The Iris-Claw Phakic Intraocular Lens
CHAPTER CONTENTS
Jan Worst originally designed the iris-claw phakic intraocular lens (IOL), and Ophtec (Boca Raton, FL) manufactures it. Many surgeons consider IOL implantation to be the safest treatment for high myopia and high hyperopia.
Specifications
- a single piece of polymethylmethacrylate
- a convex-concave optic configuration
- optic diameter: 5 or 6 mm (depending on the power of the lens that is required)
- overall diameter: 8.5 mm.
- available in 1.0-D increments (–3.0 to –23.5 D for myopia and +1 to +12 D for hyperopia)
PREOPERATIVE CONSIDERATIONS
Advantages
- lower risk for postoperative corneal ectasia, haze, and even halos compared with photorefractive keratectomy (PRK) or laser in situ keratomileusis (LASIK) (one reason for the increasing popularity of phakic IOLs)
- true reversibility of procedure
- preservation of accommodation
- better predictability of results than with PRK and LASIK for high ametropias
- higher upper limit of treatment (only −7 to −12 D for PRK), which leads to better predictability and fewer retreatments, halos, haze, and loss of BCVA
- fewer risks than with PRK or LASIK for patients with myopia higher than 10 D or hyperopia higher than 3 D (even though 60% of these patients have excellent results from the procedure)
- lower incidence of retinal detachment than with clear lensectomy, which has a non-negligible 2% risk for retinal detachment
Indications and Inclusion Criteria
- visually disabling high myopia (>− 7 D) or high hyperopia (>+3 D)
- realistic patient expectations
- patient age more than 21 years (required for refractive stability)
- endothelial cell count greater than 2000 cells/mm
- anterior chamber (AC) depth greater than 3.2 mm
- pupil size smaller than 6.5
Patient Examination
- Measure manifest and cycloplegic refraction.
- Evaluate best corrected visual acuity (BCVA) and uncorrected visual acuity (UCVA) using Snellen’s chart.
- Evaluate near visual acuity using a Jaeger chart.
- Measure pupil size in scotopic conditions.
- Perform corneal topography.
- Perform an endothelial cell count.
- Perform biometry to determine AC depth and axial length.
- Perform gonioscopy.
- Perform a slit-lamp examination of the anterior segment and fundus of the eye.
- Test patients with amblyopia or strabismus for BCVA.
- Inform these patients that the procedure will not improve BCVA.
- Exclude these patients from refractive surgery unless carefully evaluated.
- Inform these patients that the procedure will not improve BCVA.
Patient Preparation
- Perform surgery in a standard sterile cataract operating room layout.
- Instruct the patient to remove soft contact lenses at least 2 to 3 days before the preoperative examination.
- For rigid gas-permeable contact lenses, verify the stability of the eye’s topography before surgery (stability may take 4-6 weeks).
- Administer oral analgesics to the patient 15 to 30 min before surgery.
- Constrict the pupil using pilocarpine 0.2% (3 drops every 10 min).
- Administer antibiotic drops (ofloxacin 0.3%) 30 min before surgery (1 or 2 drops every 10 min).
SURGICAL CONSIDERATIONS
Absolute Contraindications
- unstable or progressive myopia or hyperopia
- glaucoma or a family history of glaucoma
- iris abnormalities
- history of uveitis
- angle closure or visible angle trauma
Relative Contraindications
- diabetic retinopathy
- autoimmune disease, Crohn’s disease, or any disease causing repeated intraocular inflammation
- amblyopia or strabismus
Methods
- Drape the patient’s head.
- Insert the speculum and isolate the eyelashes.
- Anesthetize the eye with two drops of topical tetracaine 1% (e.g., Cepacol, Viractin, or Pontocaine) or peribulbar lidocaine 2% without epinephrine (Xylocaine; Abbott Laboratories, Abbott Park, IL)
- Sterilize and prepare the eye using a swab stick with proviodine.
- Ensure that the pupil is constricted by injecting carbachol 0.01% (Carbastat) into the AC.
- Avoid using epinephrine, which dilates the pupil.
- Inject subconjunctival Xylocaine 2% in the superior, nasal, and temporal quadrants (helps to decrease patient discomfort while manipulating the iris).
- Use a 6-mm, three-step, scleral-limbal incision to minimize iris prolapse (may be a superior or temporal incision).
- If bleeding occurs, lightly cauterize the incision to avoid induced astigmatism.
- The paracentesis incisions differ from those made during standard surgery.
- Make two paracentesis incisions using a 20-gauge, 1.4-mm, V-Lance knife (one incision at the 2:00 position and one at 10:00).
- Make parallel incisions toward the 4:00 and 8:00 positions, respectively.
- Do not direct these stab incisions radially; they must point to the future enclavation site.
- End the paracentesis 1 mm superior to an hypothetical horizontal meridian bisecting the pupil (Fig. 15-1).
- Make two paracentesis incisions using a 20-gauge, 1.4-mm, V-Lance knife (one incision at the 2:00 position and one at 10:00).
- Inject a highly cohesive viscoelastic (sodium hyaluronate), such as Healon GV (Pharmacia, Peapack, NJ) through each paracentesis incision.
- Fill the AC from the periphery toward the center.
- Avoid overfilling the AC because the natural lens will bow posteriorly and the claws of the lens will bump on the inferior iris, making insertion more difficult.
- Fill the AC from the periphery toward the center.
- Apply viscoelastic on the lens.
- Insert the lens over the pupil through the incision using a lens-holding forcep with T-shaped lower jaw (Sinskey lens-holding forcep) with a 15-degree angle.
- Using an angled Sinskey or Kuglen hook, rotate the lens 90 degrees toward the horizontal meridian and desired position over the center of the pupil.
- Ensure that the lens is centered over the pupil.
- Use Miostat (Alcon, Forth Worth, TX) as needed to constrict the pupil.
- Visualize the iris spot where the claw will be entrapped.
- Insert the enclavation needle (provided by the manufacturer) for the claw that will be closest to the limbus. (Always insert the enclavation needle before the T-shaped forcep to hold the lens.)
- With the T-shaped, lower-jaw forcep, grasp the lens slighdy toward the claw to entrap it (Fig. 15-2). (This action helps to avoid accidental contact with the natural lens, especially if the iris prolapses inadvertently, because the constricted iris still covers the optic and forcep.)
- Use the enclavation needle to create a small knuckle of tissue.
- Begin 0.5 mm from the pinpointed spot and push forward so that the spot is at the top of the knuckle.
- Insert the hook of the enclavation needle between both claws of the lens while gently lifting upward, so that the knuckle of tissue becomes entrapped by the claw.
- Perform the second iris entrapment in the same manner.
- Perform an iridectomy at the end of the surgery or after the lens is inserted if the iris tends to prolapse.
- Do not hesitate to reposition the iris-claw lens so that the lens centers on the pupil (Fig. 15-3).
- Close the incision with an “X” using nylon 10-0 suture.
- Be sure to remove all the viscoelastic before suturing. (Remaining viscoelastic may artificially push on the IOL, which could mimic a decentration and deceive the surgeon into recentering the IOL.)
- Place a protective shield on the eye, and ask the patient to wear the shield while sleeping during the first postoperative week.
- Use the enclavation needle to create a small knuckle of tissue.
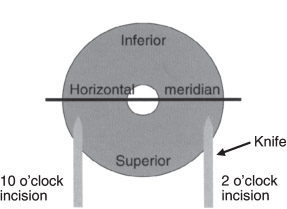
Figure 15-1 Making paracentesis incisions.
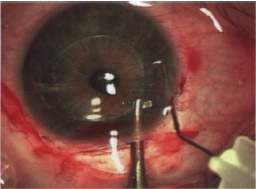
Figure 15-2 Enclavation of the lens. The T-shaped forcep holds the lens near the claw.
Perioperative Complications
- those that occur in standard intraocular surgery
- cystoid macular edema
- transient corneal edema
- endophthalmitis
- wound leaks
- cystoid macular edema
- contact between the phakic IOL and natural lens during insertion (may generate a cataract postoperatively)
- iris prolapse [perform an iridectomy (Fig. 15-4)]
- angle bleeding (occurs if the IOL is slightly pulled inward while performing the second iris entrapment)
- thin iris entrapment
- may cause phakic lensdonesis (see postoperative complications; Fig. 15-6)
- re-enclave the lens
- may cause phakic lensdonesis (see postoperative complications; Fig. 15-6)
- decentration of the IOL (reposition the lens until centered over the pupil)
- loss of AC depth
- a major complication
- immediately remove the IOL
- a major complication
Alternative Treatments
- PRK
- LASIK
- clear lensectomy (for patients with presbyopia or mild lenticular changes)
POSTOPERATIVE CONSIDERATIONS
Medications
- Prescribe antibiotic drops (oflaxacin 0.3% and tobramycin 0.3% plus dexamethasone 0.1%) four times a day for the first month.
Results with Myopia.
- Pop et al
- postoperative refraction of –0.75 ±1.10 D
- 71% of eyes within ±1 D of emmetropia
- no loss of BCVA
- one or more lines of BCVA gained by 26% of eyes
- mild halos or glare for 22% of eyes but no major complications
- only 9% with mild cell flare at 1 month postoperatively
- 26% of mild decentration of 0.25 to 0.5 mm inferior from the center of the pupil
- stable refraction at 1 to 3 months postoperatively
- no contact between the IOL and natural lens
- distance between the lens and posterior surface of the IOL usually 0.78 to 0.93 mm
- the pigment layer of the iris should not be disturbed by the presence of the IOL
- original AC depth reduced by 28 to 34% after implantation
- the pigment layer of the iris should not be disturbed by the presence of the IOL
- postoperative refraction of –0.75 ±1.10 D
- Menezo et al
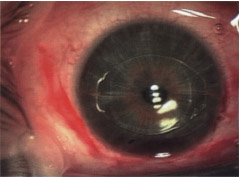
Figure 15-3 View of the irisclaw immediately after surgery.
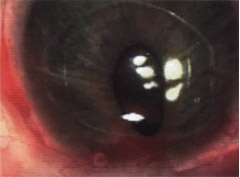
Figure 15-4 Iris prolapse during surgery.

Figure 15-5 Intraocular micrograph of the iris-claw lens in the AC showing normal iris entrapment.

Figure 15-6 Intraocular micrograph of the iris-claw lens in the AC showing thin iris entrapment that may result in phakic lens-donesis (see Postoperative Complications).
- postoperative spherical equivalent of −0.21 ±1.26 D
- 80% of eyes within ±1.00 D of emmetropia and 50% of eyes within 0.50 D of emmetropia
- halos in 23% of eyes (attributable to IOL optic size)
- particularly severe halos in eyes with decentration
- decentration in up to 12% of eyes
- no permanent loss of more than one line of BCVA visual acuity with the convex-concave model
- stable refraction between the first and the third postoperative month
- no cataract formation, retinal detachment, or related cases of glaucoma 2 years postoperatively
- endothelial cell loss of 8 to 17% (cell endothelial injury probably occurs during surgery but morphometric changes in the cells recover after 4 years and gradually approach preoperative levels after slight progressive cell loss after implantation)
Results with Hyperopia
- fewer data available for hyperopic iris-claw lenses (compared with myopic lenses)
- Fechner et al
- spherical equivalent of 0.03 ±1.67 D at 12 months to 10 years postoperatively
- no contact between the IOL and natural lens
- no permanent loss of more than one line of BCVA
- spherical equivalent of 0.03 ±1.67 D at 12 months to 10 years postoperatively
Postoperative Complications
- halos, glare, and starburst
- Considerable halos may result if the pupil is 1 mm larger than the optic diameter.
- Choose optic diameter carefully.
- Considerable halos may result if the pupil is 1 mm larger than the optic diameter.
- endothelial cell loss
- Perform an endothelial cell count at 6, 12, and 24 months postoperatively.
- If abnormal progressive endothelial cell loss occurs, consider removing the lens.
- Perform an endothelial cell count at 6, 12, and 24 months postoperatively.
- pigments released from the iris onto the IOL (rare, but caused by IOL contact with the iris)
- phakic lensdonesis
- Both claws do not entrap enough iris tissue.
- Consider repositioning the lens because of increased risk for endothelial cell loss.
- decentration
- Consider repositioning the IOL if the patient complains of disturbing halos or glare.
- lens dislocation
- Reposition the lens immediately to minimize damage to the endothelium.
- phakic lensdonesis
Enhancements and Secondary Procedures
- Verify if the surgery has increased the amount of astigmatism. (If the incisions are responsible for such an increase, wait for 6 months or for refractive stability, before considering possible enhancements.)
- For ametropia, phakic IOL implantation may be combined with PRK or LASIK.
Postoperative Care and Follow-Up
- Provide each patient with an emergency telephone number so that medical care may be provided as quickly as possible if needed.
- Examine the eye 1 day, 1 and 2 weeks, and 2, 3, 6, 12, and 24 months after surgery.
- Measure manifest refraction.
- Evaluate BCVA and UCVA using Snellen’s chart.
- Perform an endothelial cell count.
- Perform corneal topography.
- Compare current data with previous data on intraocular pressure.
- Verify decentration of the lens over time.
- The AC can be examined with the ultrasound biomicroscope.
Suggested Readings
Fechner P, van der Heijde G, Worst J. The correction of myopia by lens implantation into phakic eyes. Am J Ophthalmol. 1989;107:659.
Fechner PU, Singh D, Wulff K. Iris-claw in phakic eyes to correct hyperopia: preliminary study. J Cataract Refract Surg. 1998;24:48-56.
Guel JL, Vazquez M, Gris O, De Muller A, Manero F. Combined surgery to correct high myopia: iris claw phakic intraocular lens and laser in situ keratomileusis. J Refract Surg. 1999;15:529-537.
Menezo JL, Avino JA, Cisneros A, Rodriguez-Salvador V, Martinez-Costa R. Iris claw intraocular lens for high myopia. J Refract Surg. 1997;13:545-555.
Menezo JL, Cisneros AL, Hueso JR, Harto M. Long-term results of surgical treatment of high myopia with Worst-Fechner intraocular lenses. J Cataract Refract. 1995;21:93-98.
Menezo JL, Cisneros AL, Rodriguez-Salvador V. Endothelial study of iris-claw phakic lens: four years follow-up. J Cataract Refract Surg. 1998;24:1039-1049.
Perez-SantojaJ, Bueno JL, Zato MA. Surgical correction of high myopia in phakic eyes with Worst-Fechner myopia intraocular lenses. J Refract Surg. 1997;13:268-284.
Pop M, Mansour M, Payette Y. Ultrasound biomicroscopy of the iris-claw phakic intraocular lens for high myopia. J Refract Surg. 1999;15:632-635.
Trindale F, Pereira F, Cronemberger S. Ultrasound biomicroscopic imaging of posterior chamber phakic intraocular lens. J Refract Surg. 1998;14:497-503.
< div class='tao-gold-member'>



