The Posterior-Chamber Implantable Contact Lens
CHAPTER CONTENTS
The STAAR Implantable Contact Lens
Intraocular Lens Insertion and Laser In Situ Keratomileusis (Bioptics)
Refractive surgery for extreme ametropias (myopia > –12.00 D and hyperopia > +4.00 D) has progressed tremendously since around 1990, but not without drawbacks and controversy. Radial keratotomy (RK), photokeratectomy (PRK), laser in situ keratomileusis (LASIK), and phakic intraocular lens (IOL) insertion all involve certain risks that may not balance their advantages (Table 16-1). For example, anterior chamber (AC) IOLs are relatively easy to insert and produce excellent predictable refractive results, but they may put the integrity of the corneal endothelium and AC angle at risk for complications that may occur more than 40 years in the future. Table 16-2 compares IOL implantation and cataract surgery.
Advantages
- irrelevance of corneal thickness
- ability to correct a wide range of refractive errors
- better optics from refractive correction close to the nodal point of the eye
- less optical degradation
- no regression
- excellent predictability of results
- preservation of accommodation
- small astigmatically neutral incision with the foldable IOL
THE STAAR IMPLANTABLE CONTACT LENS
In 1986, Svyatoslov Fyodorov introduced a one-piece silicone IOL for use in phakic patients. Cataract formation and uveitis were early concerns, and cataract formation from his early “top hat” design was reported as late as 1993. STAAR Surgical Co. refined Fyodorov’s IOL design by incorporating collagen into the IOL material, which has improved the biocompatability and results obtained with today’s STAAR implantable contact lens (ICL) (STAAR model MIS-PF or MSI-TF injector and STAAR model FTP foam-tipped plunger with STAAR model SFC-45 cartridge).
Specifications
- porcine collagen/hydroxyethylmethylacrylate copolymer
- refractive index of 1.45 at 35°C
- plate haptic design
- foldable
- implantable through a 3.0-mm corneal incision
- central concave/convex optic sizes [4.5-5.5 mm in diameter; a 4.8-mm optic on a posterior-chamber (PC) phakic lens is the equivalent of a 6.05-mm optical refractive zone on the cornea; e.g., for the 5.5-mm lens, its equivalent corneal optical zone is 6.9 mm]
- myopic IOLs available (−3.0 to −20.0 D)
- hyperopic IOLs available (+3.0 to +17.0 D)
- five ICL lengths are manufactured (11.0 mm, 11.5 mm, 12.0 mm, 12.5 mm, and 13.0 mm)
- rests in front of, but not on, the anterior capsule
- central concave/convex optic sizes [4.5-5.5 mm in diameter; a 4.8-mm optic on a posterior-chamber (PC) phakic lens is the equivalent of a 6.05-mm optical refractive zone on the cornea; e.g., for the 5.5-mm lens, its equivalent corneal optical zone is 6.9 mm]
PREOPERATIVE CONSIDERATIONS
Indications
- refractive error (extreme errors uncorrectable by LASIK because of poor predictability or inability to maintain adequate corneal thickness)
- corneal thickness insufficient for LASIK
- overcorrection from previous refractive surgeries
- keratoconus (possible correction)
- amblyopia (possible correction)
Inclusion Criteria
- stable refraction for the last 12 months
- AC depth of at least 2.8 mm
- good general health
- good ocular health
- preoperative consent with explanation of alternatives
Patient Preparation and Evaluation
- discontinuation of contact lens wear (> 2 weeks for soft contact lenses and > 4 weeks for rigid gas-permeable lenses)
- measurement of refractive stability (must have been stable for more than 1 year) and refractive parameters
- dilated ocular examination
- manifest and cycloplegic refraction (myopic patients usually prescribed an ICL power approximately 3.0-5.0 D above the spherical portion of manifest refraction; for hyperopes, the difference is ∼5.0-7.0 D)
- keratometry (preferably by corneal topography)
- measurement of AC depth (from corneal endothelium to anterior capsule)
- central pachymetry
- axial length by A-scan ultrasonography
- calculation of the appropriate ICL model and diopter based solely on biometric and refractive data
- currently handled by STAAR Surgical Co.
- performed with formulas developed by Feingold and Olsen
- currently handled by STAAR Surgical Co.
- estimation of the diameter of the ciliary sulcus (i.e., white-to-white limbal measurement) to determine the degree to which the ICL vaults in front of the crystalline lens
- Measure the distance with calipers at least three times to ensure accuracy.
- Perform topography using devices such as the Orbscan II (Orbteklnc, Salt Lake City, UT) or the Vista Hand-Held Corneal Topographer (EyeSys/Premier, Jacksonville, FL)].
- Measure the distance with calipers at least three times to ensure accuracy.
- choice of the proper ICL size
- Add 0.5 mm to the white-to-white measurement for myopic lenses.
- Subtract 0.5 mm from the white-to-white measurement for hyperopic lenses.
- To ensure proper central vaulting of the myopic ICL, modulate the chosen lens size based on anterior chamber depth (ACD) (Table 16-3). (Accommodation of the crystalline lens primarily occurs by changes to its posterior plane and is therefore not affected by the ICL, which appears to differentially vault as the lens accommodates.)
- If these measurements suggest a lens size between the available ICL lengths, choose the next largest size if the eye has a large angle (>0.7 mm) or the next smaller size if the angle is small (<0.7 mm) (e.g., an eye with a white-to-white measurement of 11.25 mm, an ACD of 3.3 mm, and a large angle should get a 12.0-mm lens).
- Add 0.5 mm to the white-to-white measurement for myopic lenses.
| Cataract Surgery | ICL Surgery |
|---|---|
| IOLs are implanted into capsular bag. | ICLs are placed in front of a normal lens. |
| Protection of corneal endothelium is critical. | The anterior capsule must be protected. |
| Removal of tissue can hide surgical errors. | Tissue damage immediately obvious. |
| Some refractive errors are tolerated. | Predictability of results is essential. |
| Speed and efficiency are emphasized. | ICL placement is a delicate procedure. |
Peripheral Iridotomies
An iridotomy is a procedure that creates a small hole in the outer part of the iris to connect the PC and AC of the eye. This allows the aqueous fluid to drain easily to the AC.
Indications
- prophylactic prevention of the development of pupillary block glaucoma following ICL implantation
Equipment
- a neodymium:yttrium-aluminum-garnet laser
- an argon-krypton laser
- combination of both lasers
Methods
- Schedule 1 to 2 weeks before ICL implantation.
- Set laser power settings as low as possible (1-5 mW).
- Pretreat with an argon laser to reduce intraoperative bleeding.
- Minimize any damage to the underlying lens capsule by using the lowest power and the fewest laser pulses.
- Place the iridotomies at approximately the 10:00 and 2:00 positions on the peripheral iris and no more than 90 degrees (3 hr on a clock face) apart.
- Ensure that at least one iridotomy is patent after ICL placement.
- Make each iridotomy 0.8 to 1.0 mm in diameter.
- Verify patency before ICL surgery.
SURGICAL CONSIDERATIONS
Absolute Contraindications
- history or clinical signs of ocular disease 0 cataracts
- iritis/uveitis in either eye
- diabetic retinopathy in either eye
- glaucoma in either eye
- progressive sight-threatening disease (other than myopia)
- pigmentary dispersion syndrome
- pseudoexfoliation syndrome
- iritis/uveitis in either eye
- visually significant pre-existing lens opacities causing best corrected visual acuity (BCVA) of 20/40 or worse
Relative Contraindications
- blindness in the fellow eye (monocularity)
- unrealistic patient expectations
- irregular astigmatism
- unstable refraction
- age greater than 50 years (consider refractive lensectomy; see Chapter 13)
Equipment
- Occucoat or STAARVISC viscoelastic substance
- diamond keratome, 2.7 or 3.2 mm (model no. N03820; Diamatrix Ltd. Inc., The Woodlands, TX)
- trifacet keratome for paracentesis or any diamond blade (e.g., Diamatrix, model no. N03420)
- Lindstrom lens insertion forceps without notch (model no. SP2325; Rhein Medical Inc., Tampa, FL)
- lens tucker (model no. 6-479; Duckworth 8c Kent)
- Nugent (blunt) forceps (to open lens vial)
- manual or automated irrigation/aspiration (I/A) set-up
Medications
- drops for achieving maximal pupillary dilation
- tropicamide 1% or cyclopentolate 1% (5-10 min, 3-4 times)
- phenylephrine 2.5% (3-4 times, 5-10 min before surgery
- flurbiprofen, 0.03% (2-3 times daily for 2 days prior to surgery to reduce miosis)
- tropicamide 1% or cyclopentolate 1% (5-10 min, 3-4 times)
Anesthesia
- Use anesthesia as for cataract surgery.
- Although ICL implantation may be accomplished under topical or local anesthesia, new ICL surgeons should utilize local anesthesia (peribulbar or retrobulbar) to provide good prolonged akinesia and anesthesia.
- Once new surgeons have mastered the ICL implantation technique, they can perform it effectively under topical anesthesia in less than 15 min.
- topical anesthesia (one of the following) 0 proparacaine 0.5% (one drop, 5-10 min, 3-4 times)
- lidocaine 1%-4% (one drop, 5-10 min, 3-4 times)
- Marcaine 0.5% (one drop, 5-10 min, 3-4 times)
- lidocaine 1%-4% (one drop, 5-10 min, 3-4 times)
- peribulbar local anesthesia
- lidocaine 1% (5 cc without epinephrine)
- 5/8 inch 25-G needle
- higher potential for globe perforation in high myopes
- lidocaine 1% (5 cc without epinephrine)
- retrobulbar local anesthesia
- lidocaine 1% (5 cc without epinephrine)
- a 1.5 inch 27-G needle
- results in less chemosis than peribulbar approach
- higher potential for globe perforation in high myopes
- lidocaine 1% (5 cc without epinephrine)
Methods
- Dilate eye as indicated above.
- Confirm a minimum dilation of 8 mm before proceeding with ICL implantation.
- Less than 8 mm requires excessive distortion of the ICL to place it behind the iris and is thus too small for safety.
- If the pupil will not dilate to 8 mm, abort surgery.
- Less than 8 mm requires excessive distortion of the ICL to place it behind the iris and is thus too small for safety.
- Prepare and drape the ocular area as for cataract surgery.
- Lubricate the lens chamber, loading area, and barrel of the lens injector cartridge with several drops of balanced saline solution (BSS).
- Grasp the ICL with the lens-loading forceps.
- Verify the correct orientation with dimple on right leading haptic.
- A properly oriented lens has a dimple on the leading right-hand footplate and the trailing left-hand footplate.
- If these dimples are reversed, the lens is upside down.
- Avoid using an upside-down lens because the lens is designed to have an anterior vault to allow its central portion to clear the crystalline lens (an upside-down lens will touch the central crystalline lens).
- A properly oriented lens has a dimple on the leading right-hand footplate and the trailing left-hand footplate.
- Place the ICL into the loading barrel of the cartridge before making any incisions (so that any delays in loading do not cause delays in the middle of the surgical procedure).
- Tuck the sides of the ICL into the side-wall grooves of the cartridge.
- Lubricate with BSS.
- Place viscoelastic in front of and behind ICL to reduce bubble formation.
- Place the foam-tipped plunger in the injector pen.
- Hydrate the foam-tipped plunger with BSS.
- Retract the foam-tipped plunger into injector pen.
- Load the lens cartridge (containing the ICL) into the injector pen.
- Advance the plunger to push the ICL into view in the cartridge barrel.
- Again, verify the correct orientation of the ICL (reload if orientation is incorrect or questionable).
- Once loaded, keep the ICL and cartridge hydrated with BSS.
- Retract the plunger about 2 mm and then advance it to just behind the ICL.
- Again, check the pupil to verify that it is dilated to a minimum of 8 mm (10 mm preferred).
- If not dilated fully, abort surgery until appropriate dilation is achieved.
- Note: Intracameral lidocaine anesthesia may induce constriction of the pupil. If you use intracameral lidocaine, also use epinephrine diluted to 1:1,000 strength to maintain adequate mydriasis.
- If not dilated fully, abort surgery until appropriate dilation is achieved.
- Insert the lid speculum (never place surgical instruments near pupillary center).
- Make one or two paracentesis incisions 60 to 90 degrees away from the proposed area of the main incision.
- Make a beveled 3.2-mm clear corneal tunnel incision (corneal tunnel ideally 1.50-1.75 mm long).
- Place the viscoelastic cannula just inside the wound lip during injection (never insert the viscoelastic cannula across the pupil)
- Inject viscoelastic only until ripples or swirls form in the AC.
- Do not overinflate the AC with viscoelastic (may push the iris diaphragm down onto crystalline lens making ICL positioning difficult).
- Do not attempt to inject the viscoelastic around the zonules (may trap viscoelastic under the iris).
- Do not overinflate the AC with viscoelastic (may push the iris diaphragm down onto crystalline lens making ICL positioning difficult).
- Slowly inject the ICL (Fig. 16-1).
- Never allow the cartridge tip to come near the pupillary center.
- Inject the ICL with the cartridge only partially in the incision.
- Do not inject ICL quickly.
- Allow the leading haptic to unfold slowly after injecting 75% of the ICL.
- Gently pulsate the injection of the rest of the ICL to encourage the ICL to unfold.
- Do not rotate the ICL over the crystalline lens capsule.
- Do not push on the ICL with the I/A tip.
- Never attempt to lift the iris or “massage” the ICL to resolve iris capture.
- Never allow the cartridge tip to come near the pupillary center.
- Again, verify ICL orientation (the dimple on the right-hand leading haptic). (If the ICL is upside down, remove the ICL using the trailing footplates.)
- Place the leading footplates first under the iris.
- Lift and gently tuck the footplates and haptics under the iris.
- Constrict the pupil using acetylcholine chloride (Miochol; CIBA Vision Ophthalmics).
- Remove as much viscoelastic as possible from the AC after ICL implantation.
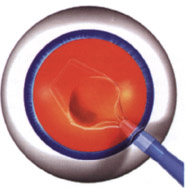
Figure 16-1 Schematic drawing depicting the insertion of the STAAR implantable contact lens (ICL).
Intraoperative Complications
- twisting or turning of the ICL during implantation
- ICL flips upside-down when injector pen removed from incision
- ICL footplate folds
- back end of ICL sticks in small incision
- a rip in the ICL haptic
POSTOPERATIVE CONSIDERATIONS
Immediate Postoperative Care
- Administer topical medications in the recovery room.
- pilocarpine 0.5 or 2% (one drop, 3 times over 10 min)
- diclofenac sodium (one drop; Voltaren, Roxane; CIBA Vision Ophthalmics)
- ofloxacin 0.3% (Ocuflox, Allergan; one drop, 4 times a day for 4 days, then 3 times a day for 4 days, then 2 times a day for 4 days, then 1 time a day for 4 days)
- prednisolone acetate 1% (Pred-Mild, Econopred, Ocu-Pred, AK-Pred, Inflamase, Pred-Forte; one drop, 4 times a day for 4 days, then 3 times a day for 4 days, then 2 times a day for 4 days, then 1 time a day for 4 days)
- pilocarpine 0.5 or 2% (one drop, 3 times over 10 min)
- Give postoperative instructions to the patient.
- Check intraocular pressure (IOP) approximately 2 to 3 hr postoperatively and treat as necessary (Table 16-4).
Follow-Up
- days 1 and 7 and months 1, 3, 6, and 12
- Measure IOP.
- Measure ICL vaulting (should be ∼25% of ICL thickness, but do not be concerned if the lens appears to be vaulted slightly >25% because it tends to “settle down” into the sulcus within a few days).
- Check uncorrected visual acuity (usually excellent immediately but may improve slightly over 2-3 weeks).
- Check corrected refraction (should be stable within 1 month).
- Evaluate the patency of the iridotomies.
- Evaluate the clarity of the crystalline lens capsule.
- Check corrected refraction (should be stable within 1 month).
- Measure IOP.
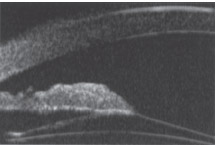
- Evaluate the position of the ICL and its interaction with structures of the anterior segment (Fig. 16-2) using ultrasound biomicroscopic imaging (essential for assessing association of findings with major complications).
- ICL-iris contact
- reduction in AC depth
- narrowing of the AC angle opening
- peripheral contact of the ICL with the crystalline lens
- ICL-iris contact
- Examine the patient as needed under a standard antibiotic/anti-inflammatory regimen [e.g., patients in a U.S. clinical study received ofloxacin and tobramycin/dexamethasone (Tobradex; Alson, Surgical Fort Worth, TX) 4 times a day for 4 days tapering off over 16 days].*
* Advise the patient that the prescription for Tobradex may not be refilled because overuse may induce secondary lens opacification (i.e., cataracts).
† These results are from Zaldivar R (1998) (Table 16.5).
| AC Depth (mm) | Amount to Add to White-to-White Measurement |
|---|---|
| <2.8 | 0; ICL implantation contraindicated |
| 2.8-3.0 | 0; white-to-white measurement ±0.5 mm as described |
| 3.1-3.5 | 0.25 mm (to maximum length of 13.0 mm) |
| >3.5 | 0.50 mm (to maximum length of 13.0 mm) |
Results†
- excellent (when the severity of the preoperative prescription is considered)
- a lower percentage of patients achieving 20/20 and 20/40 uncorrected vision than what we have come to expect for LASIK (many already had a reduced BCVA pre-operatively)
- improved BCVA of two or more lines (36% of the myopic group; offers extremely exciting opportunities for the improvement of the vision in this somewhat disabled group)
| Intraocular Pressure (mmHg) | Potential Problem | Management |
|---|---|---|
| <21 | None | Regular 24-hr follow-up |
| >21 and pupil constricted | Retained viscoelastic Blocked iridotomy | lOP-reducing agents [e.g., topical beta-blockers (Betagan, Allergan)] Topical pilocarpine Release of fluid Repeat iridotomies |
| >40 and pupil dilated | Blocked iridotomy | Release of fluid Repeat iridotomies |
| Myopia | Hyperopia | |
|---|---|---|
| Number of eyes | 124 | 24 |
| Mean refractive error (range) | −13.4 ± 2.2 D (−8.0 to −18.6 D) | +6.5 ± 2.1 D+3.8 to +10.5 D) |
| Follow-up | ≤ 36 months | 18 months |
| Efficacy 20/20 20/40 | 2% 68% | 8% 63% |
| Predictability +/−0.5 D +/−1.0 D | 44% 69% | 58% 79% |
| ≥ 2 or more lines of visual acuity, gained | 36% | 8% |
| ≥2 or more lines of visual acuity lost | 0.8% | 4% |
Source: Zaldivar R, Davidorf JM, Oscherow S. Posterior chamber phakic intraocular lens for myopia of −8 to −19 diopters. J Refract Surg. 1998;14:294-305; Davidorf JM, Zaldivar R, Oscherow S. Posterior chamber phakic interocular lens for hyperopia of +4 to +11 diopters. J Refract Surg. 1998;14:306-311.
Complications‡
- pigmentary dispersion (from ICL-iris contact)
- anterior subcapsular cataract formation (from ICL-crystalline lens contact)
- pupillary block
- IOP spikes that occur in the immediate (first 24 hr) postoperative period usually result from nonpatent iridotomies or, rarely, secondary pupillary dilation that closes off the iridotomies
- IOP spikes at 5 to 10 days postoperatively (rarely reported as a result of retained viscoelastic that causes aqueous misdirection; emphasizes need for carefully performed iridotomies as well as evacuation of viscoelastic from the eye)
- IOP spikes that occur in the immediate (first 24 hr) postoperative period usually result from nonpatent iridotomies or, rarely, secondary pupillary dilation that closes off the iridotomies
- iatrogenic cataracts
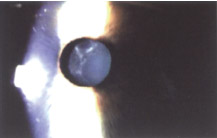
- localized “point” opacifications [caused by surgical trauma during ICL implantation (Fig. 16-3) but usually do not progress or become sight-threatening]
- central, nonlocalized, anterior subcapsular opacifications (reported in a few cases associated with no anterior vaulting above the central capsule and caused by a lens that was too small or was placed upside down in the eye, causing the lens to vault backward)
- crystalline lens opacification (estimated incidence of <1%-10%)
- late-term cataracts (reported without a direct association to surgical trauma)
- longer-term studies and follow-up required to evaluate their incidence and etiology
- localized “point” opacifications [caused by surgical trauma during ICL implantation (Fig. 16-3) but usually do not progress or become sight-threatening]
- pigmentary glaucoma
- usually results from debridement of the anterior iris surface during lens manipulation or from surgical iridotomies (not recommended)
- generally resolves within the first few weeks (indicates that it did not result from chafing of the posterior iris)
- usually results from debridement of the anterior iris surface during lens manipulation or from surgical iridotomies (not recommended)
- glare or halos (rare except for patients with physiologically large pupils)
‡ See Table 16.6 for more complications.
| Complication | Incidence |
|---|---|
| Pupillary block | 4.8% |
| ICL-related IOP spike | 1.6% |
| Steroid-induced IOP spike | 4.8% |
| Inverted IOL | 0.8% |
| IOL extraction | 4.0% |
| ICL decentration <1 mm >1 mm | 14.5% 2.4% |
| Broken IOL | 0.8% |
| Lens opacities | 2.4% |
| Retinal detachment | 0.8% |
| Other potential complications not reported | |
| ICL too small (poor vaulting) | |
| ICL too big (excessive vaulting) | |
| Pigmentary dispersion/pigmentary glaucoma | |
| Glare/halos |
Source: Zaldivar R, Davidorf JM, Oscherow S. Posterior chamber phakic intraocular lens for myopia of −8 to −19 diopters. J Refract Surg. 1998;14:294-305.
Treatment of Complications
- pupillary block from high IOP
- Treat with topical antiglaucoma medications.
- Release the aqueous fluid through the paracentesis incision.
- Constrict the pupil with pilocarpine to open the iridotomies.
- Repeat the laser iridotomies.
- Treat with topical antiglaucoma medications.
- iatrogenic cataracts
- Remove the ICL and replace it with next larger size (recommended by STAAR if the ICL is observed with
- <25% anterior central vaulting at 3 months or more postoperatively to preclude anterior capsule opacification or iris chafing).
- Remove the ICL and replace it with next larger size (recommended by STAAR if the ICL is observed with
- pigmentary glaucoma (If pigment deposits are persistent and associated with elevated IOP, consider removing the ICL.)
INTRAOCULAR LENS INSERTION AND LASER IN SITU KERATOMILEUSIS (BIOPTICS)
The ultimate goal of the refractive surgeon is the correction of any refractive error.ICLs allow surgeons to correct a wide range of spherical refractive errors, but many of these eyes also have large amounts of astigmatism. Roberto Zaldivar, MD, conceived the concept of “bioptics” to allow for full correction of virtually any refractive error.
Indications
- the correction of large refractive errors and the elimination of low to moderate levels of myopia and astigmatism (using the precision and predictability of LASIK)
Methods
- Perform the peripheral iridotomies.
- Correct the spherical component of the refractive error by implanting the ICL.
- One month later, after achieving refractive stability, correct the residual spherical and astigmatic components with LASIK (Fig. 16-4).

Figure 16-4 A schematic of the bioptics concept, which utilizes the ICL and LASIK to correct large spherical and astigmatic refractive errors.
Suggested Readings
Davidorf JM, Zaldivar R, Oscherow S. Posterior chamber phakic intraocular lens for hyperopia of +4.0 to +11 diopters. J Refract Surg. 1998;14:306-311.
Rosen E, Gore C. STAAR collamer posterior chamber phakic intraocular lens to correct myopia and hyperopia. J Cataract Refract Surg. 1998;24:596-606.
Trindade F, Pereira F. Cataract formation after posterior chamber phakic intraocular lens implantation. J Cataract Refract Surg. 1998;24: 1661-1663.
Trindade F, Pereira F, Cronemberger S. Ultrasound biomicroscopic imaging of posterior chamber phakic intraocular lens. J Refract Surg. 1998;14:497-503.
Zaldivar R, Davidorf JM, Oscherow S. Phakic intraocular lenses. In: Buratto L, Brint S, ed. LASIX. Thorofare, NJ: Slack Inc.; 1998.
Zaldivar R, Davidorf JM, Oscherow S. Posterior chamber phakic intraocular lens for myopia of –8 to –19 diopters. J Refract Surg 1998;14:294-305.
< div class='tao-gold-member'>



