14
Pediatric Uveitis
John J. Huang
INTRODUCTION
Uveitis in children covers a wide range of inflammatory and infectious conditions with isolated ocular disease or with associated underlying systemic disease. Uveitis is typically less common in children than adults. Several population studies in the United States and the United Kingdom reported incidence of pediatric uveitis to be 4.3 to 6 per 100,000. There are distinct features of childhood uveitis that require special consideration, and present with unique diagnostic and therapeutic challenges. Thorough eye examination is often difficult and may require examination under anesthesia. Uveitis and systemic manifestation in children also may present very differently such as the lack of pain, photophobia, redness associated with anterior uveitis in juvenile idiopathic arthritis patients, or the lack of pulmonary involvement in pediatric sarcoidosis. Approximately 40% of pediatric uveitis can involve the posterior segment compared to 20% in adults (Table 14.1). The overall prognosis of pediatric uveitis is worse in children than in adults due to delay in the diagnosis and initiation of treatment. Further obstacles in the care of pediatric patients involve the lack or difficulty related to children providing history or visual complaints. The risk of amblyopia is an additional unique concern for pediatric patients under the age of 10. Thus, a disproportionately greater number of children are blinded by their disease compared to adults. The long-term sequelae of suboptimal treatment are devastating for the patient and the parents. Aside from a mandatory screening system for pediatric uveitis and eye diseases, a vigilant parent and pediatrician are critical for recognizing early signs of visual problems.
Table 14.1 Differential diagnosis of pediatric uveitis: anatomical location
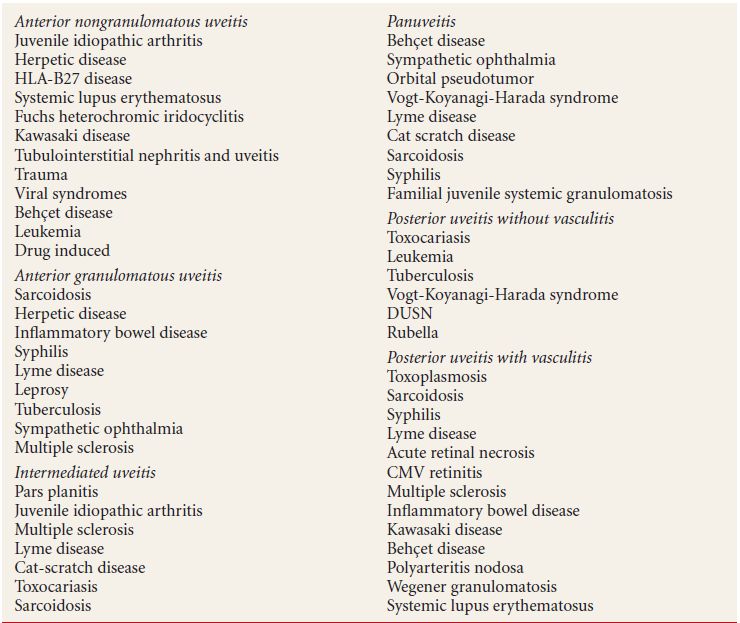
The most common symptoms on presentation in many pediatric uveitis patients are often leukocoria or strabismus, noticed by the child’s parents. The diagnosis of retinoblastoma and other masquerade syndromes must be ruled out prior to additional workup for infectious and noninfectious uveitic entities. A large number of pediatric infectious uveitis are due to the congenital infections and environmental exposures. Early recognition and proper management of these complications related to the intraocular inflammation may reduce the long-term morbidity associated with these disorders. A large number of congenital infections with ocular and systemic manifestations are related to the TORCHES (toxoplasmosis, rubella, cytomegalovirus, herpes simplex or zoster virus, HIV, syphilis) syndrome.
CAUSES AND TREATMENT
The most common cause of noninfectious uveitis in the pediatric population is juvenile idiopathic arthritis followed by HLA-B27-associated uveitis. Inflammation in children should not be tolerated and should always be treated aggressively. The ultimate goal of medical therapy for noninfectious pediatric uveitis is to achieve complete and sustained inflammation control to reduce ocular complications and prevent permanent visual disabilities. As in the treatment of adult uveitis patients, a stepladder approach is utilized. Topical and short-term systemic corticosteroids are often used for immediate disease control. Corticosteroid-sparing medications are used to treat chronic or recalcitrant disease to reduce the risk of cataract formation, glaucoma, and growth retardation. Nonsteroidal anti-inflammatory drugs are often used in combination with corticosteroids or corticosteroid-sparing immunomodulators to reduce the number of flare-ups and the total requirement for topical and systemic corticosteroids. Peripheral cryopexy or indirect laser photocoagulation in selected intermediate uveitis cases cures the disease or reduces dose for therapeutic treatment. Systemic and, more recently, biologic immunomodulation are often used for chronic and recalcitrant disease with significant ocular complications. Finally, pars plana vitrectomy is often used to manage the posterior segment complications related to the chronic inflammation and prevent amblyopia.
HERPES SIMPLEX VIRUS
Herpes simplex virus (HSV) belongs to the herpes family of viruses that also include cytomegalovirus (CMV), varicella zoster virus (VZV), and Epstein Barr virus (EBV). HSV occurs as two types: HSV-1, associated with oral-facial infections and HSV-2, associated with genital infections. HSV infections in the perinatal period is increasingly common with an incidence of 1 in 2,000 to 1 in 5,000 birth per year. The virus establishes latency in sensory neurons and also establishes pathologic lesions upon reactivation. Congenital HSV infection is associated with intrauterine growth retardation, low birth weight, microcephaly, intracranial calcification, encephalitis, seizures, pneumonitis, hepatomegaly, and recurrent cutaneous vesicles. Infants with natal or postnatal HSV infection present with a clinical picture of bacterial sepsis with associated eyelid, oral, and trunk vesicles. Approximately 13% of infants have ocular involvement with unilateral involvement in one third of the cases.
Clinical Findings
- Chorioretinitis or chorioretinal scar
- Cataract
- Optic atrophy
- Corneal ulceration
- Anterior uveitis
Differential Diagnosis
- Toxoplasmosis
- Rubella
- CMV infection
Diagnostic Testing
- Isolation of HSV from vesicular fluid, nasal secretions, and conjunctival secretion
- PCR of aqueous or vitreous fluid
- Test for decreased corneal sensation or evidence of iris atrophy
Treatment
- Intravenous acyclovir 30 mg/kg daily for 10 days to 4 weeks
- Vidarabine as a single infusion 15 to 30 mg/kg over 12 hours
- Oral valacyclovir or famciclovir
JUVENILE IDIOPATHIC UVEITIS
Juvenile idiopathic uveitis (JIA), also known as juvenile rheumatoid arthritis (JRA), is a systemic autoimmune disease that affects approximately 70,000 children in the United States. The etiology of this disorder is multifactorial with a combination of genetic predisposition and microbial trigger. The peak age of onset is between 6 months and 4 years and can be subcategorized into three groups based on the clinical manifestation at onset: systemic, polyarticular, and oligoarticular. Uveitis is rare in the systemic group of patients and is most common in the oligoarticular group with involvement in 20% of the patients. The uveitis in JIA is typically silent with the patient having little or no ocular symptoms. The presentation of uveitis may precede arthritic joint symptoms for long duration, which may further delay diagnosis and treatment. The diagnosis of uveitis is usually made in asymptomatic patients after referral from pediatricians and parents for decreased visual acuity and leukocoria (Table 14.2). Additional marker and risk factors for poor prognosis include positive HLA-DR5 haplotype, positive antinuclear antibody (ANA), female gender, early age of onset, and delay in referral to uveitis specialist. Patients on immunomodulation therapy will typically require more medication for uveitis control than arthritic symptoms. Patients are generally treated and inflammation is controlled for a minimal of 2 years before tapering of the immunomodulation therapy.
Table 14.2 American academy of pediatrics guidelines for ophthalmologic examination in children with JIA
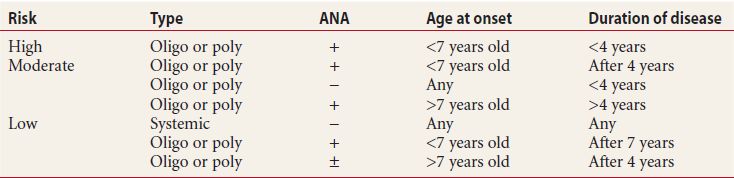
High-risk patients—ophthalmologic exam every 3 to 4 months.
Moderate-risk patients—ophthalmologic exam every 6 months.
Low-risk patients—ophthalmologic exam every 12 months.
Clinical Findings
- Anterior chamber cells
- Band keratopathy
- Extensive anterior and posterior synechiae
- Cataract
- Glaucoma
- Vitreous cells
- Cystoid macular edema in chronic cases
- Hypotony in end-stage patients due to ciliary body damage and cyclitic membrane
Differential Diagnosis
- HLA-B27 associated uveitis
- Sarcoidosis
- Systemic lupus erythematosus
- Fuchs heterochromic iridocyclitis
- Kawasaki disease
- Tubulointerstitial nephritis and uveitis
- Trauma
- Lyme disease
Diagnostic Testing
- ANA
- Rheumatology evaluation
- HLA-DR5
Treatment
- Aggressive topical corticosteroid therapy for immediate inflammation control.
- Periocular corticosteroid injection in severe cases.
- Oral NSAID (naproxen and tolmetin) is often used to reduce the amount of corticosteroids.
- Methotrexate therapy has the longest record for safety and efficacy for the treatment of JIA patients and is often used as the first line therapy.
- Cyclosporine, azathioprine, chlorambucil, intravenous cyclophosphamide, and intravenous immunoglobulin are additional options for recalcitrant cases.
- Etanercept is effective for joint disease but not for ocular inflammation.
- Infliximab is effective for both joint and ocular inflammation.
- Cataract—surgery for cataract is performed only when inflammation is controlled for a minimum of 3 months and intraocular lens are not recommended.
- Glaucoma—Ahmed valve tube shunt is preferred to reduce the risk of hypotony and is preferred over trabeculectomy.
- Vitrectomy is performed in patients with dense vitreitis, vitreous debris, epiretinal membrane, and cyclitic membrane.
LYME DISEASE
Lyme disease is a multisystem infection with occasional ocular manifestation caused by the organism Borrelia burgdorferi. The incidence of Lyme disease is 6.3 per 100,000 population. The organism is transmitted to humans by the infected deer tick Ixodes scapularis in the Northeast, and by Ixodes pacificus in the Western United States. Chronic arthritis has been associated with HLA-DR4 and HLA-DR2 haplotypes. Disseminated disease occurs several weeks after initial infection with hematogenous spread of spirochete to skin, CNS, joints, heart, and eyes. If left untreated, up to 80% of patients develop joint manifestations. Patients can develop a variety of ocular manifestation with keratitis, an immune reaction regarded as active persistent systemic disease. Intraocular inflammation is highly correlated with concurrent CNS infection, and requires neurological dosing regimen. Patients with persistent chronic systemic or ocular disease after a course of proper treatment should also be tested for human granulocytic ehrlichiosis and babesiosis.
Clinical Findings
- Systemic Findings
- Macular rash (erythema migrans), which appears 2 to 28 days after tick bite is the classic bull’s-eye lesion associated with Lyme disease (Fig. 14.1)
- Fever, malaise, fatigue, and arthralgia
- Arthritis
- Meningitis
- Atrioventricular block

Figure 14.1 Large erythema migrans skin lesion shaped like a bull’s eye that appears after exposure to the organism B. burgdorferi.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


