamox to 250 mg, 3 to 4 times a day until the IOP is normalized.
- You may notice a transitory increase in IOP the first postoperative day, which means that viscoelastic was not completely removed from the AC or PC.
- nonsteroid drops [10-12 days after finishing Tobradex; we use Voltaren (CIBA Vision, Atlanta, GA) for 7 days]
Complications (Table 17-3)
- increase in IOP (> 30 mmHg) on first or second day postoperatively
- The patient feels pain in the eye and complains of vision loss or headache in the temple.
- On slit-lamp examination the chamber may be shallow, the pupil doesn’t react to light or is sluggish, residual viscoelastic is in the AC or PC, and the gap between the PRL and anterior capsule is larger than normal.
- Check the patency of the iridectomy by testing the visual and red reflex.
- Make the iridectomy bigger or create an additional one (perhaps with a YAG laser) if it is small or closed.
- Reabsorb the residual viscoelastic in the chamber by administering Diamox (≤ 1.0 g/day) and keeping the pupil dilated.
- Administer beta-blocker drops until the IOP is normalized.
- We have witnessed four cases of increased IOP (21-27 mmHg) at the 1- week postoperative visit.
- All four cases were treated topically with timolol maleate 0.5% ophthalmic drops and Diamox.
- Two weeks postoperatively, the IOP was within normal limits (≤ 17 mmHg) for all four cases.
- Pupillary block was observed in one eye 3 weeks after insertion of a second generation lens.
- We surgically enlarged the iridectomy, which relieved the pupillary block.
- We observed no recurrence of pupillary block.
- Be ready to convert the procedure to phacoemulsification for crystalline lens extraction with IOL implantation.
- Keep an IOL ready in the OR with all IOL power calculations done in advance.
- Reabsorb the residual viscoelastic in the chamber by administering Diamox (≤ 1.0 g/day) and keeping the pupil dilated.
- The patient feels pain in the eye and complains of vision loss or headache in the temple.
- subcapsular opacity
- To date, we have seen only one case of subcapsular opacity 13 months after surgery.
- The patient lost one line of BCVA and has poor contrast sensitivity.
- To date, we have seen only one case of subcapsular opacity 13 months after surgery.
- iridocyclitis (in the near postoperative period)
- The etiology of this complication remains unknown, but all cases occurred in hyperopic eyes with lenses produced outside the United States approximately 1 to 2 months after surgery.
- A nonsmooth surface may have irritated the posterior surface of the iris and started the mechanism of sterile inflammation.
- This rare complication is more common in hyperopic eyes (3 cases).
- Patient complains that vision is deteriorating but there is no pain.
- On slit-lamp examination, you will notice flare and cells in the AC, some synechiae between the PRL and the pupil, and a pupil that is small and difficult to dilate.
- Combination therapy is needed: steroids, atropine, adrenaline subconjunctival injection, systemic steroids, and maximum mydriasis.
- We have had three cases of iridocyclitis, two of which occurred in the same patient who had both eyes implanted.
- Using the combination therapy noted above, we achieved a normal result within 2 to 3 days.
- We consider this type of reaction to be sterile iridocyclitis with low pigment dispersion.
- We did not exchange implants in these three cases.
- No further reactions or cataracts have formed to date.
- This rare complication is more common in hyperopic eyes (3 cases).
- The etiology of this complication remains unknown, but all cases occurred in hyperopic eyes with lenses produced outside the United States approximately 1 to 2 months after surgery.
| Adverse Event | No. of Occurrences | % Incidence {n/N; N = 122) | Implant Generation |
|---|---|---|---|
| Corneal edema | 0 | 0.00 | |
| after 1 month | |||
| Hyphema | 0 | 0.00 | |
| Macular edema | 0 | 0.00 | |
| Raised IOP requiring | 4 | 3.28 | II and III |
| treatment ≤ 1 month | |||
| postoperatively | |||
| Persistent raised IOP | 0 | 0.00 | |
| Pupillary block | 1 | 0.82 | II |
| Retinal detachment | 0 | 0.00 | |
| Cataract | 1 | 0.82 | |
| Nonspecific | 3 | 2.45 | II |
| inflammatory reaction | |||
| Implant decentration1 | 4 | 3.27 | II |
| Endophthalmitis | 0 | 0.00 | |
| Iridocyclitis | 3 | 2.45 |
1 Implant decentration occurred in four eyes of three patients who underwent implantation with negative-power generation II lenses; one patient had implant decentration of both operated eyes. All four decentered lenses were exchanged for the generation III implant, which was designed to improve centration and avoid decentration of its OZ.
Results
- Postoperative refractive results have not changed substantially since the earliest days after surgery (Table 17-4).
- For patients with preoperative astigmatism, we performed AK at least 1 month after PRL insertion.
- In 66.1% of cases, we obtained emmetropia.
- In 26.8% we saw a residual undercorrection (myopia) no greater than –1.00 D.
- 7.1% needed additional spectacle correction (> –1.0 but <–2.5 D; in all 6 cases the goal was to leave some residual myopia because all were presbyopic patients).
- In 46.6% of the eyes we achieved no loss of any lines of BCVA.
- In 54% we noted an increase in lines of BCVA.
- In 3.3% one line of BCVA was lost.
- Postoperative UCVA was better than preoperative BCVA in 55.1% (66/122) of the cases.
- No eyes had UCVA .worse than 20/200 at the last postoperative visit.
- In eyes that required PRL exchange because of dislocation [2 of the 26 exchanges performed to date are included in this study], we achieved the same BCVA as before the first PRL insertion (Fig. 17-6).
- Average endothelial cell loss (including patients who underwent two PRL procedures) was 5%, which does not differ from that reported with cataract surgery.
- In 54% we noted an increase in lines of BCVA.
| n/N (N = 122) | % of Population | |
|---|---|---|
| UCVA | ||
| 20/40 or better | 112 | 91.8 |
| 20/50 to 20/80 | 7 | 5.75 |
| 20/100 to 20/150 | 2 | 1.6 |
| 20/200 | 1 | 0.8 |
| Lines of BCVA gained or lost | ||
| Gained 5-7 lines | 6 | 4.9 |
| Gained 3-4 lines | 11 | 9.0 |
| Gained 2 lines | 12 | 9.8 |
| Gained 1 line | 37 | 30.3 |
| No change | 52 | 42.6 |
| Lost 1 line | 4 | 3.3 |
| Manifest sphere (compared with emmetropia) | ||
| Within 0.0 D | 39 | 66.1 |
| Within ±0.5 D | 8 | 13.6 |
| Within ±1.0 D | 6 | 10.2 |
| Within ±2.0 D | 4 | 6.8 |
| >2.0D | 2 | 3.4 |
Pediatric Usage
MYOPIA PRL insertion is an alternative to amblyopia treatment with aniseikonic spectacles or forced use of contact lenses. Without treatment, these eyes are destined for lifetime strabismus with deep amblyopia.
Indications
- high unilateral myopia (The youngest patient in whom we have implanted a myopic PRL was 7 years old with –14.00 D and amblyopia of 20/100 BCVA).
Advantages
- correction of myopia
- treatment of amblyopia
- prevention of strabismus
- exchangability of PRL if the refractive error changes when the child grows to adulthood
- ability to repeat the implantation if necessary
Patient Preparation
- We prefer and recommend performing scleral reinforcing surgery 1 to 2 months before implantation to slow growth of the eyeball.
Results
- 20/40 UCVA at 20 months postoperatively from 20/100 preoperatively
- all had improved BCVA 6 months postoperatively after occlusion therapy
HYPEROPIA We plan to start correcting hyperopia in the near future but currently do not have any clinical experience correcting hyperopia with PRL implantation in children.
Methods
- The surgical technique is the same as that for our adult patients except for the following.
- We recommend general anesthesia.
- We also prefer manual iridectomy instead of laser iridectomy at the time of surgery.
- We recommend general anesthesia.
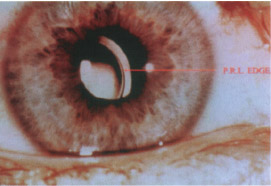
Figure 17-6 Temporal dislocation of a PC silicone PRL.
CONCLUSION
The goal of any refractive procedure is emmetropia, and the predictability of PRL implantation provides promise for achieving it. The refractive effect may be compared with contact lenses. Reversibility is PRL implantation’s most attractive feature because few refractive procedures currently may be reversed. Any skilled cataract surgeon is able to perform PRL insertion safely and easily. The complications that we have seen are not serious and were easily treated. Two main problems and complications that we need to investigate in longer follow-up are subcapsular opacities (so far we have seen only one) and pigment dispersion, which may cause glaucoma. Our study shows no pigment dispersion in negative power silicon PRLs but some slow dispersion in positive power PRLs. The ultrasound biomicroscope study showed us that the implant does not touch the anterior capsule, but we need to know more about the touching of the capsule and iris.
FUTURE APPLICATIONS
Piggyback over Intraocular Lenses
When two IOLs are necessary, it is certainly conceivable that the second lens could be a PC PRL easily inserted in the capsular bag or the ciliary sulcus. In special eyes that require piggyback lenses, the calculations of IOL power are often not as accurate and it may be necessary to exchange the more anterior lens. A PRL is much easier to remove and replace than an IOL (Fig. 17-7).
Pseudophakic Ametropia Correction
Every patient who is unhappy with the refractive results of cataract or IOL surgery could be offered a rather simple procedure of PC PRL implantation over the IOL. This application would open a whole new market for the anterior segment surgeon and replace the dangers inherent in removing and replacing a well-placed IOL in the capsular bag. Patients would more likely obtain a desirable refractive result.
Patients who wish to try monovision could have the nondominant eye implanted with an additional plus power PRL over the emmetropic IOL. If monovision was intolerable, the PRL could be easily and atraumatically slipped out.
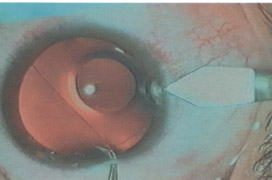
Figure 17-7 The beginning of surgery to exchange the PRL of Figure 17-6 with one that has a larger sulcus-to-sulcus diameter.
Multifocal Correction
Patients could have an emmetropic IOL implanted with a multifocal PRL placed on top of it during cataract removal. After sufficient time has passed and the patient has become accustomed to it, the patient could decide to keep the PRL or have it easily slipped out.
Patients could have a multifocal PRL placed on top of an IOL to try it out. Again, if they didn’t like it, it is easily removed. Perhaps any over- or under-correction in the original IOL could also be taken into account when calculating the PRL distance power.
Suggested Readings
Asseto V, Benedetti S, Pesando P. Collamer intraocular contact lens to correct high myopia. J Cataract Refract Surg. 1996;22:551-556.
Baikoff G. Anterior chamber phakic IOLs. AAO Annual Meeting: 1998; New Orleans.
Baikoff G, Joly P. Comparison of minus power anterior chamber intraocular lenses and myopic epikeratoplasty in phakic eyes. Refract Corneal Surg. 1990;6:252-260.
Baikoff G, Arne JL, Bokobza Y, et al. Angle fixated anterior chamber lens for myopia of –7.0 to –19.0 diopters. J Cataract Refract Surg. 1998;14:282-293.
Chatterjee A, Shah S. Predictability of spherical PRK based on initial refraction. J Refract Surg. 1998;14(suppl).
Fechner PU. Intraocular lenses for the correction of myopia in phakic eyes: short term success and long term caution. Refract Corneal Surg. 1990;6:242-244.
Gelender H. Corneal endothelial cell loss, cystoid macular edema, and iris-supported intraocular lenses. Ophthalmology. 1984;91: 841-846.
Hodkin M, Lemos MM, McDonald MB, HolladayJT, Shhidi SH. Near vision sensitivity after photorefractive keratectomy. J Cataract Refract Surg 1997;23:2.
Holladay JT. Refractive power calculation for intraocular lenses in the phakic eye. Am J Ophthalmol. 1993;116:63-66.
Marinho A, Neves MC, Pinto MC, Vaz F. Posterior chamber silicone phakic intraocular lens. J Refract Surg. 1997;13:219-222.
< div class='tao-gold-member'>



