Laser In Situ Keratomileusis
CHAPTER CONTENTS
The Evolution of Lamellar Refractive Surgery
Laser In Situ Keratomileusis as an Enhancement Procedure
Lamellar corneal surgery for the correction of refractive errors has been evolving for 50 years since Professor Jose I. Barraquer of Bogota, Colombia, invented the field in 1948. Many of his concepts continue to guide this particular field of ophthalmic surgery, and much of today’s instrumentation originated from his ideas.
Refractive lamellar corneal surgery attempts to remove, add, or modify the corneal stroma to alter the tear film/anterior corneal interface radius of curvature. For the treatment of myopia, tissue may be removed centrally [i.e., via myopic laser in situ keratomileusis (LASIK)] or added peripherally [i.e., by insertion of an intracorneal ring (ICR)] to induce central corneal flattening and reduction of myopia. For hyperopia, tissue may be added centrally (i.e., through keratophakia), subtracted peripherally (i.e., via hyperopic LASIK), or affected by a deep keratectomy with controlled ectasia [i.e., automated lamellar keratoplasty (ALK) for hyperopia], which may be performed to induce central corneal steepening with a reduction of spherical plus refractive power. Treatment of astigmatism is accomplished by flattening the steep axis or steepening the flat axis (to remove tissue) to make the overall cornea spherical.
THE EVOLUTION OF LAMELLAR REFRACTIVE SURGERY
The surgical techniques used in lamellar refractive surgery have evolved toward increased simplicity and greater patient safety. The end results have been improvement in refractive results and wider acceptance of the procedures by surgeons. Several distinct techniques for performing lamellar surgery exist today.
General Advantages
- ability to treat a larger range of refractive errors
- shorter visual rehabilitation time
- minimal postoperative discomfort
- reduced healing response compared with photorefractive keratectomy (PRK)
- relative ease of enhancement compared with PRK
General Disadvantages
- need for advanced technical expertise
- large ongoing capital expenditures
- potential for serious intraoperative complications (see pp. 121–122)
Instrumentation
- microkeratome (Figs. 11-1 and Fig. 11-2)
- functions like a carpenter’s plane to perform a planar (no refractive power) resection of anterior cornea tissue
- contains an oscillating blade that incises the tissue at an even depth [if intraocular pressure (IOP) is constant and the microkeratome moves across the cornea at a constant velocity]
- functions like a carpenter’s plane to perform a planar (no refractive power) resection of anterior cornea tissue
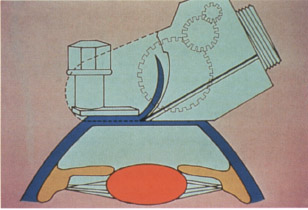
Figure 11-2 Manual Barraquer microkeratome and suction ring. (Courtesy of Stephen G. Slade, M.D.)
Freeze Keratomileusis
The term “keratomileusis” derives from the Greek roots keras (horn-like: cornea) and mileusis (carving). In 1949, Barraquer developed freeze keratomileusis, which alters the cornea’s refractive power by shaping the cornea itself. However, because of its many disadvantages, freeze myopic keratomileusis is no longer performed.
Disadvantages
- steep learning curve for performing the keratectomy and using the cryolathe
- dependence on the constant velocity of the manual microkeratome to maintain the thickness and evenness of the keratectomy
- possibility of irregular astigmatism and a loss of best-corrected visual acuity (BCVA) from any keratectomy irregularity
- difficulty mastering and maintaining skill with the cryolathe
- lack of ability to transfer skills to many other procedures
- availability of better options (e.g., LASIK)
- difficulty placing antitorque sutures
- dependence on the constant velocity of the manual microkeratome to maintain the thickness and evenness of the keratectomy
Indications and Inclusion Criteria
- myopia (≤ −15 to −18 D)
- hyperopia (≤ +6 D)
- not for treatment of astigmatism
Methods (Fig. 11-3)
- Harvest 300 μm of the corneal cap.
- Stain the corneal cap with Chiton-green stain.
- Invert the cap epithelial-side down on a freezing block.
- Sculpt the back (stromal side) surface with a cryolathe (Figs. 11-4 and Fig. 11-5).
- Reposition the cap on the stromal bed.
- Suture the cap in place.
- Remove sutures 2 to 3 weeks after complete epithelialization.
Keratomileusis In Situ for Myopia
Barraquer also conceived the process of raising a corneal cap and removing central tissue from the bed. Krwawicz and Pureskin described similar techniques as “central stromectomy.” Because of several disadvantages and the frequency of certain complications, this technique is no longer practiced.
Disadvantages
- availability of a better option (i.e., LASIK)
- difficulty placing antitorque sutures
Indications and Inclusion Criteria
- myopia (≤ –18 D)
- not for treatment of astigmatism

Figure 11-4 Surgical team member operating the cryolathe. (Courtesy of Stephen G. Slade, M.D.)

Figure 11-5 Cryolathing of a lamellar corneal disk. (Photo courtesy of Stephen G. Slade, M.D.)
Methods (Figs. 11-6)
- Create a free cap to gain access to the corneal stroma using a manual pass of the microkeratome.
- Remove a smaller-diameter disc of tissue with a second pass of the microkeratome across the stromal bed.
- Determine the size of the refractive correction with the thickness of the second “power cut.”
- Replace the cap to reduce corneal curvature and myopia.
- Suture the cap in place using an antitorque technique.
Complications
- infection
- irregular astigmatism (frequent)
- loss of cap
- lamellar complications (epithelial ingrowth and flap melting)
Keratophakia
Keratophakia means “corneal lens.” Barraquer first developed the procedure keratophakia in the 1960s as a treatment for aphakia after intracapsular cataract extraction. With the advent of extracapsular and phacoemulsification cataract surgery techniques along with improved intraocular lens (IOL) technology, keratophakia has been relegated to a lesser role; surgical aphakia is no longer a prevalent problem. The future role of keratophakia or corneal inlay techniques in refractive surgery may involve the addition of synthetic tissue or lens material under a flap or placement of a transparent material of a different (or same) index of refraction from the corneal stroma in a stromal pocket to correct myopia, hyperopia, astigmatism, or presbyopia.
Indications and Inclusion Criteria
- hyperopia (typically ≤ ∼6D)
- aphakia (≤ 14 D)
- not for treatment of astigmatism
Methods (Fig. 11-7)
- Create a flap and/or cap.
- Place a disc of tissue underneath the flap and/or cap to increase the central corneal curvature.
- Typically, harvest the tissue to be added from donor corneal tissue using a microkeratome.
- Select a specific disc diameter and thickness of tissue based on the patient’s refractive error.
Complications
- infection
- irregular astigmatism
- loss of cap
- lamellar complications(epithelial ingrowth and flap melting)
- decentration of lens inlay
- loss of BCVA
Barraquer-Krumeich-Swinger Nonfreeze Keratomileusis Technique
The goal of the Barraquer-Krumeich-Swinger (BKS) technique was the improvement of refractive results and the simplification of lamellar surgery. The procedure is no longer performed.
Advantages
- avoidance of adverse tissue effects (loss of fibroblasts) associated with freezing of the corneal cap
- preservation of the corneal epithelium with a more comfortable postoperative course of healing
- light processing of the tissue
- maintenance of the intact epithelium
Disadvantages
- availability of a better option (i.e., LASIK)
- technical difficulty performing refractive keratectomy
- difficulty placing antitorque sutures
- frequency of postoperative irregular astigmatism
Indications and Inclusion Criteria
- myopia (≤ −18 D)
- hyperopia (≤ +6 D)
- not for treatment of astigmatism
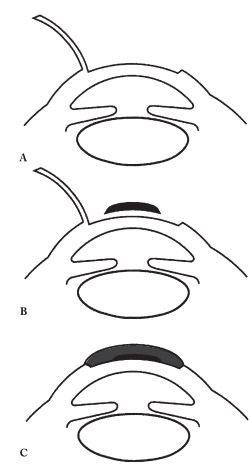
Methods (Figs. 11-8 and Fig. 11-9)
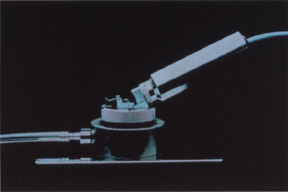
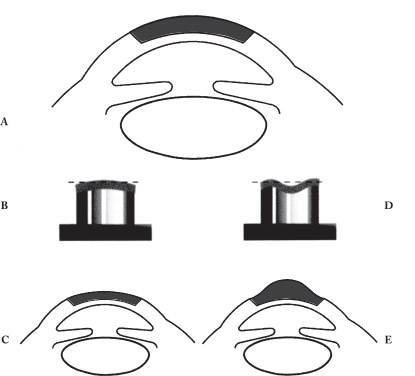
Figure 11–9 Barraquer-Krumeich-Swinger keratomileusis technique. (A) 300-μm cap created with microkeratome. (B) Cap placed epithelial-side down on suction dye. Stroma removed from central aspect of the posterior aspect cap with manual microkeratome. (C) Cap reposited with antitorque sutures. Central cornea flattened for treatment of myopia. (D) Cap placed epithelial-side down on suction dye. Tissue removed from paracentral stroma of posterior cap with manual microkeratome. (E) Cap reposited. Corneal curvature has been steepened for treatment of hyperopia.
- Harvest a 300-μm corneal cap using the BKS microkeratome.
- Place the cap epithelial-side down on one of several specific suction dyes.
- Choose the suction dye based on the planned diopter correction of myopia or hyperopia (Fig. 11-10).
- Make the refractive cut with the microkeratome.
- Suture the cap in place with the antitorque technique.
Complications
- infection
- irregular astigmatism (frequent and major drawback)
- loss of cap
- lamellar complications (epithelial ingrowth and flap melting)

Figure 11-10 Barraquer-Krumeich-Swinger suction dyes. (Courtesy of Stephen G. Slade, M.D.)
Epikeratophakia
The first “Americanized” version of a lamellar refractive surgery technique was epikeratophakia/epikeratoplasty as described by Kaufman and Werblin. What seemed to be a modernization of lamellar surgery ultimately was not a viable alternative.
Advantages
- automation of the difficult task of using the cryolathe
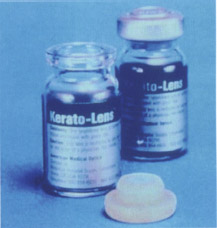
- provision of a high-quality, preprocessed refractive corneal lenticule from a centralized manufacturer that freezes and cryolathes specific corrective powers, lyophilizes the lenticule in a sterile bottle (Fig. 11-11), and then ships it to the surgeon.
Disadvantages
- variability of surgical results
- poor profitability for the manufacturer of the lenticules
- emergence of better alternative therapies (e.g., IOLs and laser refractive techniques)
Indications and Inclusion Criteria
- treatment of the following for children and adults
- aphakia
- myopia
- hyperopia
- keratoconus
- keratoglobus
- aphakia
- not for treatment of astigmatism
Methods
- Reconstitute the lenticule with balanced salt solution (BSS).
- Suture the lenticule onto the eye after host-bed preparation (Fig. 11-12).
Complications
- those associated with re-epithelialization over the donor lenticule
- infection
- irregular astigmatism
- loss of cap
Automated Keratomileusis In Situ
The next major advance in the field of lamellar refractive surgery was development of the motorized Ruiz microkeratome, which was invented by another Colombian surgeon and protégé of Barraquer, Dr. Luis Antonio Ruiz. ALK is no longer performed.
Advantages
- gears that advance the microkeratome across a geared track
- an adjustable-height suction ring (defined the technique now known as ALK; Fig. 11-13)
- a constant passage velocity
- a lamellar tissue disc of even thickness
- a smoother corneal stromal bed
- increased appeal for a larger number of surgeons who found manual microkeratomes difficult to master

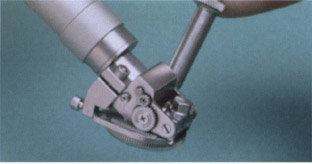
Figure 11–13 Automated geared microkeratome and geared-track of suction ring.
Disadvantages
- availability of a better option (i.e., LASIK)
- abandonment of the hyperopic technique because of concern about progressive ectasia
- technical demands of procedure
Indications and Inclusion Criteria
- myopia (≤ – 20 D)
- hyperopia (≤ +6 D)
- not for treatment of astigmatism
Methods
- Perform ALK in an outpatient setting with topical anesthesia (oral sedation is optional).
- Irrigate the conjunctival cul-de-sacs to remove debris and eyelid glandular secretions.
- Clean eyelids in the standard manner with povidone-iodine solution (Betadine).
- Drape the eyelids.
- creates a clear path for microkeratome passage
- removes the lashes and extraneous periocular tissue from the surgical field
- creates a clear path for microkeratome passage
- Instruct the patient to look at the microscope light.
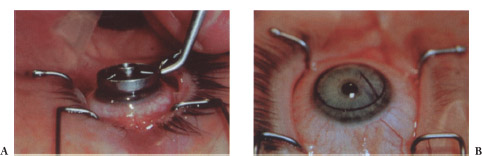
- With an inked marker, delineate the optical center, a pararadial line for orientation of the flap, and a 9-mm optical-zone (OZ) circle to center the circular suction ring (Fig. 11-14).
- Place a spacer device (or depth plate) in the microkeratome to determine the thickness of the cut. (The first keratectomy in ALK typically utilizes a 160-μm depth plate.)
- Place an adjustable suction ring on the eye and engage the suction to do the following.
- fixate the globe
- provide a geared path for the microkeratome
- raise the IOP to allow presentation of adequate corneal tissue (enables a smooth keratectomy of even thickness)
- Create a hinge in the corneal flap with a stopper device.
- Just prior to passage of the microkeratome, use a hand-held Barraquer tonometer to check the IOP to ensure that it is greater than 65 mmHg.
- Remove the suction ring after the first cut, which has a planned diameter of 7.5 to 8.0 mm.
- Reset the adjustable suction ring to resect a 4.2-mm-diameter piece of stromal tissue.
- Place a second depth plate, which corresponds to the planned myopic correction.
- Replace the suction ring and make a second cut (the “power cut”) after checking the diameter and the IOP.
- Replace the flap and position it without sutures.
- Protect the patient’s eye with a clear, plastic orbital shield (Fig. 11-15) and discharge the patient with broad-spectrum topical antibiotics
- Examine the eye the next day.
- Place an adjustable suction ring on the eye and engage the suction to do the following.
Complications
- infection
- irregular astigmatism
- loss of cap
- lamellar complications (epithelial ingrowth and flap melting)
- significant loss of BCVA (5-10% in some studies)

LASER IN SITU KERATOMILEUSIS
The postoperative complications of central corneal haze, regression of effect, and diminished efficacy for myopia over – 6 D with excimer laser PRK and the predictable shortcomings of ALK led to the development of LASIK. Researchers substituted lasers for the keratome in the refractive correction step of the myopic ALK procedure and LASIK was born. Some researchers postulated that the submicron ablation precision of the excimer laser allows for much more predictable refractive results that do not depend as heavily on individual patient healing responses, as had been noted with PRK.
Preoperative Considerations
Advantages
- incredible precision of tissue removal
- minimal postoperative discomfort
- early recovery of visual function
- immediate return to preoperative lifestyle
- lack of topical steroid usage
- lack of concern for undesirable healing phenomena (e.g., haze formation)
- a short postoperative antibiotic regimen
- less-intensive follow-up than that for PRK
- increased range of efficacy for myopia, hyperopia, and astigmatism (compared with PRK)
Indications and Inclusion Criteria*
- myopia (0.5-15.0 D)
- hyperopia (0.5-6.0 D)
- regular astigmatism (≤8D)
- patient at least 18 years of age (as for refractive surgery in general)†
- refractive stability (≥ 12 months)
- clarity of the crystalline lens
- education about the alternative refractive surgical procedures (e.g., radial keratotomy, PRK, ICR segments, clear lens extraction, or phakic IOL placement)
- evaluation of patient expectations
- completion of informed consent form
Preoperative Patient Evaluation
- visual acuity testing
- refraction
- manifest refraction (duochrome test and fogging techniques)
- cycloplegic refraction (to check excessive accommodation during manifest examination)
- comparison of refraction with prior spectacle corrections to assess the stability of refraction
- discontinuation of soft contact lens wear at least 3 days to preferably 2 weeks prior to examination
- discontinuation of rigid gas-permeable (RGP) lens wear at least 3 weeks before first of at least two examinations performed 3 days apart
- at least 0.25 D difference in refraction (validates stability)
- manifest refraction (duochrome test and fogging techniques)
- evaluation of central corneal thickness using pachymetry (assesses safe limits of corneal stromal removal with laser ablation by measuring flap thickness, depth of ablation, and residual thickness of the stromal bed after ablation)
- A thin flap more likely leads to irregular astigmatism and lost lines of BCVA.
- A flap at least 160 μm thick minimizes induced irregular astigmatism.
- A thin stromal bed (<250 μm) may increase the likelihood of central ectasia with long-term unstable refractive status.
- For example, central pachymetry (560 μm) – flap thickness (160 μm) = preablation stromal bed (400 μm) so in this case ablate no more that 200 μm of stromal bed.
- Based on the Munnerlynn formula (ablation depth = optical zone2 X diopters treated/3), no more than 15 D of myopia could be treated if using a 6-mm OZ.
- If preoperative central corneal thickness is thinner and ablation still leaves a 200-μm-thick stromal bed, less refractive error may be treated safely.
- Multizone ablations can correct larger amounts of refractive error because less tissue is removed than with single-zone ablations (overall OZ is smaller and night vision may be compromised).
- If preoperative central corneal thickness is thinner and ablation still leaves a 200-μm-thick stromal bed, less refractive error may be treated safely.
- A thin flap more likely leads to irregular astigmatism and lost lines of BCVA.
- computerized videokeratography
- slit-lamp examination
- retinal evaluation
- eye-dominance testing
- evaluation for monovision (when appropriate) (see p. 66)
- evaluation for astigmatism
- refraction
- keratometry
- videokeratography
- refraction
- formulation of nomogram
- Lasers come with algorithms for treating a specific refractive error.
- Surgical technique, ideal room conditions (humidity, 30-50%; temperature, 18–24°C; filtration of low air particulate matter), and laser components (quality of optics, gas mixture) directly impact the refractive result and are laser algorithm-independent but addressed by the individual surgeon nomogram.
- Clearly follow a methodical calculation scheme when determining what data to enter into the laser for each eye to be treated.
- A worksheet in the patient’s chart prevents calculation mishaps (Table 11.1).
- Lasers come with algorithms for treating a specific refractive error.
* These ranges are not absolute; many surgeons have successfully treated patients with myopia, hyperopia, or astigmatism beyond these ranges. Other surgeons may work at lower ranges based on their personal experience with the procedure.
† The use of LASIK for equalization of refractive error between eyes of pediatric patients has been done outside the United States but remains controversial.
Absolute Contraindications
- unstable refraction
- keratoconus
- irregular astigmatism
- inadequate corneal thickness
- active corneal or ocular disease
Relative Contraindications
- thin corneas
- active collagen vascular disease
- systemic vasculitis
- low endothelial cell counts (<500-1500 cells/mm2)
- anterior basement dystrophy
- history of recurrent erosions (an epithelial defect can occur during the keratectomy and lead to poor flap adhesion with subsequent epithelial ingrowth and flap melting; surgeon experience helps to avoid epithelial ingrowth)
- pregnancy or lactation (may be considered if stable through prior pregnancies and have no refractive change from current eyewear; J.F.D. has treated several pregnant and lactating women after careful consent and thorough evaluation of their previous refraction history)
- history of herpes simplex or herpes zoster keratitis (use prophylactic oral and/or topical antiviral agents perioperatively because of risk for stromal melting; proceed very carefully with these patients)
- patients with monocular vision
| Line 1 (preoperative refraction) | −6.0 D sphere |
| Line 2 (postoperative target) | piano |
| Line 3 (line 1-line 2) | −6.0 D sphere |
| Line 4 (% reduction or addition; presume 90% of sphere) | −5.4 D sphere |
| Line 5 (treatment entered into laser) | −5.4 D sphere |
Surgical Considerations
At least two different techniques have been used for laser myopic keratomileusis: LASIK and the Buratto technique. LASIK is now the predominant technique because the sutureless hinged flap is significantly easier to deal with compared with correctly orientating a free cap onto the stromal bed (Fig. 11-16 and Fig. 11-17). The Buratto technique is analogous to freeze myopic keratomileusis (MKM) except for substitution of the excimer laser for the cryolathe in the refractive step of the procedure.
- LASIK
- Create a hinged flap.
- Remove corneal stroma from the bed with the laser.
- Treat sphere and cylinder depending on the capabilities of the laser (Figs. 11-18 to Fig. 11-20).
- Create a hinged flap.
- The Buratto technique
- Remove a thick disc of tissue (300-350 μm) completely from the eye.
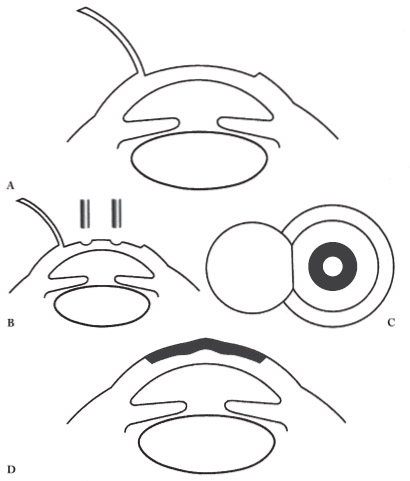
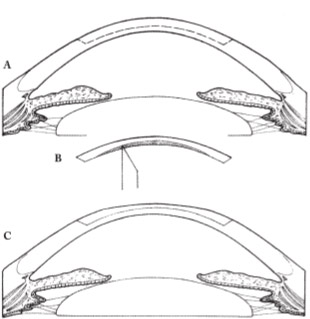
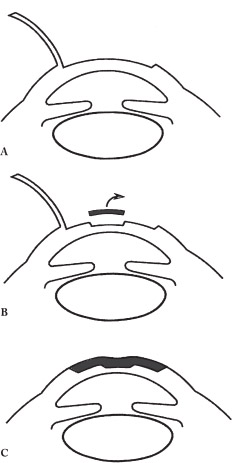
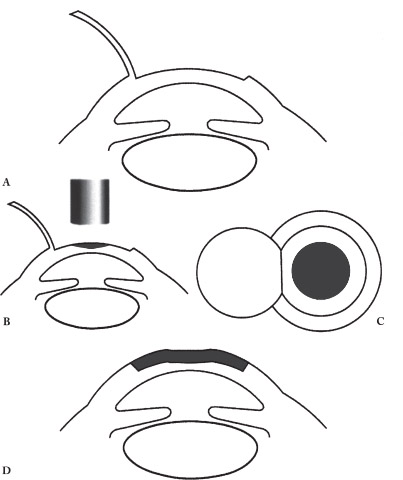
Figure 11-17 Laser in situ keratomileusis for hyperopia. (A) Creation of flap. (B) Laser ablation of stromal bed and paracentral tissue removal (shaded area). (C) Shaded area represents zone of tissue removal (top view). (D) Flap replaced and central cornea steepened.
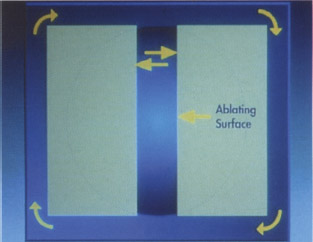
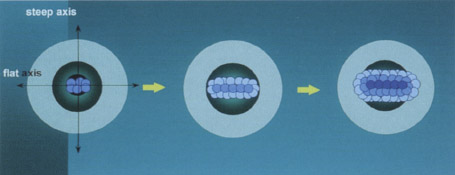
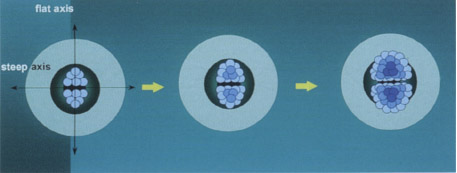
Figure 11–20 Schematic of plus cylinder ablation with scanning spot laser to steepen the flat axis by removing tissue paracentrally parallel to the minus cylinder axis or the flat axis on keratometry.
- Place the disc beneath the laser stroma side up and ablate with the excimer laser (Fig. 11-21)
- Replace the disc of tissue on the eye.

Instrument Setup and Surgical Team Mentality
- Select a laser depending on desired ablation depth. 0 most lasers: 12 to 15 μm/D (in 6-mm single zone algorithms)
- VISX Star (VISX, Inc., Santa Clara, CA): 15 μm/SE diopter (6-mm single-zone algorithm)
- VISX Smoothscan: 12 μm/SE diopter (6-mm single-zone algorithm)
- VISX Star (VISX, Inc., Santa Clara, CA): 15 μm/SE diopter (6-mm single-zone algorithm)
- Consider the amount of residual stroma.
- 160-μm plate leaves a 150 ± 20 μm flap
- 200 to 250 μm should be left in stromal bed (U.S. Federal Department of Agriculture now recommends 250 μm)
- ideal total corneal thickness = 150 + 250 μm
- 160-μm plate leaves a 150 ± 20 μm flap
- Select a keratome based on keratometry values (Ks).
- Ks <42.0 D [200-μm plate with the Automated Corneal Shaper (ACS) or Hansatome (Bausch & Lomb, Rochester, NY)]
- Ks = 42-46 D (160-180 μm plate with ACS or Hansatome)
- Ks> 46 D (160-μm plate or Hansatome)
- Ks <42.0 D [200-μm plate with the Automated Corneal Shaper (ACS) or Hansatome (Bausch & Lomb, Rochester, NY)]
- Properly clean, assemble, and test the microkeratome.
- Calibrate and set up the laser.
- Check fluence (proper energy setting in mJ/cm2).
- Check beam homogeneity (evenness of energy distribution across surface area).
- Each team member is responsible for every aspect of the procedure and should complete multiple checks as the procedure progresses.
- Check fluence (proper energy setting in mJ/cm2).
- Ensure appropriate humidity, temperature, and air purification in the laser room at all times to preserve laser optics and establish standardized treatment conditions.
Patient Preparation
- Administer 5 to 10 mg of diazepam orally approximately 45 min prior to the procedure.
- Do not use a preoperative miotic.
- Irrigate the conjunctival fornices with eyewash to remove any meibomian secretions or tear-film debris.
- Clean eyelids with Betadine.
- Position the patient under the laser in the supine position with the frontal surface of the cornea perpendicular to the laserbeam aperture.
- Instill 1 to 2 drops of a mild topical anesthetic (e.g., proparacaine).
- Dry the eyelashes with a gauze sponge and place a fenestrated drape over eyelashes to keep them and redundant periocular tissues out of the surgical field.
- Insert a wire-locking eyelid speculum (allows adequate exposure).
The Keratectomy
- Open the speculum another 1 to 2 mm after waiting 1 min after initial insertion.
- Mark the corneal epithelium with a lamellar corneal surgery marker (useful for proper positioning of a free cap; see Fig. 11-14).
- Place the LASIK pneumatic suction ring onto the eye to provide globe fixation, elevation of IOP to create an even-thickness keratectomy, and a track for the advancement of the microkeratome.
- Press down suction ring.
- After activating the vacuum to the pneumatic suction ring, directly check the IOP using a Barraquer tonometer, pneumotonometer, or digital palpation.
- Ensure that the path of the microkeratome is clear.
- Pull down the lower lid with the Hansatome.
- After obtaining sufficient IOP, lubricate the corneal surface with BSS or proparicaine to minimize epithelium disruption while making a pass with the microkeratome.
- Load the microkeratome into the dovetailed groove on the suction ring and then advance and reverse it.
- Double depress at the end of the cut to ensure completion.
- Discontinue vacuuming and remove the LASIK suction ring or hold the eye with the suction ring while suction is off during the laser ablation.
Laser Ablation
- Before lifting the flap, the surgeon and staff should confirm proper laser settings and position the patient’s head so that the corneal surface is perpendicular to the ablation beam.
- Lift the flap and fold it out of the ablation field.
- Center the ablation over the entrance pupil (critical for hyperopes).
- Monitor the centration cautiously.
- If significant movement occurs, stop the ablation, reorient the patient (center eye by raising patient’s chin and turn head nasally for small palpebral apertures), and proceed when the centration is aligned.
- Use an eye tracker or eye fixation for nystagmus, mobile eyes, or hyperopic eyes.
- Monitor the centration cautiously.
- Turn down the microscope light.
- Wipe dry any ablation fluid that accumulates on the corneal surface with a single pass of a nonfragmenting cellulose sponge or blunt spatula.
- As the ablation proceeds to the largest-diameter treatment zones, cover the hinge with a blunt instrument, if necessary, to prevent ablation of the back surface of the corneal flap.
- If treating concurrent astigmatism, ensure the appropriate axis of treatment by marking a reference point on the patient’s limbus prior to initiating the treatment session.
- If significant cyclotorsion occurs when placing the patient in the supine position, adjust the axis that is programmed into the laser.
- Correct astigmatism by differentially removing tissue in the frontal plane of the cornea in one of the two major meridians (flatten the steep axis, steepen the flat axis, or perform crossed-cylinder ablation).
- minus cylinder format [Flatten the steep axis by using large-area ablation lasers with closing blades (see Fig. 11-18), masking systems, or flying-spot lasers by passing the spot parallel to the minus cylinder axis or flat axis on keratometry (see Fig. 11-19). It is best used for myopic astigmatism because it minimizes tissue removal.]
- plus cylinder format [Steepen the flat axis best with scanning-spot lasers by removing tissue paracentrally parallel to the minus cylinder axis or flatter axis on keratometry (see Fig. 11-20). It is best used for hyperopic astigmatism because it minimizes tissue removal.]
- crossed cylinder format [Use this method for mixed astigmatism in which each major meridian receives a combination of steepening or flattening, respectively (Fig. 11-22).]
- minus cylinder format [Flatten the steep axis by using large-area ablation lasers with closing blades (see Fig. 11-18), masking systems, or flying-spot lasers by passing the spot parallel to the minus cylinder axis or flat axis on keratometry (see Fig. 11-19). It is best used for myopic astigmatism because it minimizes tissue removal.]
Repositioning the Flap
- Gently float the flap into the stromal bed at the completion of the laser ablation.
- Place a small-gauge cannula underneath the flap and irrigate for 5 to 10 sec with BSS in a closed system to clear any remaining debris from the interface (increased irrigation time decreases adhesion of the flap and leads to flap edema with greater flap-edge gape; Fig. 11-23).
- Inspect the flap to ensure proper positioning by verifying that an equal gutter (keratectomy edge) distance is present throughout the circumference (Fig. 11–24).
- Check corneal alignment marks.
- Allow the interface to dry for several minutes.
- During the drying phase we recommend that you administer a microdrop of BSS over the central corneal epithelium to maintain its integrity.
- Test flap adhesion by performing a striae test.
- Depress the peripheral cornea with closed blunt-tipped forceps.
- When striae pass well into the flap 360 degrees, you have achieved appropriate adhesion.
- Depress the peripheral cornea with closed blunt-tipped forceps.
- Remove the speculum and drape.
- Reexamine the eye to ensure that the flap is properly positioned.
- Instill a topical broad spectrum antibiotic (Ciloxan; Alcon) and nonsteroidal antiinflammatory medication drop (Voltaren; Ciba Vision).
- Place a shield over the orbit but do not apply a pressure patch.
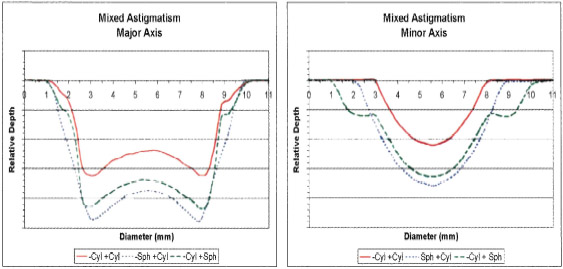
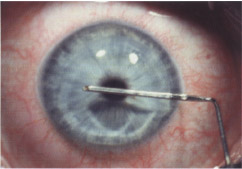
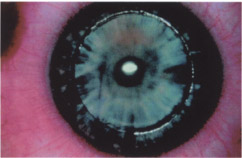
Figure 11-24 The reposited flap should be inspected for equal gutter/keratectomy edge distance throughout its circumference. (Courtesy of Stephen G. Slade, M.D.)
Postoperative Considerations
Typical postoperative care of a LASIK patient is relatively simple.
Results
- generally no pain
- foreign body sensation, light sensitivity, and tearing (typically present for the first few hours after surgery)
- uncorrected visual acuity (UCVA) of 20/40 or better in the low and moderate myopia treatment ranges
- a clear cornea with intact epithelium on slit-lamp examination
- proper flap apposition (check)
- stromal edema or interface debris (document)
Patient Management
- Prescribe topical prophylactic antibiotics 4 times a day for the first week.
- Prescribe topical corticosteroids for the first 4 to 7 days postoperatively.
- Topical preservative-free lubricating drops may help select patients (as needed) for several weeks after surgery.
- Use an orbital shield to protect the globe from direct pressure during the first 3 to 4 nights.
- Systemic analgesics are rarely necessary.
- Instruct the patient to resume normal activities after the 1 day postoperative examination (if results are normal), but caution the patient to avoid rubbing the cornea and participating in contact sports without proper eye protection.
- Instruct the patient to avoid exposure to potentially contaminated moisture sources such as hot tubs, pools, and fresh-water lakes for at least 2 weeks.
- Tell the patient that full visual recovery may take several weeks or more and may be delayed if significant irregular astigmatism exists.
FLAP COMPLICATIONS Flaps may be too short, too thin, irregular, or free (free cap) (Fig. 11-25 to Fig. 11-27). An alteration of the various forces during the LASIK procedure (Table 11-2) may explain their occurrence.
Prevention
- Properly assemble and prepare the microkeratome.
- Training the surgeon and staff is the cornerstone for achieving reproducible high-quality lamellar incisions.
- Confirm adequate (> 65 mmHg) suction levels. [Use a Barraquer tonometer or pneumotonometer to check dilation of the pupil, dimming of the patient’s vision, adherence of the suction ring, level of the suction pressure meter of the base unit, or pressure on palpation with fingertip (i.e., digital pressure).]
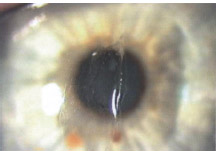
Figure 11-25 A centrally perforated flap immediately after LASIK.

Figure 11–26 A horizontal linear flap defect because of a defective blade 4 months after LASIK.
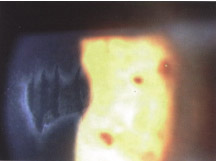
Figure 11-27 A central flap perforation with skip marks 2 months after LASIK.
| Flap Complication | Mechanism |
|---|---|
| Perforated cornea | Absence or incomplete insertion of depth plate |
| Short flap | Obstruction of microkeratome path |
| Thin flap | Inadequate or lost suction |
| Irregular flap | Inadequate or lost suction |
| Button-hole flap | Inadequate or lost suction |
| Ks> 48.0 D | |
| Mechanical theory of conservation of length leading to central corneal buckling and button-hole flap formation | |
| Free flap | Ks <41.0 |
| No microkeratome stop screw |

Figure 11-28 Interface blood immediately after LASIK.
Management
- Abort the excimer laser correction (may further alter the irregular stromal bed and affect the final result).
- Leave the flap in place or replace it as precisely as possible into the stromal bed and leave it for at least 5 min.
- Monitor the eye weekly for epithelial ingrowth (more common after thin-flap complications).
- Consider a repeat LASIK procedure after 3 months using a deeper depth plate (180 or 200 μm).
- A free cap may still achieve an excellent outcome with laser treatment in the stromal bed and replacement of the cap.
CORNEAL NEOVASCULARIZATION Prolonged contact-lens use can cause neovascularization of the peripheral cornea. Vessels may be cut during the keratectomy step of LASIK and result in bleeding onto the stromal surface of the ablation bed (Fig. 11-28).Other etiological factors may be at work.
- large 9.5-mm keratectomy with Hansatome or other hyperopic rings
- a corneal scar or phlyctenule
- pterygium
- decentered keratectomy
- small cornea or microcornea
Prevention
- To avoid neovascularization, decenter the flap slightly inferiorly.
- Avoid using the large 9.5-mm ring of the Hansatome on small steep corneas.
- Anticipate bleeding in eyes with corneal scars that are associated with patent blood vessels.
Management
- Corneal neovascularization usually stops without treatment in a few minutes.
- Monitor any blood that extends onto the stromal bed to ensure that it does not move into the ablation zone of the laser.
- Absorb blood with a dry Murocel sponge as it progresses toward the ablation area.
- Temporarily arrest bleeding using direct pressure from the suction ring during the ablation process.
- Once ablation is complete, replacement of the corneal flap often tamponades further bleeding.
- Persistent corneal bleeds require additional treatment.
- To treat persistent corneal bleeding, locally apply a Murocel sponge soaked with Tobradex, 0.1% dexamethasone, 2.5% phenylephrine, or 0.5% aproclo-nidine.
- Apply filtered compressed air.
- Dry gently with a dry Murocel sponge.
PERFORATION OF THE CORNEA This extremely rare event may occur when LASIK is performed with the ACS (but without proper insertion of the depth plate) or any other microkeratome that allows insertion and removal of depth plates. The perforation becomes obvious when the microkeratome advances. Signs and symptoms of corneal perforation include:
- patient complaints of sudden pain
- the sudden appearance of intraocular fluid in the operative field
- a sudden drop in suction pressure of the suction ring
- the presence of extruded intraocular contents with a flat anterior chamber, peaking of the iris, or extrusion of the crystalline lens when reversing the microkeratome
Prevention
- This problem is best prevented by carefully inspecting the equipment before each case of LASIK.
- Use the “pre-flight checklist” advocated in training programs for technicians and surgeons to check the depth of keratome plate insertion before each use.
- Use the newer Hansatome with its fixed unremovable depth plate.
Management
- As soon as penetration is suspected, release the suction to minimize extrusion of the ocular contents.
- Gently remove the microkeratome from the eye.
- Place sutures across the corneal incision to stabilize the eye and then cover the cornea with a contact lens.
- Arrange for emergency referral to a surgeon who is comfortable with repair of the anterior segment.
POSTOPERATIVE PAIN Most patients do not experience pain following LASIK because of minimal epithelial disruption and the regularity of the post-LASIK corneal surface. Postoperative pain has many causes:
- epithelial defect
- dislodged flap
- toxic epithelial keratopathy
- residual pressure from suction ring/lid speculum
- infection (rarely)
Prevention
- Ensure that the procedure is as atraumatic as possible.
- Minimize the use of preoperative topical anesthesia to reduce postoperative epithelial toxicity.
- Administer 1 drop of a topical nonsteroidal medication to reduce the immediate foreign-body sensation.
- Advise patients to avoid rubbing or squeezing the eye because it may disturb flap position and cause significant pain.
Management
- Address any complaint of significant pain by performing an eye examination to ensure that the flap is in place and the epithelium is intact. (You will usually identify no major problems.)
- Administer a mild narcotic to assist with sleeping to reassure the patient.
- Provide topical nonsteroidal drops and lubrication drops to help control pain related to epithelial defects.
- Immediately treat the superficial punctate keratitis identified on the flap epithelium with generous lubrication.
EPITHELIAL DEFECTS Epithelial defects, which cause postoperative pain and a foreign-body sensation, are generally evident immediately after performing the keratectomy and most commonly form along the superior aspect of the keratectomy edge when using the Bausch and Lomb ACS (Rochester, NY) or the Hansatome (Fig. 11-29). The risk for epithelial ingrowth increases after stimulation of epithelial healing and growth begins. Etiology includes:
- anterior basement membrane dystrophy (ABMD) (Patients with ABMD commonly develop these defects; there is an even higher incidence for enhancements.) (Fig. 11-30)
- a history of recurrent corneal erosions (Patients with loose epithelium such as those with ABMD or a history of recurrent corneal erosions are best treated with PRK.)
- epithelial toxicity from topical anesthesia
- operative trauma/manipulation
- history of dry eye
- insufficient wetting of the corneal surface prior to passage of the microkeratome
- advanced age (Patients >45 years old tend to have a less adhesive epithelium to Bowman’s membrane and frequently the epithelium is sloughed when the micro -keratome is reversed.)
Figure 11–29 Loose epithelium with a defect along the flap edge immediately after LASIK.
Figure 11–30 Typical appearance of the map lines of ABMD.
Signs and Symptoms
- significant pain
- prolonged visual recovery
- epithelial ingrowth
- flap melt
- infection
- LASIK interface inflammation (the “sands of Sahara”)
Prevention
- Use topical anesthesia sparingly (once under the laser) to avoid any epithelial toxicity.
- Keep the corneal surface well lubricated to prevent epithelial irritation.
- Perform all surgical maneuvers with great delicacy to avoid any epithelial trauma.
- Use a modified technique if the patient has known ABMD.
- Do not mark the cornea.
- Perform a very wet (copious corneal irrigation prior to passage of the microkeratome) keratectomy to minimize friction between the depth plate and epithelium.
- To minimize sloughing of the epithelium, discontinue the vacuum at the completion of the forward pass of the microkeratome, and lift off the microkeratome and suction ring manually from the eye with the flap sliding out of the corneal shoot with minimal to no friction created over the epithelium.
Management
- Copiously lubricate the patient’s eye and administer a topical prophylactic antibiotic drop to guard against infection daily until the defect heals.
- Small epithelial defects (<3 mm) generally heal quickly in 24 hr, so a postoperative nonsteroidal drop and a good sleep restore eye comfort.
- Treat larger epithelial defects with a contact lens, which reduces postoperative pain, lacrimation, and eyelid squeezing and generally remove it after 1 to 2 days.
- Alternatively, apply tincture of benzoine to the forehead and cheek skin and pull the lids together with paper tape to prevent blinking but do not apply gauze or a dressing beneath the tape. (This technique achieves minimal to no anterior-posterior pressure, only inferior-superior suspension.)
- Follow patients with epithelial defects weekly for 1 month to monitor for epithelial ingrowth.
Figure 11-31 Grade 3 LIK with dense clumping of cellular material in the interface 3 days after LASIK. UCVA had dropped to 20/200 and BCVA was 20/50.
LASIK INTERFACE KERATITIS Laser interface keratitis (LIK), or the “Sands of Sahara” syndrome, presents as interface inflammation in the 24- to 72-hour postoperative period. The interface inflammation has a “sifted sand” appearance with a dusting of a powder-like material in the interface that generally is more dense centrally (Figs. 11-31 and Fig. 11-32). The rest of the eye is usually unaffected with no conjunctival injection, anterior chamber inflammation, epithelial defects, or corneal infection (unilateral in 70% of cases). There are four grades of LIK (Table 11-3). Likely causes include:
- betadine
- benzene
- BSS
- contaminants from eyelids
- contaminants on instruments (consecutive serial cases on the same day with same instruments and surgeon)
- corneal abrasions
- laser thermal effect
- lubricant
- meibomian gland secretions
- metallic debris
- talc
- topical medications
- bacterial endotoxin or exotoxin
- endotoxins released from the cell walls of dead bacteria upon sterilization of improperly cleaned or stored instruments
- exotoxins from patients with bacterial antigen loads from un- or undertreated blepharitis (isolated cases)
- endotoxins released from the cell walls of dead bacteria upon sterilization of improperly cleaned or stored instruments
| Grade | Interface | Topography | Vision |
|---|---|---|---|
| I | Partial | No change | Excellent |
| II | Complete | Irregular/shifts | Excellent |
| III | Complete | Irregular/shifts | Foggy |
| IV* | Complete | Irregular/shifts | Foggy |
* And inflamed eye

Figure 11-32 Grade 3 to 4 LIK. The circular inflammatory cellular material has formed along the rings of the broad-beam excimer ablation.
Prevention
- Because causes of LIK remain unproven, prevention is difficult.
- Clean and autoclave instruments and, in particular, the keratome between cases.
- At the end of the operating day, clean, sterilize, and dry the instruments to remove all moisture (prevents an environment for bacterial colonization and active division).
- Analyze all loaner units or traveling microkeratomes for cleanliness.
- Remove potential endotoxins using a proper cleaning regimen (e.g., an absolute ethanol soak).
- Gently clean the packaged microkeratome blade before use to remove any surface debris that may stimulate inflammation.
- Immediately use topical steroid drops for the first few postoperative days to suppress any inflammation early.
Management
- Ensure sterility of cornea (no epithelial defects).
- Early identification of LIK allows the prompt initiation of topical steroid treatment, which may rapidly resolve the condition.
- More severe cases may take 4 to 8 weeks to resolve.
- Start topical steroids every hour and then slowly taper over several weeks.
- Treat severe cases with interface irrigation (reported as successful by some surgeons).
- Antibiotics have no obvious role.
INFECTION Infections or corneal ulcers are extremely uncommon after LASIK with an incidence of less than 1/5000 cases. Because the corneal epithelium protects against infection, the risk of infection is minimal once the epithelium is completely healed. The short time of exposure of the stroma and the lack of epithelial disruption minimize this risk. Infections begin as infiltrates in the area of an epithelial defect and, if left: untreated, may progress into a typical corneal ulceration with infiltration, ocular inflammation, and pain.
Prevention
- Follow any patient with a postoperative epithelial defect daily to ensure that no infection occurs until the defect has healed.
- Use prophylactic antibiotics.
- Sterilize the microkeratome.
- Ensure good lid hygiene.
- Use antiseptic eyewash preoperatively.
- Wear talc-free gloves.
Management
- Assume that any corneal infiltrate associated with an epithelial defect after LASIK is infective and treat it immediately and aggressively.
- Perform corneal cultures (utility at this early stage of infection is controversial).
- Stop administering nonsteroidal medications and topical steroid drops.
- Instill topical fluoroquinolone every hour until improvement is noted.
- Lubricate the eye.
- Follow up with patient daily.
- If not resolved, switch to fortified topical antibiotics.
LASIK FLAP STRIAE Normally the striae are oriented horizontally with a nasal hinge and vertically with the superior hinge. Most flap striae occur within the first postoperative hour. Flap striae become more difficult to remove as the length of the postoperative course increases, and just 1 week postoperatively flap striae begin to become embedded in the corneal flap tissue (Figs. 11-33 and Fig. 11-34). Striae may be caused by
- misalignment of the corneal flap after flap replacement
- movement of the corneal flap during the first postoperative day
- the “tenting effect” of the corneal flap over the ablated stromal bed

Prevention
- Reposition the flap with minimal manipulation once it has been replaced into the correct position.
- Instruct patients to avoid rubbing or squeezing the eye postoperatively.
- Instruct patients to wear eye protection 24 hours a day for the first week to prevent any eye trauma while the flaps heal.
Management
- Identify flap striae on the first postoperative day (imperative) because striae become more difficult to remove as the length of the postoperative course increases.
- Retroilluminate the fixation light and aiming beam through the dilated pupil to accurately localize the flap striae and identify microstriae in cases of unexplained reduction of BCVA.
- Treat flap striae that extend through the visual axis or induce regular or irregular astigmatism.
- Administer phenylephrine 2.5% (allows intraoperative retroillumination).
- Mark the flap edge while viewing under the slit lamp.
- Make no flap alignment markings.
- Reflect back the flap.
- Hydrate the stromal surface of the flap with BSS for 30 sec.
- Replace the flap in the stromal bed and float it into position.
- Leave the flap for 5 min to attach the stromal bed and dry the epithelial surface.
- Mark the flap edge while viewing under the slit lamp.
- Use the side of blunt forceps or a dry Murocel sponge to stretch the flap perpendicular to the striae.
Figure 11-34 Severe striae associated with residual interface haze after LIK 3 weeks after LASIK.
DISLODGED FLAP Flap dislocation occurs in only 1/500 to 1/1000 of LASIK patients, usually because of some type of eye trauma or vigorous eyelid squeeze during the first 12 hr postoperatively. Vision becomes blurred and the eye becomes painful with an acute foreign-body sensation similar to the pain of a corneal abrasion. The incidence of epithelial ingrowth increases with both displacement and free caps.
Prevention
- Check the stability of the flap by ensuring that it is secure at the conclusion of the procedure by using the striae and blink tests (see p. 119).
- Wait 1 to 3 min after properly aligning the corneal flap and avoid excessive interface irrigation so that a strong seal may form.
- Advise patients to not rub or squeeze the eye.
- Provide eye protection for both day and night-time use.
Management
- Until flap replacement, lubricate the eye every 30 min with sterile preservative-free artificial tears to hydrate the flap and improve the discomfort.
- Patients usually keep the eye closed because of discomfort, or you may tape the eye shut until treated.
- Replace the corneal flap as soon as possible to avoid infection, reduce pain, and avoid permanent striae and damage to the flap (same procedure as for treating flap striae).
INTERFACE DEBRIS Interface debris often is present to some extent in most eyes following LASIK. Visual outcome is generally not affected and removal is unnecessary if the debris is inert. LASIK interface inflammation, however, does affect the visual outcome and should be differentiated from focal, noninflammatory interface debris. Following are examples of debris.
- lint
- red blood cells
- meibomian gland secretions
- metallic debris from blade
- dust
- rust particles from instruments
Prevention
- Interface irrigation during primary LASIK is the most effective method for reducing and potentially eliminating interface debris (removes > 90% of the minute dust particles that are invisible under the laser microscope but visible postoperatively by slit lamp).
- Several other preventive measures help to avoid interface debris.
- preoperative lid hygiene
- washing the fornices
- draping the lids
- air filters in surgical suite
- cleaning of all instruments between use to remove rust
- preoperative lid hygiene
Management
- If interface inflammation is suspected, follow the patient closely and begin administration of prophylactic topical steroids.
- Remove an interface contaminant that affects vision.
- Remove a large strand of lint that extends beyond the edge of the flap by pulling on it laterally with forceps.
- Remove debris that is completely under the flap using interface irrigation and flap repositioning (as in primary LASIK).
EPITHELIAL INGROWTH Reports indicate that 1.7% of eyes that undergo LASIK develop significant epithelial ingrowth that requires removal. However, refinements in the technique that delicately preserve the corneal epithelium have reduced this incidence to less than 1%. Epithelial ingrowth can occur in a number of patterns including lines, speckles, nest or pearls, strands, or sheets. Significant and persistent epithelial ingrowth often results in peripheral flap edge melt. Interface epithelial ingrowth may originate at three potential sites.
- stem cells peripheral to keratectomy edge (most common)
- isolated nest within the interface with no direct connection to the periphery (infrequent)
- passage through a defect in Bowman’s membrane and flap stroma (rare; caused by trauma to these structures with direct communication of surface epithelium to the interface
Risk Factors
- preoperative risk factors
- °ABMD
- a history of recurrent corneal erosions
- advanced age
- a history of ingrowth in the other eye
- °ABMD
- postoperative risk factors
- epithelial defects
- flap edema
- inflammation
- repeat LASIK
- flap slippage
- epithelial defects
Prevention
- Eliminate epithelial defects with LASIK (see Epithelial Defects section).
Management
- Identify the epithelial ingrowth by using one of several tests (Table 11-4).
- Consult Machat’s practical grading system for epithelial ingrowth to guide the course of management (Table 11-5 and Fig. 11-35 to Fig. 11-37).
- Indications for treatment include the following.
- greater than 2 mm of ingrowth from the flap edge
- documented progression
- associated flap melting
- a disturbance of BCVA attributable to the ingrowth
- greater than 2 mm of ingrowth from the flap edge
- Mark the edge of the corneal flap using the slit lamp.
- Mark peripheral cornea alignment.
- Slowly dissect free the flap at its temporal margin.
- Gently fold the flap over its nasal hinge.
- Remove the epithelium from underneath the flap by peeling and scraping (use a dry Murocel sponge or blunt instrument).
- Remove the epithelium from the stromal side of the Gently push back any epithelium hanging in the peripheral stromal bed.
- Replace the flap as for primary LASIK.
- Thoroughly irrigate underneath the cap to eliminate residual epithelial cells.
Figure 11-35 Grade 1 epithelial ingrowth.
| Test | Finding |
|---|---|
| Tangential slit-lamp illumination | White to gray material under flap |
| Fluorescein staining | Pooling at the flap edge |
| Corneal topography | Surface irregularities |
| Retroillumination | Margins of sheets of ingrowth |
Figure 11-36 Grade 2 epithelial ingrowth.
Figure 11-37 Grade 3 epithelial ingrowth.
ERRORS IN REFRACTIVE OUTCOME Patients are disappointed if any significant refractive error remains after LASIK because they still depend on refractive correction (Table 11.6). Even a −12.00 D myopic will return for a −0.50 D enhancement, despite remarkable improvement in uncorrected vision. Although we are able to accurately program excimer laser ablation and perfect keratectomy techniques, the healing response of the cornea is the unknown variable with LASIK. Some patients may regress up to 3.0 D whereas others do not regress at all. Younger patients (<25 years) tend to regress and experience undercorrections whereas older patients (>45 years) regress less and experience overcorrections.
| Grade | Description | Treatment | |
|---|---|---|---|
| 1 | Thin ingrowth, 1-2 cells thick, limited to≤2 mm of flap edge, transparent, difficult to detect, well delineated white line along advancing edge, no associated flap changes, nonprogressive | No retreatment required | |
| 2 | Thicker ingrowth, discreet cells evident within nest, ≥2 mm from flap edge, individual cells translucent, easily seen with slit lamp, no demarcation line along nest, corneal flap edge rolled or gray, no flap edge melting or erosion, usually progressive | Requires nonurgent treatment within 2-3 weeks | |
| 3 | Pronounced ingrowth, several cells thick,>2 mm from flap edge, ingrowth areas opaque, obvious with slit lamp, white geographic areas of necrotic epithelial cells with no demarcation line, corneal flap margins rolled with thickened whitish-gray appearance, progression results in large areas of flap melting from collagenase release from the necrotic epithelium, confluent haze develops peripheral to the flap edge as flap pulls away leaving exposed stromal bed in contact with surface epithelium | Urgent treatment required with close follow-up Recurrences are more common because of the altered flap edges |
Prevention
- Ensure the accuracy and the stability of the preoperative refraction.
- Use a consistent LASIK technique with controlled stromal hydration and drying.
- Consult nomograms developed for LASIK that account for the degree of correction and age of the patient to minimize errors in the refractive predictability (Table 11-7).
- Most myopia nomograms err toward undercorrection because myopia is generally less difficult to treat. 0 Overcorrect hyperopes by 10 to 20% because they tend to regress to emmetropia over 1 to 3 months.
- Carefully evaluate the technique that you choose, the geographic location of the laser center, the staffs attitude, and results to determine which nomogram is best for you.
- Most myopia nomograms err toward undercorrection because myopia is generally less difficult to treat. 0 Overcorrect hyperopes by 10 to 20% because they tend to regress to emmetropia over 1 to 3 months.
Management
- A contact lens may manage any refraction as early as 1 week after LASIK, so that patients may return to full activities almost immediately.
- Topical steroids have little effect on refractive results.
- After achieving refractive stability, you may perform an enhancement procedure.
- The greater the primary LASIK correction, the more postoperative time that is required to achieve full refractive stability.
- Do not perform PRK over a LASIK flap because PRK may induce corneal haze.
- The greater the primary LASIK correction, the more postoperative time that is required to achieve full refractive stability.
| Error | Comment | Enhancement |
|---|---|---|
| Hyperopia | Normal cornea Thin cornea | Hyperopic LASIK at 4 months Laser thermokeratoplasty at 6 months |
| Myopia | 1-3 D preoperatively 3-6 D preoperatively 6 D preoperatively | Myopic LASIK at 1 month Myopic LASIK at 2 months Myopic LASIK at 3-4 months |
| Regression | Wait for stability | Myopic LASIK |
| Astigmatism | Wait for stability | LASIK at 3-4 months |
CENTRAL ISLANDS Several situations lead to the formation of central islands.
- central accumulation of fluid
- inhomogeneous beam
- vortex plume with central shielding of successive pulses when using a broad-beam excimer laser
The presentation of central islands includes the following.
- loss of BCVA and UCVA
- irregular astigmatism
- monocular diplopia
- undercorrection
Although most central islands resolve by 1 month with no treatment or PRK.
Prevention
- Central island facto (CIF) software has been incorporated into the VISX laser to allow extra treatment to the central cornea to compensate for the central island effect of the broad beam laser.
- Scanning excimer lasers eliminate the risk of central islands.
- Fluid does not accumulate centrally.
- The vortex plume is not stationary.
- Homogeneity of the beam with scanning lasers is not critical because of the smoothing or polishing effect of overlapping spots or slits.
- Fluid does not accumulate centrally.
- Remove any central accumulation of fluid by wiping the stromal bed during LASIK (alters overall stromal hydration and therefore affects the final refractive outcome).
Management
- Identify and monitor central islands with topography until they are stable in size and severity (Fig. 11-38).
- Do not use refraction as an indicator of stability because it often varies considerably with each refraction.
- Treat a central island only if it causes subjective visual complaints or loss of BCVA.
- Topographic central island without patient complaints should not be treated just because the practitioner thinks it should be treated; treat the patient.
- Measure the size and height of the island with corneal topography (use the Munnerlyn formula to calculate the height of the island).
- height in microns = diameter2 X diopter height/3
- Then correct the exact number of microns and diameter size of the island using the phototherapeutic keratectomy (PTK) mode on the VISX (Star or Smoothscan) or the Chiron 116 excimer laser.
- Alternatively, treat the refractive myopia in the PRK mode of the VISX laser but only for the first 50% of the ablation.
- The Chiron 217 does not treat the central island well because the blending effect of the scanning laser does not allow the beam to be focused into the central area alone.
- Use a conservative approach because overtreatment results in a central divot, which creates irregular astigmatism and abrupt topographic changes over the pupillary axis (leads to multiple image formation or ghosting, which is difficult to correct surgically but may be treated with a rigid contact lens).
- Do not use refraction as an indicator of stability because it often varies considerably with each refraction.
| Patient Age | |||
|---|---|---|---|
| Amount of Myopia | <25 years | 25-45 years | >45 years |
| <2.0 D | 100% | 100% | 100% |
| >2.0 D | 90% | 86% | 84% |
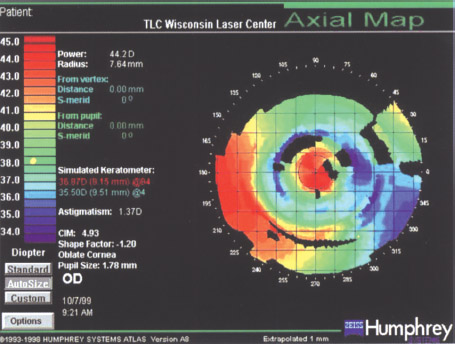
Figure 11-38 Corneal topography demonstrating a central island.
IRREGULAR ASTIGMATISM All patients have some degree of postoperative irregular astigmatism immediately, which gradually resolves a few weeks after the procedure. Persistent irregular astigmatism is now relatively uncommon but results in several undesired outcomes.
- reduced UCVA and BCVA
- visual distortion
- ghosting
- monocular diplopia
Prevention
- Proper surgical technique minimizes flap-related complications, such as striae.
- Check the homogeneity of the excimer laser beam regularly to ensure that the beam is smooth and symmetrical (irregular patterns are amplified during large corrections).
- Monitor hydration of the stromal bed (uneven wetting of the stromal bed can result in an irregular ablation pattern).
Management
- Postoperative topography, photokeratoscopy, manual keratometry, or even retinoscopy often uncovers some degree of irregularity that is related to some variation in corneal healing.
- Slit-lamp examination may reveal flap striae, LASIK interface inflammation, or corneal scarring which may result in irregular topographic patterns.
- Treatment of the flap striae and LIK (as described previously) dramatically improves both the symptoms and the topographic pattern.
- Corneal topography may demonstrate other irregularities of an otherwise normal cornea (e.g., central islands).
- Other irregular patterns are more difficult to treat because they require a customized ablation pattern.
- Topography-linked scanning excimer lasers offer the most promise for the treatment of irregular patterns.
- If all else fails, RGP contact lenses, if tolerated, are usually very helpful in reducing (if not eliminating) unwanted visual symptoms.
NIGHT GLARE Night glare occurs when the pupil dilates greater than the OZ of the refractive correction (Fig. 11-39). Preoperative and postoperative night glare are more common in high myopes. Patients experience halos, starbursts, and reduced quality of vision. Although manageable in most patients, night glare may disable others.
Prevention
- Screen patient preoperatively for pupil size.
- Counsel patients with large pupils (>6 mm) in dim illumination about the potential risk of postoperative night glare.
- Treat patients with large pupils with larger-diameter ablation zones (≤9 mm); however, these lasers ablations remove significantly greater amounts of stroma so stromal thickness is the critical data point for determining candidacy.
Management
- Fortunately, most symptoms of night glare abate within the first year after the operation.
- Refinements in ablation profiles have resulted in significant reduction in the number of complaints of night glare.
- Perform LASIK on the other eye.
- Eliminate monovision.
- Prescribe night-driving glasses (1.00 D).
- Prescribe polarized lenses.
- Use spectacle lens filters (shooter’s yellow, lambda 540).
- Instruct patient to use a night light in the car while night driving.
- Initiate miotic therapy (pilocarpine 1/8%) to constrict pupil when night driving
- Perform LASIK on the other eye.
- Surgical.
- Retreat the eye by using a larger OZ and ablation zone.
- Perform topography-assisted LASIK to same eye.
- Retreat the eye by using a larger OZ and ablation zone.
DECENTERED ABLATIONS Decentration of the ablation results in a residual refractive error (irregular astigmatism), which is associated with visual distortions and ghosting, particularly at night, and the patient may lose some BCVA. The patient’s concerns are often more significant than expected for such a small refractive error. Decentered ablations have many causes.
- pharmacological pupillary dilation
- pharmacological constriction
- large angle kappa
- poor patient fixation
- wide flap hinge encroaching on ablation zone
- eccentric fixation
- treatment beam not coaxial with patient fixation beam (validate during instrument setup)
Prevention
- Always center excimer ablations on the pupil to minimize decentrations.
- Avoid pharmacological alteration several days before performing LASIK.
- To ensure centration on the pupil leave the suction ring on the eye but without active suction to control the position of the ablation completely.
- Patients often have difficulty fixating on the fixation beam once the flap has been cut because the stroma does not provide a clear interface.
Figure 11–40 Decentered hyperopic ablation 4 months after hyperopic LASIK for a +5.0 D correction.
Management
- Detect decentration (obvious with postoperative topography; Fig. 11-40).
- Because the decentered ablation creates an irregular ablation pattern, treatment is difficult with a broad-beam laser.
- The refractive error is treatable and the flap is replaceable, these treatment options do not treat the edge glare effect from the sort edge of the ablation zone.
- A second ablation in the opposite direction of the original decentration has also been suggested but may result in a more irregular pattern.
- Topography-assisted LASIK (TA-LASIK) holds the most promise for decentered ablation because it treats the untreated area of the ablation zone.
- Because the decentered ablation creates an irregular ablation pattern, treatment is difficult with a broad-beam laser.
LASER IN SITU KERATOMILEUSIS AS AN ENHANCEMENT PROCEDURE
Indications and Inclusion Criteria
- at least 1.00 D of myopia or hyperopia
- at least 1.00 D of astigmatism
- UCVA of 20/40 or worse
Risks
- overcorrection
- epithelial ingrowth
- flap striae
- infection
- pain
Preoperative Evaluation
- Ensure stable refraction.
- Ensure adequate corneal thickness using pachymetry.
- Perform regular topography.
Methods (Fig. 11-41)
- Mark flap edge at slit lamp.
- Place alignment marks on cornea.
- Lift flap before 6 months postoperatively.
- Recut flap at a deeper depth after 6 months.
- Peel back flap edge to minimize epithelial disruption.
- Perform excimer enhancement ablation.
- Refloat flap into position.
- Irrigate the stroma interface.
- To ensure centration on the pupil, leave that suction ring on the eye with the suction off to control the position of the ablation completely.
- Check alignment marks and gutter for alignment.
- Wait 1 to 5 min for adhesion to occur.
- Perform a blink and/or striae test.
Postoperative Management
- Monitor for ingrowth.
- Check refractive outcome.
Laser In Situ Keratomileusis after Radial Keratotomy
Indications and Inclusion Criteria
- myopia or hyperopia post radial keratotomy (RK)
- RK performed at least 1 year ago
- stable refraction
- regular astigmatism on topography
Risks
- unstable postoperative refraction
- decreased postoperative refractive predictability
- flap fragmentation
- epithelial ingrowth
- persistent starburst and night glare
- persistent diurnal variation
- potential increase in corneal anatomical instability
Preoperative Evaluation
- Ensure refractive stability.
- Measure early morning refraction.
- Make no more than eight radial incisions.
- The OZ should be at least 3.0 mm.
- Allow radial incisions to heal well.
- Verify no epithelial cysts.
- Ensure no reduction in BCVA from RK.
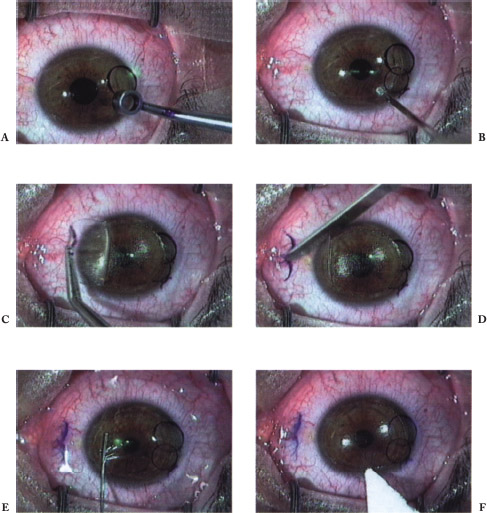
Figure 11-41 Technique of LASIK enhancement. (A) Flap edge is marked with alignment marks. (B) Flap edge is lifted. (C) Flap is grasped with nontoothed forceps and folded back. (D) Residual epithelial cells are scraped from the stromal surface of the flap and laser is then applied. (E) Flap replaced and the interface is irrigated. (F) Peripheral edge of the flap is dried and inspected to ensure good flap alignment.
Methods (Fig. 11-42)
- Use a 200-μm depth plate with ACS.
- Target slight myopia.
- Perform monocular treatment.
- Use extreme care with flap manipulation.
- Align flap and radial incisions carefully.
Postoperative Management
- Expect greater initial refractive fluctuations than with primary LASIK.
- Monitor patient for epithelial ingrowth.
- Do not lift the flap.
- Recut flap at 6 months for enhancements.
Laser In Situ Keratomileusis after Photorefractive Keratectomy
Indications and Inclusion Criteria
- myopia or hyperopia after PRK
- no corneal haze
- corneal thickness at least 450 μm
Risks
- persistence of superficial corneal haze
- epithelial defects
- epithelial ingrowth
- reduction in corneal anatomic integrity
Preoperative Evaluation
- Establish refractive stability.
- Ensure adequate corneal thickness.
- Ensure no corneal haze.
- Ensure no history of recurrent erosion after PRK.
- Confirm well-centered ablation with topography.
- Ensure no loss of BCVA from PRK.
Methods
- Use a 200-μm depth plate with ACS.
- Administer minimal topical anesthetic.
- Protect the epithelium with lubrication.
Postoperative Management
- Monitor patient for epithelial ingrowth.
- Refractive stability may take a few weeks to develop.
Laser In Situ Keratomileusis after Penetrating Keratoplasty
Indications and Inclusion Criteria
- residual myopia and astigmatism after penetrating keratoplasty (PK)
- sutures removed at least 1 year ago
- stable refraction
- regular astigmatism on topography
- adequate corneal thickness
Risks
- unstable postoperative refraction
- decreased predictability of postoperative refractive
- epithelial ingrowth
- dehiscence along graft edge
- induction of graft rejection
- greater incidence of enhancement
Preoperative Evaluation
Methods
- Wait 12 months after PK sutures are removed.
- Center suction ring on graft.
- Minimize suction time.
- Wait 2 weeks after PK before performing ablation.
Postoperative Management
- Prescribe topical steroids for 1 to 2 weeks to prevent rejection.
- Monitor for ingrowth.
- Wait 4 months before performing enhancement.
- Lift flap for enhancement.
Laser In Situ Keratomileusis after Automated Lamellar Keratoplasty
Indications and Inclusion Criteria
- residual myopia and astigmatism after ALK
- removal of sutures at least 1 year ago
- stable refraction
- regular astigmatism on topography
- adequate corneal thickness
Risks
- unstable postoperative refraction
- decreased predictability of postoperative refractive status
- epithelial ingrowth
- greater incidence of enhancement
- reduction in corneal anatomic integrity
- induction of irregular astigmatism
- loss of BCVA
Preoperative Evaluation
- Confirm refractive stability.
- Confirm no irregular astigmatism on topography.
- Ensure no loss of BCVA from ALK.
Methods
- Position the cut temporal to previous keratectomy.
- Use a 200-μm cut.
Postoperative Management
- Expect greater refractive fluctuations initially.
- Watch for ingrowth.
- Wait 4 months before performing enhancements.
- Lift flap for enhancement.
Laser In Situ Keratomileusis after Insertion of a Phakic Intraocular Lens
Indications and Inclusion Criteria
- residual refractive error after phakic IOL insertion
- posterior-chamber phakic IOL implantation
- refractive stability
Exclusion Criteria
- age less than 50 years
- extreme refractive errors
- thin corneas
Risks
- endothelial damage with anterior chamber IOL (ACIOL)
- dislocation of IOL
- crystalline lens or IOL in contact with posterior chamber IOL (PCIOL)
Preoperative Evaluation
- Ensure refractive stability.
- Perform regular topography.
- Wait at least 1 month after phakic IOL insertion before using a refractive laser.
- Keratectomy should be performed prior to ACIOL insertion, but refractive laser correction is still done 1 month later by lifting the flap.
- Rule out cataracts.
Methods (Fig. 11-43)
- Minimize suction time.
- Treat residual sphere and cylinder.
Postoperative Management
- Check IOL centration.
- Enhance as in primary LASIK.
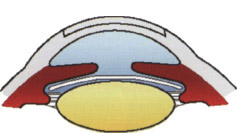
Figure 11-43 LASIK after insertion of a posterior chamber phakic IOL.
Laser In Situ Keratomileusis after Cataract Surgery
Indications and Inclusion Criteria
- refractive error after cataract surgery
- normal BCVA
- stable refraction
Risks
- dislocation of IOL
- additional loss of endothelial cells
- thin flap (because of poor suction)
Preoperative Evaluation
- Ensure refractive stability.
- Perform regular topography.
- Wait at least 1 to 3 months after cataract surgery.
Methods (Fig. 11-44)
- Ensure good suction.
- Use a 200-μm depth plate with ACS.
- Treat residual sphere and cylinder.
Postoperative Patient Management
- Check IOL centration.
- Enhance as in primary LASIK.
Topography-Assisted Laser In Situ Keratomileusis
Indications and Inclusion Criteria
- irregular astigmatism with primary LASIK
- decentered ablation zone after LASIK
- small OZ after LASIK
Risks
- reduced corneal thickness
- increased irregular astigmatism
- misalignment of centration or axis of custom ablation
- unpredictable results with central islands
Preoperative Evaluation
- Perform pachymetry.
- Estimate central K reading.
- Perform multiple high-quality topography.
- Send data to Technolas in Germany.
Methods
- Use a Hansatome flap to obtain the full effect of custom ablation.
- Ensure centration (critical).
- Ensure axis alignment (critical).
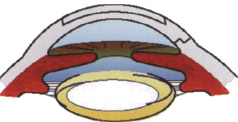
Figure 11-44 LASIK after cataract surgery or clear lens extraction.
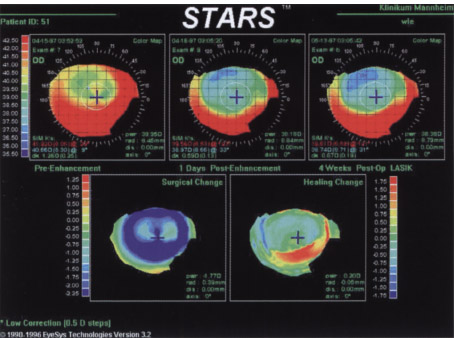
Figure 11-45 Topographic changes following treatment of a decentered ablation using topography assisted LASIK. (Courtesy of Micheal Knorz, M.D.).
Postoperative Management
- Expect longer visual rehabilitation compared with standard LASIK.
- Evaluate with topography (Fig. 11-45).
Suggested Readings
Doane JF, Koppes A, Slade SG. A comprehensive approach to LASIK. Ophthalmic Nun Technol. 1996;15:144-147.
Machat JJ, Slade SG, Probst LE, eds. The Art of Lasik. Thorofare, NJ: Slack, Inc.; 1999.
Pallikaris IG, Siganos DS, eds. LASIK. Thorofare, NJ: Slack, Inc.; 1997.
Slade SG, Doane JF. LASIK: Laser in situ keratomileusis. In: Yanoff M, Duker JS, eds. Ophthalmology. London: Mosby; 1998:1-8.
Slade SG, Machat J, Doane, JF. Laser in situ keratomileusis: cornea. In: Kaufman HE, Barron BA, McDonald MB. The Cornea. 2nd ed. Newton, MA: Butterworth-Heinemann; 1998:1015-1036.
Wu H, Steinert R, Slade S, Thompson V, eds. Refractive Surgery. New York: Thieme; 1999.
< div class='tao-gold-member'>



