13 ![]()
Definition
How Is Traumatic Glaucoma Defined?
Traumatic glaucoma is the occurrence of elevated intraocular pressure (IOP) secondary to ocular trauma. However, not every posttraumatic IOP elevation is necessarily due to trauma; for instance, the eye may have harbored primary glaucoma prior to the trauma. Furthermore, traumatic glaucoma may be masked by coincidental pathology that lowers the IOP. Table 13–1 shows how the IOP level may be interpreted following trauma.
Table 13–2 lists the different types of trauma that may be sustained by the eye. Glaucoma complicating intraocular surgery is discussed in Chapter 12. Head injury may lead to a carotid-cavernous fistula, which may give rise to glaucoma by raising episcleral venous pressure; this is discussed in Chapter 6. Otherwise, all other forms of traumatic glaucoma are discussed in detail in this chapter.
High IOP |
Preexisting primary glaucoma* |
Preexisting primary glaucoma + traumatic glaucoma* |
Pure traumatic glaucoma |
Low IOP |
Missed rupture globe (e.g., posterior scleral rupture) |
Cyclodialysis |
Ciliary shutdown |
Choroidal effusion |
Retinal detachment |
Normal IOP |
No ocular damage leading to glaucoma |
Combination of high and low IOP |
* The fellow eye may show manifestations of primary glaucoma. |
| Mechanical injury |
Direct |
Nonpenetrating (blunt) trauma |
Penetrating trauma (± intraocular foreign body) |
Surgical trauma |
Cataract surgey |
Glaucoma surgery (incisional and laser) |
Penetrating keratoplasty |
Scleral buckling |
Pars plana vitrectomy |
Nd:YAG laser surgery |
Indirect |
Head injury |
| Chemical injury |
Alkali burns |
Acid burns |
| Radiation injury |
| Electrical injury |
| Thermal injury |
Nd:YAG, neodymium:yttrium-aluminum-garnet. |
What Are the Mechanisms of Traumatic Glaucoma?
Much like primary glaucoma, traumatic glaucoma may be of the open-angle or closed-angle type. In open-angle varieties, the obstruction to aqueous outflow may be pretrabecular (e.g., epithelial down-growth), trabecular (e.g., glaucoma complicating hyphema, and ghost cell glaucoma), or posttrabecular (e.g., elevated episcleral venous pressure secondary to a carotid-cavernous fistula). Angle closure results from apposition or adherence of peripheral iris to the trabecular meshwork or peripheral cornea. In the anterior (“pull”) mechanism, an abnormal tissue in the angle contracts and pulls the iris into the angle (e.g., a fibrovascular membrane associated with neovascular glaucoma). Posterior (“push”) mechanisms include pupillary block (e.g., by a swollen cataractous lens) and forward movement of the iris-lens diaphragm (secondary to ciliochoroidal effusion or ciliary block).
How Long After Trauma Does the IOP Rise Occur?
Depending on pathogenesis, the onset of IOP elevation following trauma is variable. The IOP may rise in the first few hours following trauma, as in hyphema. Lens particle glaucoma, for example, will only appear a few days after penetrating trauma. Ghost cell glaucoma requires at least 2 weeks to develop. Angle recession glaucoma typically develops years after the traumatic incident. Therefore, a patient presenting with traumatic glaucoma may have even forgotten the traumatic incident that caused the IOP elevation. The temporal aspect of the different types of traumatic glaucoma will be discussed under each category.
In this chapter, traumatic glaucoma will be discussed under the following categories: nonpenetrating trauma, penetrating trauma, chemical injury, radiation injury, electrical injury, and thermal injury. Figure 13–1 shows the general lines of management of traumatic glaucoma.
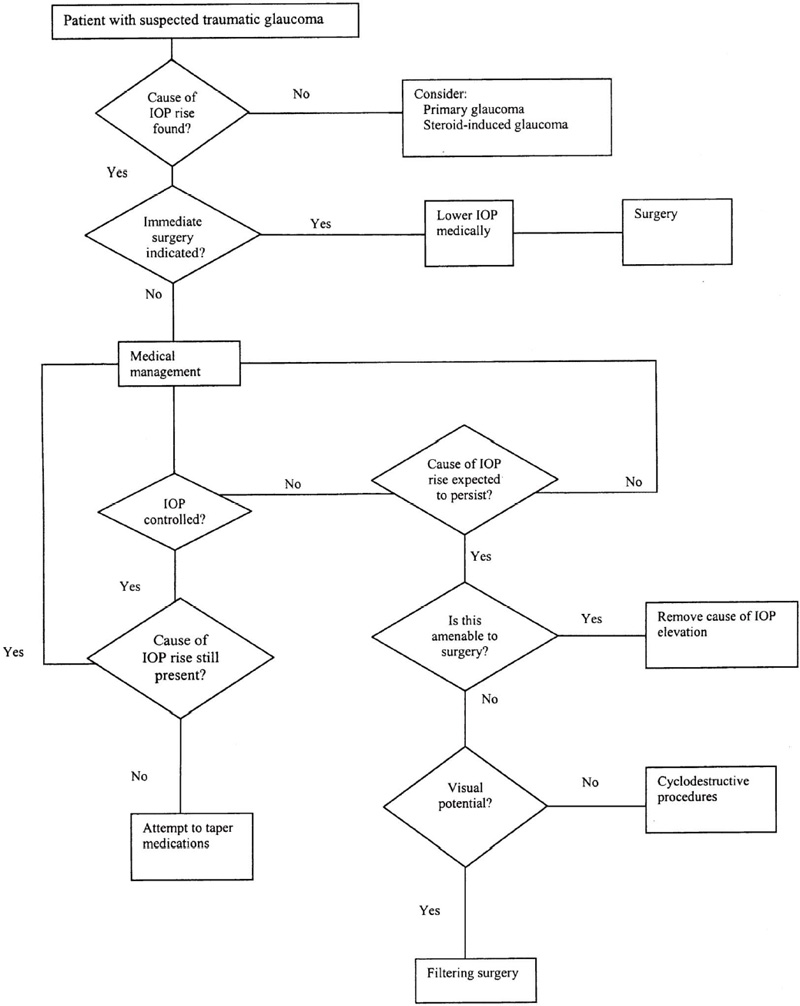
Figure 13–1. General lines of management of traumatic glaucoma.
GLAUCOMA COMPLICATING NONPENETRATING TRAUMA
Definition
How Is the Problem Defined?
Nonpenetrating ocular trauma is injury to the eye resulting from impact of a blunt injurious agent that does not penetrate the globe. Whether or not the trauma is penetrating depends on the size, shape, weight, composition, speed, and direction of the injuring object, as well as the impact, location, and the status of the eye and ocular adnexa before the injury. Various types of glaucoma may complicate nonpenetrating ocular trauma.
Epidemiology and Importance
What Type of Patient Is More Liable to Sustain Direct Ocular Trauma?
Most patients sustaining direct ocular trauma—whether penetrating or blunt—are young, typically less than 30 years of age.1–7 The setting of ocular trauma is related to age, play being the most common in children, sports and assaults in young adults, and work and domestic accidents in older adults.8–10 Males are more commonly victims of ocular trauma than females.2,7,11,12 Patients from lower socioeconomic groups experience more severe and frequent ocular trauma.12
Diagnosis and Differential Diagnosis
What Is the Differential Diagnosis of Glaucoma Secondary to Nonpenetrating Trauma?
Table 13–3 lists the various types of glaucoma complicating nonpenetrating trauma. These may occur singly or in combination. For example, hyphema may be associated with lens dislocation and trabecular injury. Figure 13–2 shows the differential diagnosis of elevated IOP in the presence of recent blunt trauma, and Figure 13–3 after an old traumatic incident.
Glaucoma secondary to hyphema |
Hemolytic glaucoma |
Hemosiderotic glaucoma |
Ghost cell glaucoma |
Angle recession glaucoma |
Glaucoma secondary to trabecular injury |
Glaucoma secondary to traumatic cataract |
Glaucoma secondary to lens dislocation |
Glaucoma secondary to forward movement of the iris-lens diaphragm |
Glaucoma secondary to posttraumatic uveitis |
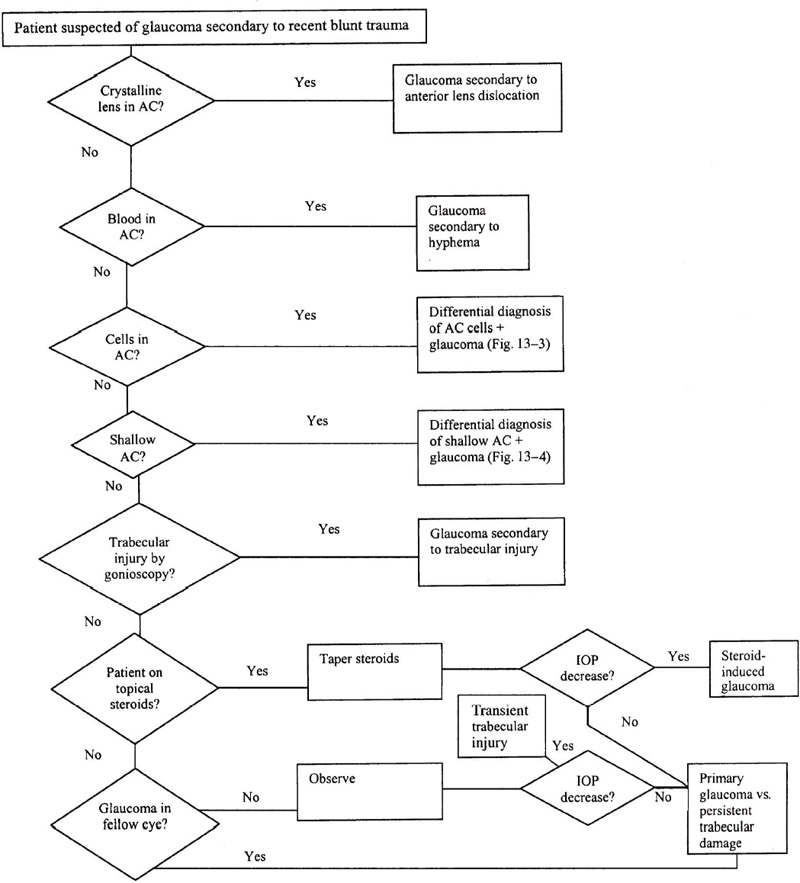
Figure 13–2. High IOP in the presence of recent blunt trauma.
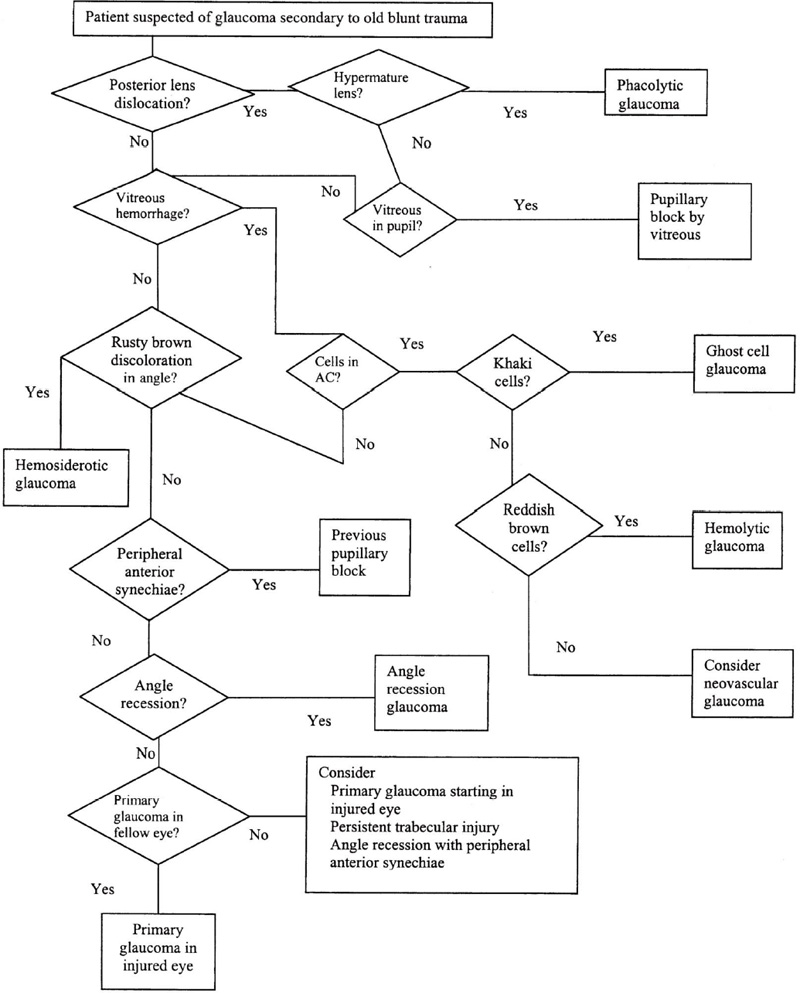
Figure 13–3. IOP elevation in the presence of old blunt trauma.
Treatment and Management
How Is Glaucoma Secondary To Nonpenetrating Trauma Managed?
In most cases, initial management of glaucoma is lowering of IOP through aqueous suppressants, such as beta-lockers, α2-agonists, and carbonic anhydrase inhibitors (CAIs), and, if necessary, hyperosmotic agents such as mannitol. Definitive management depends on the cause, as is discussed below.
In the following section, each of the different types of glaucoma complicating nonpenetrating ocular trauma (listed in Table 13–3) is discussed in detail.
GLAUCOMA COMPLICATING HYPHEMA
Definition
How Is Glaucoma Complicating Hyphema Defined?
Hyphema is characterized by red blood cells in the anterior chamber and is frequently associated with glaucoma. Traumatic hyphema occurs most often from a tear in the anterior surface of the ciliary body, with resultant disruption of the major arterial circle of the iris, arterial branches to the ciliary body, or veins coursing between the ciliary body and the episcleral venous plexus. In most cases, the blood clears within a few days by egress through the trabecular meshwork. If the hyphema persists, an additional problem, such as trabecular meshwork injury, uveitis, vitreous hemorrhage, or rebleeding, must be suspected.13
What Are the Mechanisms Underlying Glaucoma Complicating Hyphema?
There are several mechanisms by which hyphema may elevate the IOP. Most frequently, there is mechanical obstruction of the trabecular meshwork by erythrocytes and blood products. In cases with larger hyphemas, pupillary block by a blood clot may also contribute to the elevated IOP.14 Because fresh erythrocytes easily pass through the normal conventional aqueous outflow system, it is presumed that the IOP rises as a result of temporary impairment of trabecular meshwork function following blunt trauma. Even assuming normal outflow facility, the trabecular meshwork may be overwhelmed transiently by the numbers of red blood cells, combined with plasma, fibrin, and debris.13
Typically, IOP elevation is transient, subsequently falling to a mildly subnormal level for a few days.15 Persistent glaucoma is a rare complication. In a retrospective study of 314 patients with hyphema, Kearns16 reported a 1% incidence of persistent glaucoma.
Epidemiology and Importance
What are the Risk Factors for Glaucoma Complicating Hyphema?
Hyphema is a frequent sequela of nonpenetrating (and penetrating) trauma. The incidence varies in different reports, ranging from 6% in a study of pediatric ocular trauma12 to 55.2% in a survey of penetrating injuries caused by assault.3 Patients with traumatic hyphema are most often young males, with sports-related injuries and assaults accounting for the majority of cases associated with blunt trauma.16
The incidence of elevated IOP in traumatic hyphema has been found to correlate well with the size of the hemorrhage. Coles17 studied 235 cases of traumatic hyphema, and found elevated IOP in 13.5% of eyes with hyphema filling less than half of the anterior chamber, 27% with hyphema filling more than half of the anterior chamber, and 52% with total hyphema. Elevated IOP is also more commonly seen in eyes that rebleed. In a series of 113 cases, glaucoma developed in 33% of patients who rebled and in 100% of patients when rebleeding resulted in eight-ball hyphemas.18
Patients with sickle cell hemoglobinopathy may have IOP elevation disproportionate to the amount of the hyphema.19 Their erythrocytes have a tendency to sickle in aqueous humor, and the sickled cells may pass slowly through the trabecular meshwork. These patients are also in greater jeopardy from the elevated IOP because of their predisposition to central retinal artery occlusion.19,20
Diabetes mellitus has also been implicated with delayed clearance of erythrocytes from the anterior chamber, as erythrocytes from patients with proliferative diabetic retinopathy show decreased deformability and increased adherence.21
Diagnosis and Differential Diagnosis
How Is Hyphema Diagnosed?
The clinical diagnosis of hyphema is based on the finding of red blood cells in the anterior chamber. The amount varies from rare circulating cells in the aqueous to subtotal hyphema with a level, or even total hyphema that may darken to become a “black-ball” or “eight-ball” hyphema. The presence of uniformly bright red blood indicates a fresh hemorrhage, although this may darken with time. The presence of layering (i.e., a mixture of fresh and clotted blood) should alert the examiner to the possibility of rebleeding.13
Once hyphema is detected, it should not be immediately assumed that the trauma was blunt. Penetrating trauma, with or without an intraocular foreign body, may also cause hyphema. Therefore, the examiner should reascertain the nature of the injury from the patient, or the accompanying family members. The eyelids, conjunctiva, cornea, and sclera should be carefully examined with the slit lamp for the possibility of penetrating injury. If necessary, plain x-ray and computed tomography (CT) imaging may be performed to exclude intraocular foreign bodies. These imaging techniques are also useful for the exclusion of orbital fractures.
Other signs of blunt trauma should be sought. These include pupillary sphincter tears, iridodialysis, angle recession, cyclodialysis, trabecular dialysis, lens subluxation or dislocation, retinal dialysis and /or detachment, macular edema (commotio retinae), and choroidal rupture.22 Gonioscopy (to detect angle recession, cyclodialysis, or trabecular dialysis) should not be performed until 4 weeks after the traumatic incident, as the attendant pressure on the globe may reopen an occult rupture of the globe, or promote rebleeding by dislodging a blood clot from the injured vessel. Likewise, scleral indentation to detect peripheral retinal pathology should be deferred. If the hyphema is total, ultrasound examination may be useful to detect coincidental posterior segment pathology, such as vitreous hemorrhage, retinal detachment, and posterior lens dislocation. Where available, high-frequency ultrasound (ultrasound biomicroscopy) may detect anterior segment conditions masked by a total hyphema, such as lens subluxation or angle recession.23
With the slit lamp, a search is made for corneal blood staining. Pathologic studies of blood staining demonstrate erythrocyte breakdown products and hemosiderin in the keratocytes and corneal stroma.24 Initially, this will manifest as a subtle yellowish discoloration of the posterior corneal stroma. Although corneal blood staining requires a high IOP, it may occur in the absence of glaucoma if there is corneal endothelial damage. When corneal blood staining is detected, this in itself may be an indication for surgical evacuation of the hyphema.
The visual acuity should be correlated with the amount of hyphema and coincidental ocular pathology. The presence of profoundly reduced vision (no light perception or bare light perception) that is not explained by the amount of hyphema or posterior segment problems should alert the examiner to the possibility of traumatic optic neuropathy, which may require megadose steroid therapy or surgical decompression of the optic canal.25 Nevertheless, many patients with hyphema manifest afferent pupillary defects caused by the intraocular blood itself, rather than by the optic nerve injury.13
The IOP is measured by applanation tonometry or pneumatonometry. Ocular pressure by palpation is avoided in the acute period for reasons similar to gonioscopy and scleral indentation. Examination of the fellow eye is essential to provide a baseline IOP or to rule out the possibility of preexisting primary glaucoma in the injured eye.
If the patient is of African descent, a search should be made for sickle cell disease, including hemoglobin electrophoresis. If sickle cell disease is present, management will have to be more aggressive. Similarly, diabetes is also ruled out.
What Is the Differential Diagnosis of Hyphema with Glaucoma?
If the patient does not have a history of trauma, and there are no signs suggestive of trauma, other causes of hyphema should be considered, as any of them may be accompanied by glaucoma. These include neovascular glaucoma, herpetic iridocyclitis, retinoblastoma, uveal malignant melanoma, and juvenile xanthogranuloma.
Treatment and Management
How Is Glaucoma Complicating Hyphema Managed?
Management should be directed toward three main aims: encouraging resorption of hyphema, prevention of rebleeding, and treatment of elevated IOP.
To encourage hyphema resorption, activity should be restricted. For simple hyphema, outpatient management with limited activity and a shield may suffice.26,27 For severe cases and sickle cell patients, hospitalization with bed rest is mandatory.
Many drugs have been used to accelerate resorption of hyphema, including intravenous hyperosmotic agents (urea and mannitol), subconjunctival methyl-prednisolone,28 systemic acetazolamide, topical atropine and pilocarpine,29 and intracameral tissue plasminogen activator (TPA),30 but none has been shown to have a clinically significant benefit. Although TPA was found in a rabbit model to accelerate hyphema resorption, it also substantially increased rebleeding episodes.30
Prevention of rebleeding is achieved by inhibition of clot lysis. Two antifibrinolytic agents, aminocaproic acid31–33 and tranexamic acid,34 have been tried, with equivocal results. Aminocaproic acid often causes nausea, vomiting, systemic hypotension, and dizziness, and has not been universally accepted. Furthermore, both drugs may precipitate thrombotic episodes in predisposed patients, such as patients with coronary artery disease. Because of these considerations, antifibrinolytics are reserved for patients at high risk of complications related to rebleeding, such as those with sickle cell disease, and perhaps all black patients.13
Elevated IOP associated with hyphema usually responds favorably to topical aqueous suppressant therapy, such as beta-blockers and α2-agonists. CAIs may also be added when required. However, systemic acetazolamide is better avoided in sickle cell patients, as it increases ascorbate levels in the aqueous humor and produces systemic acidosis, both of which exacerbate erythrocyte sickling.19 Methazolamide may be safer as it causes less systemic acidosis than acetazolamide.
When elevated IOP cannot be controlled medically and threatens to damage the optic nerve head, or if the hyphema is associated with corneal blood staining, surgical intervention is indicated. The critical level of IOP that warrants intervention depends on the status of the optic nerve head and the patient’s general medical status. A healthy optic nerve may tolerate pressures of up to 40 or 50 mm Hg for a week or longer, whereas a glaucomatous disc may suffer further damage with substantially lower pressures within a shorter time period. Evaluation of the fellow eye may provide important information on preexisting glaucoma. Even the slightest IOP rise should be taken more seriously in sickle cell patients, as they are more prone to retinal artery occlusion.13
The optimal time for surgical intervention is controversial. Rebleeding is more frequent if intervention is instituted early. Furthermore, if intervention is delayed 3 to 5 days, many cases will resolve spontaneously. Four days has been suggested as the optimal time for surgical intervention with total hyphemas, as this allows optimal clot retraction without adherence to adjacent tissues.35
Various surgical approaches have been utilized successfully. The simplest of these is anterior chamber washout by irrigation through a paracentesis, with or without fibrinolytics.36,37 Cases with more extensive clotting may require clot aspiration with the aid of ultrasonic emulsification or vitrectomy instrumentation. 38,39 In such cases, complete clot removal is neither safe nor necessary. Repeated attempts to disengage the clot may result in iris, lens, or angle damage, or invite rebleeding. Alternatively, the clot may be expressed out of the anterior chamber through a corneoscleral incision with the aid of a viscoelastic agent.40,41 Trabeculectomy with gentle irrigation through a separate paracentesis track may allow almost total removal of the clot, with at least temporary IOP control.42 Although permanent filtration usually is not established, the trabeculectomy often affords subconjunctival filtration for a few weeks while trabecular meshwork function recovers.
HEMOLYTIC GLAUCOMA
Definition
What Is Meant by Hemolytic Glaucoma?
Hemolytic glaucoma is an open-angle glaucoma that occurs within days to weeks after a large intraocular hemorrhage.
What Is the Mechanism of IOP Elevation in Hemolytic Glaucoma?
The mechanism of IOP elevation is an obstruction of the trabecular meshwork by macrophages laden with pigment, erythrocytes, and debris.43,44 One ultrastructural study demonstrated that the condition is also associated with degenerative changes in trabecular endothelial cells that had phagocytosed blood.45 Most commonly, the condition is self-limited but may persist, requiring management as discussed below.
Epidemiology and Importance
What Are the Risk Factors for Hemolytic Glaucoma?
The main risk factor for hemolytic glaucoma is intraocular hemorrhage, whether hyphema or vitreous hemorrhage.
Diagnosis and Differential Diagnosis
How Is Hemolytic Glaucoma Diagnosed?
The condition is diagnosed with the slit lamp by the presence of reddish-brown cells in the aqueous humor. There should be associated intraocular hemorrhage, in the form of hyphema and/or vitreous hemorrhage.
If the trauma is not recent, gonioscopy may be performed. Gonioscopy reveals an open angle without neovascularization. The trabecular meshwork may be covered with reddish-brown pigment, especially inferiorly.44 The condition may also be confirmed by cytologic examination of the aqueous, which characteristically shows macrophages filled with golden brown pigment.44
What Is the Differential Diagnosis of Hemolytic Glaucoma?
Hemolytic glaucoma is associated with intraocular hemorrhage, which does not necessarily have to be traumatic in origin. Apart from trauma, other causes of intraocular hemorrhage include proliferative diabetic retinopathy, hypertension, intraocular tumors, retinal detachment, sickle cell retinopathy, and retinopathy of prematurity. Hemolytic glaucoma may also be confused with ghost cell glaucoma, which is discussed below. Fortunately, the management of both hemolytic and ghost cell glaucoma is the same.
Treatment and Management
How Is Hemolytic Glaucoma Treated?
The condition usually responds to medical management with beta-blockers, α2-agonists, CAIs, and hyperosmotic agents. Typically, the problem is self-limiting, and the drugs may be gradually tapered. Resistant cases may require surgical intervention, such as anterior chamber washout (with cytologic evaluation of the aqueous to confirm the diagnosis) or pars plana vitrectomy.44
HEMOSIDEROTIC GLAUCOMA
Definition
What Is Meant by Hemosiderotic Glaucoma?
This is a rare condition associated with a long-standing intraocular hemorrhage.
What Is the Mechanism Underlying Hemosiderotic Glaucoma?
The exact mechanism is unclear. It has been postulated that hemoglobin released from degenerated erythrocytes is phagocytosed by endothelial cells of the trabecular meshwork. The iron liberated by the hemoglobin causes siderosis of the trabecular meshwork, obstructing aqueous outflow.46 It is thus a form of secondary open-angle glaucoma.
Epidemiology and Importance
What Are the Risk Factors for Hemosiderotic Glaucoma?
The main factor predisposing to this condition is the presence of a long-standing intraocular hemorrhage, allowing erythrocytes to degenerate and release their hemoglobin content.
Diagnosis and Differential Diagnosis
How Is the Condition Diagnosed?
In addition to the presence of a long-standing intraocular hemorrhage, whether hyphema or vitreous hemorrhage, gonioscopy should reveal an open angle with rusty brown discoloration.
What Is the Differential Diagnosis?
Hemosiderotic glaucoma should be distinguished from other open-angle glaucomas associated with intraocular hemorrhage. Hemolytic glaucoma is differentiated from hemosiderotic glaucoma by the presence in the former of reddish-brown blood cells, and reddish brown pigment covering the trabecular meshwork, especially inferiorly. Ghost cell glaucoma is characterized clinically by the presence of khaki-colored cells in the aqueous and vitreous, which may settle in the angle, especially inferiorly, or may be so numerous as to cause a pseudohypopyon.
As with all glaucomas associated with intraocular hemorrhage, the inciting hemorrhage may be of traumatic or nontraumatic origin.
Treatment and Management
How Is Hemosiderotic Glaucoma Managed?
The initial management of hemosiderotic glaucoma consists of lowering the IOP using beta-blockers, α2-agonists, CAIs and, when necessary, hyperosmotic agents. If medical treatment fails to control the condition, it may be due to advanced siderotic angle damage, and filtering surgery may be appropriate. However, intraocular hemorrhage may require washout (hyphema) or vitrectomy (vitreous hemorrhage).
GHOST CELL GLAUCOMA
Definition
How Is Ghost Cell Glaucoma Defined?
Ghost cell glaucoma is an open-angle glaucoma associated with degenerated erythrocytes (ghost cells).
What Is the Mechanism of Ghost Cell Glaucoma?
After a prolonged vitreous hemorrhage, ghost cells develop in the vitreous and subsequently migrate to the anterior chamber through a disrupted anterior hyaloid face. As the erythrocytes degenerate in the vitreous, they change from their typical biconvex shape to spherical khaki-colored ghost cells (erythroclasts). The latter are more rigid than normal erythrocytes and less able to pass through the trabecular meshwork.47 The condition is often transient, with the IOP returning to normal levels after the denatured cells clear from the anterior chamber angle. However, this may take months.
The onset of ghost cell glaucoma is typically 2 to 3 weeks following trauma, as it takes at least 1 to 2 weeks for erythrocytes to degenerate into ghost cells.48,49 The degree of IOP elevation depends on the number of ghost cells reaching the anterior chamber. If the number of cells is small, the IOP may be normal, and if sufficient cells are present, the IOP may reach 50 or 60 mm Hg.
Epidemiology and Importance
What Are the Risk Factors for Ghost Cell Glaucoma?
The main risk factor is vitreous hemorrhage that persists long enough to allow erythrocyte degeneration. The second is disruption of the anterior hyaloid, which allows the degenerated cells to pass forward to the anterior chamber. Both of the above events may occur as a result of ocular trauma, or from nontraumatic causes, as discussed above.
A small hyphema is unlikely to produce ghost cell glaucoma. However, in the setting of an eight-ball or near-total hyphema, ghost cells may form, which may contribute to a prolonged IOP elevation seen even after removal of the blood. Aspirates from eight-ball hyphema show a significant number of ghost cells hidden within the clot.50
Diagnosis and Differential Diagnosis
How Is Ghost Cell Glaucoma Diagnosed?
As mentioned above, the degree of IOP elevation is variable. If the IOP is in the 50 to 60 mm Hg range, there may be severe ocular pain.
With the slit lamp, using high magnification and a narrow slit beam, ghost cells are seen in the anterior chamber as tiny khaki-colored cells. If the cornea is edematous from marked pressure elevation, a drop of topical glycerol may be needed to clear the cornea and permit a clearer view of the aqueous. Occasionally, these cells may collect inferiorly in the anterior chamber, forming a khaki-colored layer. If fresher erythrocytes have also reached the anterior chamber, they too may form a layer.51
Gonioscopy may be normal. If there are enough ghost cells, they may deposit on the trabecular meshwork, giving it a khaki hue, especially in the inferior angle. The lens may be subluxated or dislocated. Ophthalmoscopy usually will reveal vitreous hemorrhage. If the lens is cataractous, ultrasonography may be needed to confirm the presence of vitreous hemorrhage.
In doubtful cases, an aqueous sample may be obtained for cytologic diagnosis. After topical anesthesia, a 30-gauge needle is used to aspirate aqueous through a temporal paracentesis.52 The aqueous sample is then spread on a slide and examined by phase contrast microscopy.53,54 Ghost cells appear as spherical cells with a thin membrane. Clumps of degenerated hemoglobin (Heinz bodies) are seen adhering to the internal aspect of the cell membrane. Unlike hemolytic glaucoma, there are few, if any macrophages. Methyl violet 1% staining may aid in the diagnosis,55 and the aspirate can be subjected to scanning and transmission electron microscopy, where available.54
What Is the Differential Diagnosis of Ghost Cell Glaucoma?
Ghost cell glaucoma does not necessarily have to occur in the setting of trauma. Originally, ghost cell glaucoma was described following pars plana vitrectomy.56 This is particularly liable to occur if only core vitrectomy is performed, leaving a large peripheral skirt of vitreous containing hemorrhagic debris. Because pars plana vitrectomy often disrupts the anterior hyaloid, it provides a route for ghost cells to reach the vitreous.
Ghost cell glaucoma can also occur after cataract extraction if the anterior hyaloid is disrupted. Two scenarios are possible. The first possibility is that the vitreous hemorrhage existed preoperatively. In such a case, ghost cells are released from an existing reservoir, and pressure elevation may occur only a few days after surgery. In the second scenario, the surgery is complicated by hyphema, and the erythrocytes pass backward into the vitreous cavity through a disrupted anterior hyaloid face. The hyphema may produce a transient IOP rise in the early postoperative period, and then weeks later the IOP may rise again as a result of ghost cells reaching the anterior chamber.57 It is worth noting that the presence of an intraocular lens does not preclude the occurrence of ghost cell glaucoma.58
It is also possible that ghost cell glaucoma occurs without prior surgery or trauma, for example in long-standing diabetic vitreous hemorrhage when a defect in the anterior hyaloid develops, presumably spontaneously, as the vitreous liquefies.59
Similar to ghost cell glaucoma, neovascular glaucoma can also cause a sudden and high IOP elevation, together with corneal edema. There may also be an associated vitreous hemorrhage. To differentiate the two conditions, a drop of glycerol is used to clear the cornea. In neovascular glaucoma, rubeosis may be seen at the pupillary margin or the angle, together with synechial angle closure, neither of which is seen in ghost cell glaucoma. In neovascular glaucoma, there are no ghost cells in the anterior chamber.51
The combination of cells in the anterior chamber with elevated IOP is also seen in hemolytic glaucoma and glaucoma complicating uveitis. In hemolytic glaucoma, the cells are reddish-brown rather than khaki brown. In glaucoma complicating uveitis, the cells are leukocytes, not khaki-colored ghost cells. Typical signs of uveitis are circumcorneal ciliary injection, keratic precipitates, and anterior and posterior synechiae. In ghost cell glaucoma, the conjunctiva is usually white and quiet despite the presence of corneal edema, the ghost cells show no tendency to adhere to the cornea, and there are no synechiae. Questionable cases may require anterior chamber aspiration for resolution of the diagnosis.51 Figure 13–4 summarizes the differential diagnosis of posttraumatic IOP elevation associated with cells in the anterior chamber.
Treatment and Management
How Is Ghost Cell Glaucoma Managed?
Initial management consists of medically lowering the IOP by aqueous suppressants such as beta-blockers, α2-agonists, and CAIs. Miotics are of doubtful value.
If the pressure does not respond to medical management, anterior chamber washout is performed using a blunt cannula inserted into the anterior chamber through a temporal paracentesis. Balanced salt solution is injected into the angle, and the paracentesis should be wide enough to allow egress of fluid. Approximately 10 mL of fluid are usually needed to wash out the ghost cells from the angle. Before the procedure, an aqueous sample may be obtained for cytologic examination.51
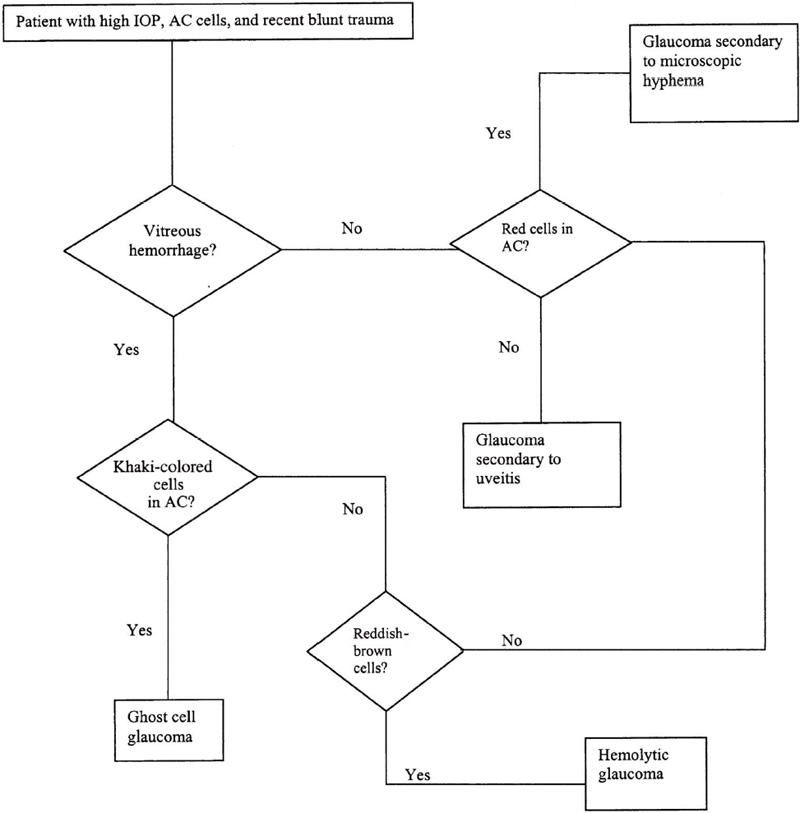
Figure 13–4. High IOP and anterior chamber cells after recent blunt trauma.
If the IOP remains elevated despite repeated anterior chamber washouts, this indicates that there is still a reservoir of ghost cells in the vitreous. In such a case, pars plana vitrectomy is required to resolve the condition.58,60,61 Special attention must be given to the removal of all ghost cells, including those in the vitreous base. If the offending ghost cells are not completely removed, the remaining cells are released by the vitrectomy procedure, actually worsening the condition.61
ANGLE RECESSION GLAUCOMA
Definition
How Is Angle Recession Glaucoma Defined?
This is a chronic open-angle glaucoma that occurs secondary to posttraumatic angle recession.
What Is the Mechanism of IOP Elevation in Angle Recession Glaucoma?
Angle recession is a deepening of the anterior chamber angle resulting from a tear in the face of the ciliary body between the scleral spur and the iris root, frequently occurring between the circular and longitudinal muscles of the ciliary body. In most cases, at least 180 degrees of the angle needs to be affected for IOP elevation to develop. Characteristically, the IOP elevation occurs years after the initial trauma that caused angle recession. In a series of 18 patients with angle recession, Herschler62 reported that the mean duration between initial trauma and the discovery of IOP elevation was 16 years.62 Mermoud et al63 studied 65 patients with angle recession and found that the latency period between injury and diagnosis of glaucoma averaged 7.6 ± 9.5 years.
The exact mechanism of IOP elevation in association with angle recession is controversial. It has been suggested that angle recession provides evidence of past injury but is not the actual cause of the glaucoma. It is believed, rather, that the initial trauma causes degeneration or proliferative changes in the trabecular tissue, which decrease outflow facility.64 Another theory is that the cause of glaucoma is the formation of a Descemet-like membrane that grows from the cornea over the anterior chamber angle.64–66
Epidemiology and Importance
What Is the Incidence of Angle Recession Following Blunt Trauma?
The incidence of angle recession following blunt trauma varies in different reports from 60 to 94%.2,15,67–69 Therefore, it should be suspected in every case of blunt ocular trauma, regardless of IOP level. Bilateral angle recession has been reported in 55 to 59% of South African patients with angle recession.63,70
What Are the Risk Factors For IOP Elevation Following Angle Recession?
The risk of IOP elevation after angle recession appears to be correlated with the extent of angle recession. Studies have shown that all patients who developed IOP elevation had greater than 180 degrees of angle recession.67,71 Similarly, Salmon et al70 reported that the prevalence of glaucoma in 146 eyes with angle recession of any degree was 5%, whereas in eyes with 360-degree angle recessions, the prevalence of glaucoma was 8%.
Spaeth72 has reported that “normal” fellow eyes in patients with unilateral angle recession glaucoma are more likely to have elevated IOP and a positive response to corticosteroid-provocative testing. It has been suggested, therefore, that eyes with an underlying tendency to develop open-angle glaucoma are more likely to develop a late increase in IOP after blunt trauma.62,72
Diagnosis and Differential Diagnosis
How Is Angle Recession Glaucoma Diagnosed?
The classic presentation of angle recession glaucoma is a unilateral IOP elevation with optic disc excavation and visual field loss.73 Angle recession is suspected when the anterior chamber appears abnormally deep. The typical gonioscopic appearance of angle recession consists of a widened ciliary body band with prominence of the scleral spur. This may be present in the whole angle, or only in scattered areas. However, this appearance may change as the tear in the ciliary body begins to scar, leading to the formation of peripheral anterior synechiae with obliteration of the angle recess. Thus, the initial depth and extent of angle recession may diminish with time. In such cases, other signs of blunt trauma may provide a valuable clue for diagnosis. Such signs include tears of the trabecular meshwork, iridodialysis, cyclodialysis, pupillary sphincter tears, absent or torn iris processes, iridoschisis, iridodonesis, phacodonesis, Vossius ring (an imprint of the pupil on the anterior caspule following blunt trauma), and dark brown to black deposits (small residua of hyphema) in the angle recess inferiorly.13
As mentioned above, angle recession may be bilateral. Therefore, gonioscopy of the fellow eye is mandatory, and is very helpful for comparison purposes. When angle recession is found, the IOP does not necessarily have to be elevated. There may be coincidental pathology decreasing the IOP (e.g., cyclodialysis), effectively “neutralizing” the IOP-elevating effect of angle recession. The other possibility is that the causative injury was relatively recent, and that the pressure elevation has not yet set in. There is usually a latent period of several years following trauma before glaucoma manifests itself. Finally, not every case of angle recession will be associated with IOP elevation.
What Is the Differential Diagnosis of Angle Recession Glaucoma?
The IOP elevation associated with angle recession is insidious in onset, asymptomatic, and typically unilateral. Therefore, the differential diagnosis of angle recession glaucoma includes all causes of chronic unilateral glaucoma, such as glaucoma associated with the pseudoexfoliation syndrome, uveitic glaucoma, glaucoma complicating intraocular tumors, neovascular glaucoma, and other causes of traumatic glaucoma. Furthermore, the condition may be superimposed on primary open-angle glaucoma, in which case examination of the fellow eye may reveal IOP elevation, an open angle, optic disc changes, and visual field loss.
Treatment and Management
How Is Angle Recession Glaucoma Managed?
Angle recession is fairly resistant to treatment. Initially, aqueous suppressants are tried, namely beta-blockers, α2-agonists, and CAIs. Pilocarpine was reported to cause a paradoxical increase in IOP in one eye.74 It is probable that the primary mechanism of aqueous drainage in that eye was uveoscleral outflow, because of damage to the trabecular meshwork. Pilocarpine is known to inhibit uveoscleral outflow in humans.
If medical treatment fails, some form of surgery is required. The average success rate of argon laser trabeculoplasty (ALT) in angle recession glaucoma is approximately 25%.75,76 Argon laser trabeculopuncture is an alternative to ALT that has a variable success rate in the literature, ranging from 42% 77 to 91%.76
Filtering procedures are less frequently successful in angle recession glaucoma than in primary open-angle glaucoma (POAG). Mermoud et al78 reported that the success rate of filtering surgery in angle recession glaucoma was 52% versus 89% for POAG at 1 year after surgery, 32% versus 84% at 2 years, and 8% versus 76% at 3 years. The main reason for failure was fibrosis of the fistula or filtering bleb.78
Given the relatively poor success rate of filtering surgery and the propensity to fibrosis, it is probably worthwhile in these eyes to perform primary filtering surgery with antimetabolites such as 5-fluorouracil (5-FU) or mitomycin C (MMC). In another study, Mermoud et al63 compared trabeculectomy alone to trabeculectomy with MMC or 5-FU, and demonstrated a significantly higher success rate with MMC at 1 and 2 years after surgery.63 Finally, if filtering surgery with antimetabolites fails, a seton procedure is required.
GLAUCOMA SECONDARY TO TRABECULAR INJURY
Definition
What Is Meant by Glaucoma Secondary to Trabecular Injury?
This is an IOP elevation that occurs secondary to trabecular injury, without the presence of angle recession.
What Is the Mechanism of Glaucoma Secondary to Trabecular Injury?
Trabecular meshwork injury occurs in the form of edema or tears. Tears of the trabecular meshwork heal in their original position, and may be impossible to detect later. The tear itself does not decrease outflow facility, but the associated scarring of the trabecular meshwork may decrease outflow facility and cause secondary open-angle glaucoma. In addition, the untorn surrounding trabecular meshwork may sustain some reversible damage, which transiently contributes to the IOP rise.13
Typically, glaucoma secondary to trabecular injury occurs in the first few days after trauma. Depending on the extent and reversibility of trabecular damage, and the preexisting facility of outflow, the glaucoma may be transient, or it may persist and require definitive management.
Epidemiology and Importance
What Is the Incidence of Trabecular Injury Following Nonpenetrating Trauma?
The occurrence of trabecular injury following nonpenetrating trauma is often overlooked. When specifically sought, the incidence may be as high as 76%, particularly in injuries that are severe enough to cause hyphema.62 As a result, trabecular injury is one of the commonest causes of early IOP elevation following trauma.
Diagnosis and Differential Diagnosis
What Are the Clinical Features of Glaucoma Complicating Trabecular Injury?
Trabecular injury should be suspected whenever there is early glaucoma following nonpenetrating trauma. The gonioscopic finding may be trabecular edema, or a tear in the trabecular meshwork. Early after trauma, these findings may be masked by concomitant hyphema or uveitis, although a mild hyphema may allow sufficient visualization of the angle to make the diagnosis. Later on, the gonioscopic findings become much more subtle, and the angle may even appear normal. If there is sufficient recovery of the trabecular meshwork, the glaucoma may resolve. Extensive trabecular damage may result in persistent glaucoma.
What Is the Differential Diagnosis of Glaucoma Complicating Trabecular Injury?
An early IOP rise following trauma can be due to trabecular injury, hyphema, or traumatic uveitis. Hyphema is distinguished by the finding of red blood cells in the anterior chamber, whereas uveitis is characterized by leukocytes in the anterior chamber. However, it is probably common for all three entities to coexist in different combinations, each contributing to IOP elevation.
After the acute phase has subsided, a persistent IOP rise due to trabecular injury should be differentiated from other secondary open-angle glaucomas occurring after trauma. These include entities associated with intraocular hemorrhage, such as hemolytic glaucoma, ghost cell glaucoma, and hemosiderotic glaucoma. Hemolytic glaucoma and ghost cell glaucoma both exhibit cells in the anterior chamber, which are absent in glaucoma resulting solely from trabecular injury. Hemosiderotic glaucoma, especially late, is not associated with cells in the anterior chamber, similar to glaucoma resulting from trabecular injury. However, hemosiderotic glaucoma may show a characteristic rusty brown discoloration, whereas trabecular injury may leave a normal-appearing angle. Siderotic glaucoma complicating an old ferrous iron body is another type of late-onset open-angle glaucoma complicating penetrating trauma. In such a case, there will be other signs of siderosis oculi, as discussed later in this chapter. Angle-recession glaucoma may be confused with glaucoma complicating trabecular injury. In most cases, gonioscopy will resolve the problem. Again, both angle recession and trabecular injury may coexist in the same patient.
Finally, a late-onset glaucoma associated with ocular trauma and a normal-appearing angle may be simply primary open-angle that had been previously undiagnosed, or was accelerated by mild trabecular injury.
Treatment and Management
How Is Glaucoma Due to Trabecular Injury Treated?
Initially, IOP is lowered by aqueous suppressants as described above. If this succeeds, the patient is kept on medical treatment, and periodic attempts are made to taper therapy. If trabecular function recovers, treatment may be discontinued, or at least reduced. If the IOP fails to respond to medical therapy, filtering surgery is warranted.
GLAUCOMA SECONDARY TO TRAUMATIC CATARACT
Definition
What Is Meant by Glaucoma Secondary to Traumatic Cataract?
This is an IOP elevation occurring in a patient having traumatic cataract resulting from nonpenetrating trauma.
What Is the Mechanism of IOP Elevation from Traumatic Cataract?
In some cases, the IOP elevation presumably results from lens swelling that produces relative pupillary block, which leads to angle closure. This may lead to glaucoma relatively early following the trauma. In other cases, the patient may present with an old traumatic cataract and pressure elevation due to associated angle recession.
Epidemiology and Importance
Is Traumatic Cataract a Risk Factor for Traumatic Glaucoma?
Patients who develop cataract as a result of nonpenetrating injury are more prone to glaucoma than patients who do not develop cataract. Coles17 reported that in a series of patients with traumatic hyphema, glaucoma occurred in 42% of patients with traumatic cataract versus only 15% of patients who did not have traumatic cataract.17
Traumatic cataract is also associated with a high risk of angle recession, as the trauma that is severe enough to cause cataract usually causes concomitant angle recession. In a series of 46 eyes with traumatic cataract in which gonioscopy was possible, Canavan and Archer2 found a 96% incidence of angle recession.
Diagnosis and Differential Diagnosis
How Is Glaucoma Secondary to Traumatic Cataract Diagnosed?
Glaucoma due to pupillary block occurs relatively early after trauma. Examination will reveal a shallow anterior chamber together with cataractous changes in the lens. Gonioscopy may show anterior bowing of the iris (iris bombé) with iridocorneal apposition obscuring a variable portion of normal angle structures.
If the pressure rise is due to concomitant angle recession, it typically occurs years after the trauma (as previously discussed). The patient’s main complaint may be visual due to the cataract, as the glaucoma associated with angle recession is asymptomatic. On examination, the lens is cataractous, and the anterior chamber is deep. Gonioscopy may show the typical changes of angle recession (see Angle Recession Glaucoma, above).
What Is the Differential Diagnosis of Glaucoma Complicating Traumatic Cataract?
Glaucoma due to pupillary block should be differentiated from other causes of traumatic glaucoma associated with a shallow anterior chamber and angle closure (Fig. 13–5). These include traumatic uveitis with ring synechiae, lens subluxation with incarceration of the lens in the pupil, forward rotation of the ciliary body with forward displacement of the iris-lens diaphragm, and malignant glaucoma.13 Traumatic uveitis is usually associated with white blood cells and flare. Iris bombé is observed when posterior synechiae develop over 360 degrees around the pupil. The anterior chamber is relatively deep centrally, as opposed to the other conditions where the anterior chamber is shallow centrally, and the iris appears to be draped over the lens. Lens subluxation may be associated with phakodonesis. Forward rotation of the ciliary body is suspected when there is choroidal effusion, which may be seen ophthalmoscopically if the media are clear, or diagnosed by B-scan ultrasonography. Definitive diagnosis of ciliary body rotation is now possible with high-frequency ultrasound biomicroscopy.79 Malignant glaucoma (aqueous misdirection syndrome) may also be differentiated from ciliary body rotation by ultrasound biomicroscopy.79,80 The differential diagnosis of angle recession glaucoma is discussed above.
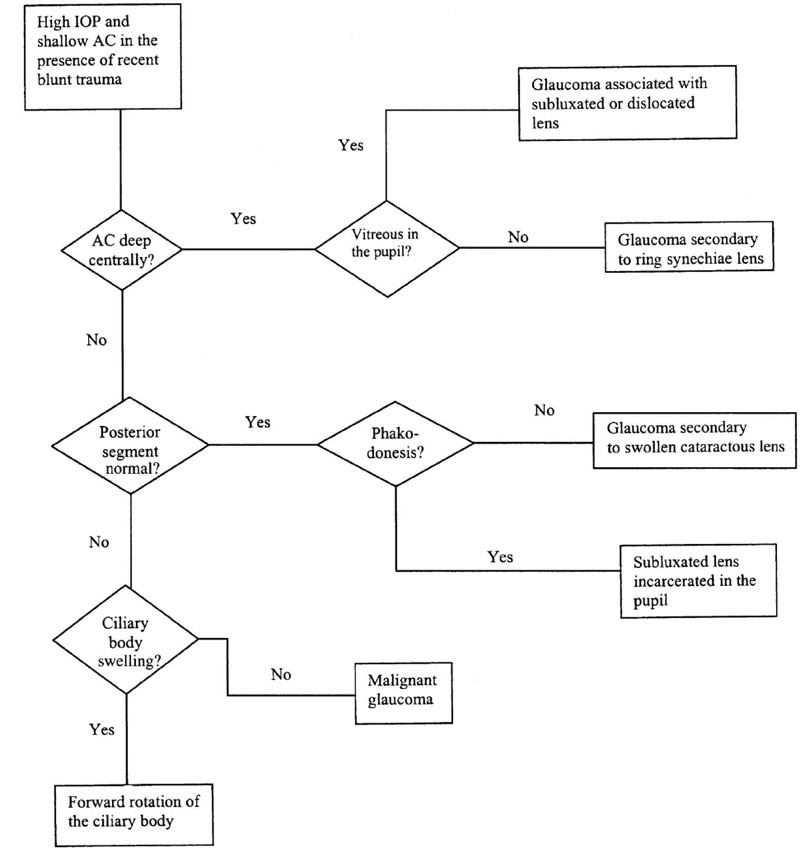
Figure 13–5. High IOP and a shallow anterior chamber after recent blunt trauma.
Treatment and Management
How Is Glaucoma Secondary to Traumatic Cataract Treated?
If a pupillary block mechanism is evident, neodymium:yttrium-aluminum-garnet (Nd:YAG) laser iridotomy is indicated to relieve pupillary block. If the cataract is visually significant, it may be removed at a later date. If the lens is severely cataractous, or if there is evidence of phakolytic glaucoma, cataract extraction may improve vision and restore normal IOP. The management of angle recession glaucoma is discussed above.
GLAUCOMA SECONDARY TO LENS DISLOCATION
Definition
What Is Meant by Glaucoma Secondary to Lens Dislocation?
This is glaucoma caused by traumatic lens displacement as a result of nonpenetrating trauma. Lens displacement is caused by zonular disruption. Partial zonular disruption leads to subluxation of the lens, where the lens is displaced but remains partially or completely within the pupillary area. Total zonular disruption leads to lens dislocation, where the lens comes to lie completely in the anterior chamber (anterior dislocation), or falls back into the vitreous cavity (posterior dislocation).
What are the Mechanisms of Glaucoma Secondary to Lens Dislocation?
With lens subluxation, forward displacement of the lens or herniation of vitreous through the ruptured zonules may cause pupillary block and angle-closure glaucoma. With total anterior dislocation, angle-closure glaucoma may occur due to pupillary block, and open-angle glaucoma may occur from direct obstruction of the iridocorneal angle by the lens or lens fragments. Posterior lens dislocation is less likely to cause glaucoma than anterior dislocation. In such cases, glaucoma may occur due to herniation of vitreous through the pupil with pupillary block. If a posteriorly dislocated lens develops hypermature cataract, phakolytic glaucoma may occur.
Epidemiology and Importance
What Is the Incidence of Lens Dislocation Following Nonpenetrating Trauma?
Lens dislocation, whether subluxation or complete dislocation, is a very common sequela of nonpenetrating ocular injury and should be suspected in every case. Mieler et al81 found that out of four golf-related nonpenetrating eye injuries, three were associated with lens dislocation. Chorich et al82 also reported four eye injuries caused by bungee cords, in which two were associated with lens subluxation.
What Is the Incidence of Glaucoma Following Lens Dislocation?
Lens dislocation is a significant risk factor for traumatic glaucoma. In a retrospective review of 73 cases of glaucoma following nonpenetrating trauma, Sihota et al83 found that 38.4% had some form of lens displacement. Rodman84 reported a 77.5% incidence of glaucoma with anterior lens dislocation and 87.5% with subluxated or posteriorly dislocated lenses in a histopathologic review of 120 cases.
Diagnosis and Differential Diagnosis
How Is Glaucoma Secondary to Lens Dislocation Diagnosed?
As mentioned earlier, lens subluxation will lead to glaucoma if there is forward displacement of the lens with pupillary block, or if there is associated vitreous herniating through the pupil and causing pupillary block. In the first instance, there is a shallow anterior chamber, the iris appearing to be draped over the lens. The lens may show phakodonesis. If this is difficult to elicit, the subluxation may be suspected when there is myopic astigmatism that is not explained by keratometry, indicating that the astigmatism is lenticular in origin. In the second instance, there is more evident subluxation, with the edge of the lens being seen in the pupil. This is associated with vitreous prolapsing through the pupil, and a shallow anterior chamber. In both cases, gonioscopy will reveal iridocorneal apposition hiding the normal angle structures from view.
Anterior lens dislocation is diagnosed when the whole lens is found to be completely in front of the iris, often with lenticulocorneal touch. Posterior dislocation is diagnosed when there is aphakia without a history of cataract extraction. The lens is seen ophthalmoscopically in the vitreous cavity if the media are clear. If the glaucoma is due to pupillary block by vitreous, there will be a shallow anterior chamber with vitreous herniating through the pupil, and gonioscopic evidence of angle closure. If the glaucoma is phakolytic, there will be cells in the anterior chamber (macrophages filled with lens debris), and the dislocated lens appears hypermature.
Both subluxation and dislocation may be masked by concomitant corneal edema or intraocular hemorrhage. In such cases, the abnormal lens position may be confirmed by ultrasonography.
What Is the Differential Diagnosis of Glaucoma Secondary to Lens Dislocation?
Glaucoma due to incarceration of a subluxated lens in the pupil should be differentiated from other causes of traumatic glaucoma associated with a shallow anterior chamber. These include glaucoma secondary to traumatic cataract (without dislocation), traumatic uveitis with pupillary block, ciliary body rotation with forward displacement of the iris-lens diaphragm, and malignant glaucoma. This has been discussed above (see Glaucoma Secondary to Traumatic Cataract). Phakolytic glaucoma with a posteriorly dislocated hypermature lens is to be differentiated from other causes of traumatic glaucoma associated with cells in the anterior chamber, namely glaucoma secondary to hyphema, hemolytic glaucoma, ghost cell glaucoma, and glaucoma complicating traumatic uveitis. The differential diagnosis of these conditions has been discussed above (see Ghost Cell Glaucoma).
Treatment and Management
How Is Glaucoma Secondary to Lens Dislocation Treated?
Glaucoma secondary to anterior lens dislocation is usually associated with lens-corneal endothelial touch. Urgent lens extraction is indicated both to relieve pupillary block and to prevent corneal endothelial decompensation. If the lens is soft, it may be removed by vitrectomy instrumentation. If the lens is hard, intracapsular extraction is more appropriate. In both cases, the procedure should include an anterior vitrectomy.
Pupillary block by vitreous may be relieved by Nd:YAG laser iridotomy. If lens extraction is indicated, anterior vitrectomy is performed at the time of lens extraction. A posteriorly dislocated lens usually does not cause problems. If the lens is hypermature and inducing phakolytic glaucoma, the lens is removed by pars plana vitrectomy techniques.
GLAUCOMA SECONDARY TO FORWARD DISPLACEMENT OF THE IRIS-LENS DIAPHRAGM
Definition
What Is Meant by Glaucoma Secondary to Forward Displacement of the Iris-Lens Diaphragm?
This a form of traumatic angle-closure glaucoma secondary to forward movement of the iris-lens diaphragm.
What Is the Cause of Forward Displacement of the Iris-Lens Diaphragm Following Nonpenetrating Trauma?
This may result either from forward rotation of the ciliary body due to posttraumatic choroidal or ciliary body edema,85 or from malignant glaucoma (aqueous misdirection syndrome).86
Epidemiology and Importance
What Is the Risk of Glaucoma After Forward Displacement of the Iris-Lens Diaphragm?
The incidence of forward displacement of the iris-lens diaphragm after blunt trauma is very low.85 However, when it does occur, the risk of glaucoma is high.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
How Is Forward Displacement of the Iris-Lens Diaphragm Diagnosed?
The condition is diagnosed when there is elevated IOP together with a shallow anterior chamber (see Fig. 13–5). The iris appears draped over an anteriorly displaced lens, as opposed to other causes of pupillary block where the anterior chamber appears relatively deep centrally with anterior bowing of the peripheral iris. Gonioscopy reveals angle closure due to iridocorneal apposition.
Ciliary body rotation is distinguished from malignant glaucoma by the presence of choroidal and/or ciliary body effusion. Choroidal effusion may be seen ophthalmoscopically if the media are clear. Peripheral annular choroidal effusion and ciliary body effusion are best detected by ultrasonography. The absence of uveal effusion is highly suggestive of malignant glaucoma.13
What Is the Differential Diagnosis of Glaucoma Secondary to Forward Displacement of the Iris-Lens Diaphragm?
This includes all causes of elevated IOP associated with a shallow anterior chamber, namely forward rotation of the ciliary body, malignant glaucoma, pupillary block due to traumatic cataract (with lens swelling), pupillary block due to forward displacement of a subluxated lens, and pupillary block in association with traumatic uveitis. This has been discussed above (see Glaucoma Secondary to Traumatic Cataract).
Treatment and Management
How Is Glaucoma Secondary to Forward Displacement of the Iris-Lens Diaphragm Managed?
Forward rotation of the ciliary body is usually self-limited and is best treated by antiinflammatory agents such as corticosteroids and cycloplegics. Aqueous suppressants (beta-blockers, α2-agonists, and CAIs) and hyperosmotic agents are used as necessary to control the IOP. Unless there is an associated pupillary block mechanism, iridotomy is neither necessary nor helpful.
Malignant glaucoma is treated initially with vigorous cycloplegia. If the condition fails to respond, posterior vitrectomy, often with lens extraction, is needed to relieve the aqueous misdirection.13
GLAUCOMA SECONDARY TO TRAUMATIC UVEITIS
Definition
How Is Glaucoma Secondary to Traumatic Uveitis Defined?
This is an IOP elevation associated with uveitis secondary to nonpenetrating ocular trauma.
What Is the Mechanism of Glaucoma Secondary to Traumatic Uveitis?
There are several mechanisms by which traumatic uveitis can cause pressure elevation. The outflow pathways may become obstructed by inflammatory cells, debris, protein, or other serum components that are liberated because of vascular incompetence.87 The trabecular endothelial cells may swell as a result of inflammation, compromising outflow. More severe inflammation may completely damage the trabecular endothelial cells. Chronic inflammation may induce sclerosis of the trabecular meshwork. The trabecular meshwork may also become obstructed by a hyaline membrane. If posterior synechiae occur, this may lead to pupillary block and secondary angle closure.88
Epidemiology and Importance
How Often Is Uveitis Caused by Nonpenetrating Ocular Trauma?
Rosenbaum et al89 studied a series of 496 patients with uveitis, and found 24 patients (4.8%) who had uveitis attributable to nonpenetrating trauma. In a series of 230 cases of anterior uveitis in children, Giles90 reported that the incidence of traumatic uveitis was 1.3% (60% were idiopathic).
Diagnosis and Differential Diagnosis
How Is Glaucoma Secondary to Traumatic Uveitis Diagnosed?
Uveitis is diagnosed by the presence of flare and cells in the anterior chamber. There may also be posterior synechiae, with or without pupillary block and iris bombé. Gonioscopy may be normal or may show a hyaline membrane over the trabecular meshwork. If there is pupillary block, iridocorneal apposition may be seen on gonioscopy. Other effects of nonpenetrating trauma may be seen, such as lens subluxation, cataract, angle recession, and so on.
After the uveitis has resolved, the IOP may remain elevated as a result of permanent trabecular endothelial cell damage. Gonioscopy may be normal, so that the diagnosis can only be made by careful history taking, and the finding of other signs of nonpenetrating trauma.
What Is the Differential Diagnosis of Glaucoma Secondary to Traumatic Uveitis?
This includes other causes of traumatic glaucoma associated with cells in the anterior chamber. Inflammatory cells may be difficult to distinguish from red blood cells. Inflammation should be suspected if the IOP is elevated with a small number of cells in the anterior chamber, because a similar quantity of fresh erythrocytes would not be expected to induce ocular hypertension in eyes with normal facility of outflow. However, if IOP returns to normal after resolution of hyphema, only to rise later in association with fine tan-colored cells in the anterior chamber, ghost cell glaucoma rather than uveitic glaucoma should be suspected. Hemolytic glaucoma is associated with reddish brown cells in the anterior chamber, which represent macrophages engulfing hemolytic debris.
Glaucoma due to pupillary block should be differentiated from other causes of traumatic glaucoma associated with a shallow anterior chamber (see Diagnosis and Differential Diagnosis under Glaucoma Secondary to Forward Displacement of the Iris-Lens Diaphragm, above).
Treatment and Management
How Is Glaucoma Secondary to Traumatic Uveitis Treated?
Initial treatment should consist of antiinflammatory and antiglaucomatous medications. Antiinflammatory medications include corticosteroids, nonsteroidal antiinflammatory drugs, and cycloplegics. Antiglaucomatous medications that may be used are aqueous suppressants such as beta-blockers, α2-agonists, and CAIs. Miotics should be avoided as they increase blood-aqueous barrier breakdown.
In cases with posterior synechiae and pupillary block, vigorous cycloplegia may break the synechiae and relieve the pupillary block. If this fails, prompt laser iridotomy is needed to reestablish normal aqueous flow.
In most cases, the IOP normalizes once inflammation resolves. If IOP elevation persists, and is uncontrollable by medication, filtering surgery may be indicated.
GLAUCOMA COMPLICATING PENETRATING TRAUMA
Definition
What Is Meant by Glaucoma Complicating Penetrating Trauma?
Penetrating (or “perforating”) trauma is an injury to the globe that results in a full-thickness laceration of the ocular wall. This may or may not be associated with a retained intraocular foreign body. Occasionally, the injurious agent may pass through the anterior portion of the globe, traverse the eye, and exit again through the posterior part of the ocular wall, producing a double penetrating injury. A penetrating injury may produce elevation of the IOP, either acutely or as a delayed effect.
What Are the Mechanisms of Glaucoma Complicating Penetrating Trauma?
Several mechanisms may produce glaucoma in an eye that has sustained penetrating trauma. A prolonged flat anterior chamber may result in peripheral anterior synechiae. Intraocular inflammation is associated with glaucoma that results from a variety of mechanisms (see Glaucoma Secondary to Traumatic Uveitis, above). Inflammation of the uninjured fellow eye, known as sympathetic ophthalmia, may produce glaucoma in the uninjured eye. Intraocular hemorrhage may occur following penetrating trauma, and may induce IOP elevation by several mechanisms, namely, glaucoma complicating hyphema, ghost cell glaucoma, hemolytic glaucoma, and hemosiderotic glaucoma. All forms of glaucoma associated with intraocular hemorrhage have been discussed above (see Glaucoma Complicating Nonpenetrating Trauma). Lens injury with violation of the lens capsule may also produce glaucoma, as will be discussed below. Epithelial down-growth and fibrous ingrowth may also cause glaucoma. A retained (and often missed) metallic foreign body may remain in the eye and cause chemical effects. Iron foreign bodies cause siderosis, and copper causes chalcosis, both conditions being associated with glaucoma.
Table 13–4 lists the causes of glaucoma complicating penetrating trauma.
What Are the Mechanisms of Lens-Induced Glaucoma in Association with Penetrating Trauma?
Lens injury may induce glaucoma through one of three mechanisms. The first is lens particle glaucoma glaucoma, where the trabecular meshwork becomes obstructed with cortical material and and inflammatory cells. Another mechanism is phacoanaphylaxis, where patients becomes sensitized to their own lens proteins and develop a granulomatous reaction around the lens. If the trabecular meshwork becomes involved in the inflammatory process, glaucoma may develop.91 Alternatively, the lens may swell, causing relative pupillary block and secondary angle closure.13
What Is the Definition of Glaucoma Secondary to Epithelial Down-Growth and Fibrous Ingrowth?
A poorly apposed corneal or corneoscleral laceration may allow epithelial elements or fibrous tissue to invade the eye. Epithelial down-growth may manifest as an epithelial cyst in the anterior chamber, or a sheet-like growth. Fibrous ingrowth usually appears in the form a retrocorneal membrane. All these conditions may be associated with glaucoma, which is usually intractable.
What Is the Mechanism of Glaucoma Secondary to Epithelial Down-Growth and Fibrous Ingrowth?
An enlarging epithelial cyst may induce glaucoma by preventing aqueous from reaching portions of the angle. There may also be associated iritis, which may elevate the IOP by several mechanisms (see Glaucoma Secondary to Traumatic Uveitis, above).
Glaucoma secondary to flat anterior chamber |
Glaucoma secondary to inflammation |
Glaucoma secondary to intraocular hemorrhage |
Lens-induced glaucoma |
Glaucoma secondary to epithelial down-growth and fibrous ingrowth |
Glaucoma secondary to siderosis |
Glaucoma secondary to chalcosis |
Sheet-like epithelial down-growth produces glaucoma through several mechanisms. Hypotony, inflammation, and shallowing of the anterior chamber lead to broad peripheral anterior synechiae. Proliferating epithelium covers the trabecular meshwork, as well as the false angle caused by peripheral anterior synechiae. Areas of trabecular meshwork underlying the epithelial sheet undergo sclerosis and necrosis.92 Chronic inflammation of the uvea leads to trabeculitis and decreased outflow facility. Pupillary block glaucoma is produced when the epithelial sheet occludes or secludes the pupil.93 Hemorrhagic and ghost cell glaucoma may result from repeated hemorrhage from friable neovascularization. Chronic hypotony may progress to intractable glaucoma if the fistula closes, either spontaneously or iatrogenically.94
Glaucoma in association with fibrous ingrowth occurs from obliteration of the angle structures, and peripheral anterior synechiae occur from persistent flat anterior chamber or inflammation or recurrent bleeding from friable neovascularization, often leading to hemolytic glaucoma.95,96
What Is Meant by Glaucoma Secondary to Siderosis Bulbil
Iron released from retained metallic foreign bodies is deposited in various intraocular structures resulting in toxic damage. This condition is termed siderosis bulbi. Involvement of the trabecular meshwork may lead to secondary open-angle glaucoma. Iron is also toxic to the retina.13
What Is Meant by Glaucoma Complicating Chalcosis?
Chalcosis is a condition where copper released from a retained intraocular foreign body is oxidized within the eye, producing tissue damage. Damage to the trabecular meshwork results in glaucoma.
Epidemiology and Importance
What Is the Incidence of Penetrating Ocular Trauma?
This varies according to sex and age, the incidence being higher at younger ages and in males. Thus, in 10- to 19-year-old males, the incidence of penetrating ocular trauma is 94.3 per million person-years, whereas in 60- to 69-year-old females, the incidence is 3.9 per million person-years.1 Alcohol and illicit drug use increase the risk for penetrating ocular injury.3
What Are the Causes of Penetrating Ocular Trauma?
Penetrating injury may result from blunt forces (10–46%), sharp laceration (34–37%), or missiles (27–41%).3,4,97,98 Intraocular foreign bodies were present in 6% of assault-related and 35% of occupational injuries in patients registered in the National Eye Trauma System (NETS).3,4
What Is the Incidence of Sympathetic Ophthalmia Following Traumatic Ocular Injuries?
The incidence of sympathetic ophthalmia following traumatic ocular injuries is 0.1 to 0.3%.99–101 Jennings and Tessler102 diagnosed sympathetic ophthalmia in 1.4% (20 patients) of the total number of referred patients with uveitis seen over an 11-year period.
How Long After Trauma Does Sympathetic Ophthalmia Occur?
Chan et al103 studied 32 cases of sympathetic ophthalmia and found that 18 cases (56%) occurred within 1 year of injury. Eight patients (25%) developed the condition more than 3 years following injury. Two cases (6%) occurred within 2 weeks after injury; 10 cases (31%) between 2 weeks and 3 months; six cases (19%) between 3 months and 1 year; and four patients (13%) between 1 and 3 years. In one other patient, the interval between injury and the occurrence of the condition was 64 years.
What Are the Risk Factors for the Occurrence of Epithelial Down-Gowth and Fibrous Ingrowth After Penetrating Trauma?
The basic risk factor for both epithelial down-growth and fibrous ingrowth is poor wound closure, whether from faulty surgical technique or because of the nature of the wound (excessively lacerated with friable edges). Poor wound closure results in incarceration of tissue, serving as a wick that facilitates postoperative wound gape. Apposition of iris to the wound provides a source of nutrients for the proliferating cells. Chronic inflammation contributes to poor wound healing. Recurrent bleeding from a vascularized, inflamed wound is thought to provide a fibrin scaffold for fibrous proliferation into the anterior chamber.94
What Is the Incidence of Epithelial Down-Growth and Fibrous Ingrowth?
The incidence of these conditions is low, and decreasing over time, mainly due to advances in microsurgical techniques. Terry et al104 estimated a rate of 0.35% epithelialization after traumatic and surgical perforations based on 28 diagnostic laboratory specimens out of 8,000 cases. Although most studies pertain to cataract surgery, they show the trend for epithelial down-growth to decrease over time; in the older literature, 17 to 26% of all enucleations after cataract surgery were due to this complication, whereas recently the incidence ranges from 0.12 to 0.08%.105 Allen106 reported an 11% incidence of fibrous ingrowth in 237 eyes enucleated for trauma. In general, the incidence of fibrous down-growth in enucleated eyes tends to be lower than epithelial down-growth.107.
What Is the Incidence of Glaucoma Secondary to Siderosis and Chalcosis?
This is a relatively rare form of traumatic glaucoma. Percival108 reported a series of 153 patients with posterior segment intraocular foreign bodies (iron or otherwise), in which only eight (5%) developed glaucoma that was not attributable to lens-induced mechanisms. Glaucoma appears to be less frequently associated with chalcosis than with siderosis.109
Diagnosis and Differential Diagnosis
How Is Glaucoma Secondary to a Flat Anterior Chamber Diagnosed?
In addition to elevated IOP, there are signs of a healed corneal or corneoscleral laceration. This laceration may have been sutured, or it may have been neglected, with the formation of anterior iris synechiae to the resultant scar. The anterior chamber may be irregular in depth. Gonioscopy will reveal a closed angle due to the presence of peripheral anterior synechiae.
What Is the Differential Diagnosis of Glaucoma Secondary to a Flat Anterior Chamber?
Other causes of a previously flat anterior chamber include corneal melting due to corneal infection (e.g., bacterial or herpetic), and sterile corneal melting as a result of collagen vascular disease (e.g., rheumatoid arhthritis). In such cases, there is no history of ocular trauma.
Peripheral anterior synechiae may form as a result of prolonged pupillary block associated with traumatic uveitis or a swollen cataractous lens, both of which may occur in the absence of penetrating trauma.
How Is Glaucoma Secondary to Inflammation Diagnosed?
Inflammation is a common sequela of penetrating trauma, and may induce pressure elevation. Inflammation may also occur in the fellow uninjured eye, presumably as a result of autosensitization of the eye to uveal pigment released into the systemic circulation at the time of trauma.110,111 The condition is termed sympathetic ophthalmia, the injured eye being the “exciting” eye, and the fellow eye being the “sympathizing” eye. This may cause IOP elevation in both eyes.
As mentioned above, inflammation is diagnosed by the presence of flare and cells in the anterior chamber, with or without posterior synechiae. The latter may induce pupillary seclusion, which leads to iris bombé and secondary angle closure. Angle closure may be confirmed by gonioscopy.
Sympathetic ophthalmia presents as bilateral granulomatous uveitis. It is therefore mandatory to examine the fellow uninjured eye if uveitis is found in the injured eye. The first symptoms of sympathetic ophthalmia are photophobia and blurring of near vision due to loss of accommodation. In addition to the usual signs of uveitis, there may be characteristic nodules occurring in the choroid, known as Dalen-Fuchs’ nodules, representing foci of granulomatous inflammation.112
What Is the Differential Diagnosis of Glaucoma Complicating Inflammation?
Glaucoma complicating inflammation is to be differentiated from other types of traumatic glaucoma associated with cells in the anterior chamber. Pupillary block glaucoma is to be differentiated from other causes of traumatic glaucoma associated with a flat anterior chamber. This has been discussed above (see Glaucoma Secondary to Traumatic Uveitis). Examination of the fellow uninjured eye is essential to exclude sympathetic ophthalmia.
Sympathetic ophthalmia does not necessarily occur in the setting of unilateral accidental trauma. It may be induced by surgery in one eye, including cataract, glaucoma, and retinal detachment surgery, all of which may presumably result in uveal incarceration in the wall of the globe. Sympathetic ophthalmia should be differentiated from other causes of granulomatous panuveitis, such as the Vogt-Koyanagi-Harada syndrome.
How Is Lens-Induced Glaucoma Diagnosed?
Lens particle glaucoma glaucoma and glaucoma secondary to phakoanaphylactic uveitis are diagnosed by the presence of a corneal or corneoscleral laceration, violation of the lens capsule, and free lens matter and cells in the anterior chamber.
Relative pupillary block is diagnosed when there is a shallow anterior chamber with the iris appearing to be draped over a cataractous lens.
What Is the Differential Diagnosis of Lens-Induced Glaucoma?
Lens particle glaucoma and glaucoma secondary to phakoanaphylactic uveitis may be confused with other types of traumatic cataract associated with cells in the anterior chamber. This includes glaucoma complicating hyphema, hemolytic glaucoma, ghost cell glaucoma (all of which are associated with intraocular hemorrhage), and glaucoma complicating traumatic uveitis. In all these entities, the lens is intact, and there is no free lens matter in the anterior chamber.
Pupillary block due to a swollen cataractous lens may occur in association with nonpenetrating ocular trauma. In such a case, there is no evidence of corneoscleral lacerations, and there may be other signs of nonpenetrating trauma, such as pupillary sphincter tears and angle recession.
How Are Epithelial Down-Growth and Fibrous Ingrowth Diagnosed?
Epithelial down-growth may present as a cyst or sheet-like growth. The time interval between injury and the occurrence of epithelial down-growth is variable, ranging from a few days to 10 years.94
An epithelial cyst may be either translucent or gray in color, usually appearing connected at one point with the traumatic wound. Rarely, the cyst will appear disconnected from the wound. Occasionally, a cyst will present in the posterior chamber, and grow into the anterior chamber through a peripheral iridectomy, or erode through the iris. The appearance and rate of growth of these cysts is variable, and they usually stabilize after a period of continued growth. There may be associated glaucoma, iridocyclitis, and pupillary distortion, and if large enough, the cyst may occlude the visual axis.94
Sheet-like epithelial down-growth is more irritating to the eye, so that the patient usually complains of tearing and dull-aching pain. Photophobia and blurred vision are less frequent complaints. There is usually ciliary injection, and often wound gape, an inadvertent filtering bleb, or a fistula demonstrable by Seidel testing. Band keratopathy is occasionally present.113 The cornea may or may not demonstrate edema overlying a posterior corneal membrane demarcated by a gray line, best seen on retroillumination. The gray line represents the edge of the advancing epithelial sheet, and may be scalloped, with focal pearl-like areas of thickening. Aqueous flare and cells may be present and indicate iridocyclitis; flare may be disproportionate to ciliary flush or symptoms.114
The epithelial membrane grows rapidly over the iris, often obscuring iris details. In brown irides, the advancing edge of the membrane may appear as an indentation in the iris. The pupil may be distorted.
On gonioscopy the epithelium may be seen as a sheet obscuring details of the trabecular meshwork. Peripheral anterior synechiae are often present. Gonioscopy can be used to assess the extent of epithelialization of the angle, through an iridectomy, and sometimes over the ciliary body and retina.94
Fibrous ingrowth is most commonly recognized as a retrocorneal membrane. Usually, the condition does not make the eye uncomfortable. The membrane may resemble an epithelial sheet, appearing as a translucent membrane with a fairly distinct border. More commonly, the membrane appears gray and felt-like with a frayed leading margin. The overlying cornea is usually edematous. Extension of the membrane over the iris, angle, and vitreous is easily recognized as a thick enveloping membrane. The pupil may be drawn into the fibrous scar.
The condition may be fairly quiescent with minimal accompanying inflammation, or there may be massive fibrous intraocular proliferation, and later retraction, resulting in retinal detachment, hypotony, and phthisis bulbi.94
What Is the Differential Diagnosis of Epithelial Down-Growth and Fibrous Ingrowth?
Epithelial cysts should be differentiated from congenital cysts of the iris stroma, which may be pigmented, arising from the pigment epithelium, or nonpigmented, arising from the iris stroma.115 Pigmented cysts are easy to differentiate from epithelial cysts, which are nonpigmented. On the other hand, congenital stromal cysts may be confused with epithelial cysts, but usually present at an earlier age, without a history of trauma or evidence of a penetrating wound.
Sheet-like epithelial down-growth is to be differentiated from other causes of retrocorneal membranes, such as a reduplicated Descemet’s membrane (as occurs in chronic iridocyclitis), detachment of Descemet’s membrane, peripheral corneal edema (usually from operative endothelial trauma), and vitreo-corneal adhesion, which may cause corneal edema and have a grayish appearance.116 The posterior lip of a shelved corneal incision (as is commonly used for phacoemulsification) may also be confused with epithelial down-growth, but is nonprogressive as opposed to an epithelial sheet.94
Fibrous ingrowth has essentially the same differential diagnosis as sheet-like epithelial down-growth. Fibrous ingrowth is distinguished from epithelial down-growth by its slow growth and vascularity.
How Is Glaucoma Secondary to Siderosis Diagnosed?
The pressure elevation associated with siderosis bulbi is asymptomatic. If there is associated cataract, the vision may be affected, even in the absence of significant retinal damage. If the lens is clear, vision may be impaired by advanced retinal damage.
In addition to pressure elevation, there is a constellation of signs due to iron deposition in the various ocular tissues. Iron deposition in the iris produces heterochromia, and mydriasis results from toxic damage to the iris sphincter. The deep cornea and anterior subcapsular portion of the lens have a rust-brown color. Advanced retinal damage produces a retinitis pigmentosa-like picture. Gonioscopy reveals rust-brown discoloration of the angle. There may also be signs of previous perforation of the globe by the foreign body, such as a sealed corneal wound, a hole, or a transillumination defect in the iris. Occasionally, a foreign body may be directly visualized in the angle by gonioscopy, or in the posterior segment by ophthalmoscopy.13
To confirm the clinical suspicion of an intraocular foreign body, appropriate radiography, ultrasonography, and CT may be of help. Magnetic resonance imaging (MRI) should be avoided as the associated magnetic field may produce movement of the foreign body, which may result in intraocular damage.117 Electrophysiologic testing may be used to assess retinal function; a depressed electroretinogram (ERG) indicates siderotic retinal damage.118
What Is the Differential Diagnosis of Glaucoma Complicating Siderosis Bulbi?
IOP elevation, a history of ocular trauma, rust-brown discoloration of the angle, and possibly mydriasis from traumatic iris sphincter rupture are also seen in hemosiderotic glaucoma (see above). However, the other signs of iron deposition seen in siderosis are absent. Angle recession glaucoma is another form of traumatic secondary open-angle glaucoma associated with traumatic mydriasis but is differentiated from siderotic glaucoma by its characteristic gonioscopic picture and the absence of other signs of siderosis.
How Is Glaucoma Secondary to Chalcosis Diagnosed?
There may be signs of foreign body entry such as a sealed corneal wound, a hole, or a transillumination defect in the iris. The foreign body may be seen in the angle by gonioscopy, or in the posterior pole by ophthalmoscopy. Imaging studies may be needed to confirm the presence of a foreign body. The iridocorneal angle is open.
Copper may be deposited in the cornea, lens, vitreous, and retina. Copper deposits in the cornea appear as a golden brown, ruby red, or green pigment ring in the peripheral Descemet’s membrane (Kayser-Fleischer ring). Lens opacities occur in the form of anterior subcapsular cataract.112 Posterior segment examination may reveal fibrillary degeneration of the vitreous, and /or maculopathy secondary to copper deposition in the retina.109 Vision may be affected by cataract, vitreous opacification, or maculopathy.
Electroretinographic (ERG) findings in chalcosis are not as striking as those seen in siderosis. If there is significant vitreous opacification, this may mildly depress the ERG; otherwise ERG is usually within the normal range.109
What Is the Differential Diagnosis of Chalcosis?
Chalcosis oculi is seen in Wilson’s disease, primary biliary cirrhosis, chronic active hepatitis, exogenous copper administration, and progressive intrahepatic cholestasis of childhood. Wilson’s disease is distinguished from other conditions by low serum ceruloplasmin and the presence of neurologic symptoms.119 In all types of chalcosis not caused by an intraocular foreign body, the condition is characteristically bilateral. Unless there are bilateral foreign bodies, posttraumatic chalcosis is unilateral.
Figures 13–6 and 13–7 outline the differential diagnosis of IOP elevation following recent and old penetrating trauma.
Treatment and Management
How Is Glaucoma Secondary to a Flat Anterior Chamber Managed?
The best treatment for this problem is prevention, by meticulous initial closure of corneal and corneoscleral lacerations. In the early postoperative period, a flat or shallow anterior chamber, hyptony, and a positive Seidel test are indicators of wound leakage. A small leak may be initially managed with a bandage contact lens. If this fails to reform the anterior chamber, resuturing of the wound is indicated. If the wound edges are excessively friable, or if it is judged that adequate suturing would induce excessive astigmatism, cyanocrylate tissue adhesive is a useful tool.
If there is established glaucoma, initial management is by aqueous suppressants. Failure of medical treatment is an indication for filtering surgery.
How Is Glaucoma Secondary to Inflammation Treated?
Initial management consists of corticosteroids, cycloplegic agents, and aqueous suppressants. Laser iridotomy may be required for iris bombé. Persistent IOP elevation despite resolution of inflammation may be an indication for filtering surgery (see Glaucoma Secondary to Traumatic Uveitis, above).
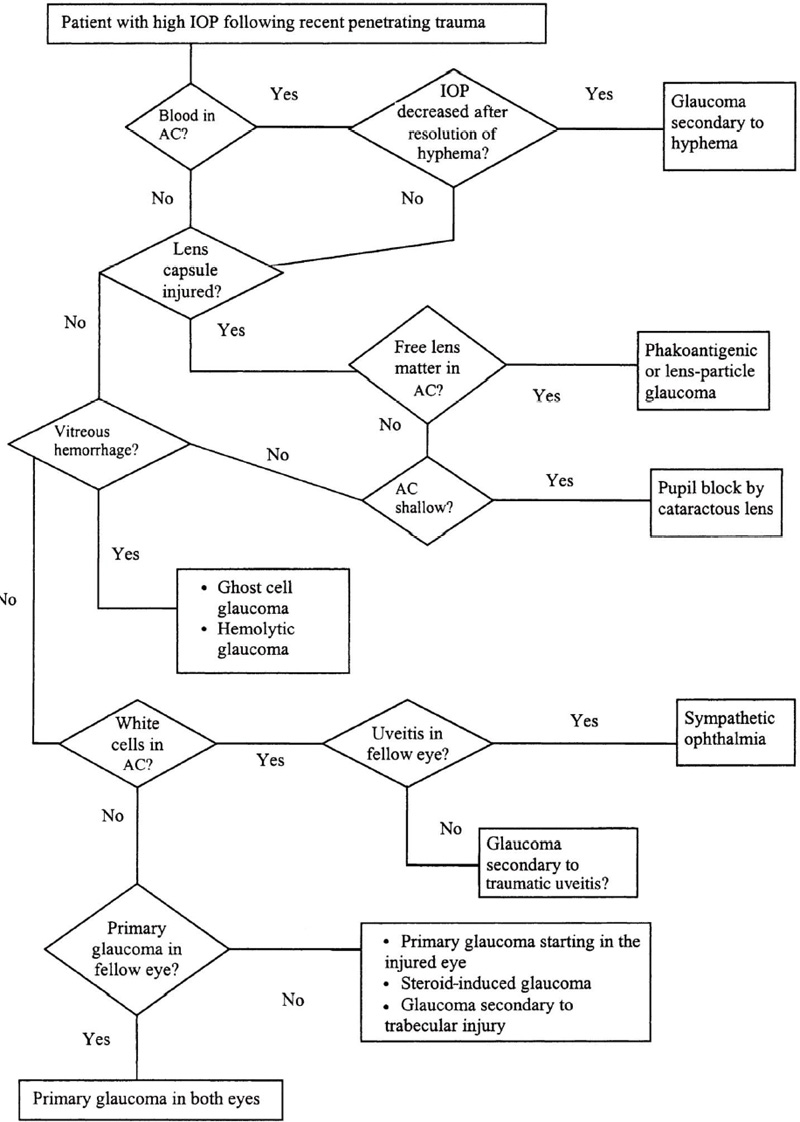
Figure 13–6. High IOP after recent penetrating trauma.
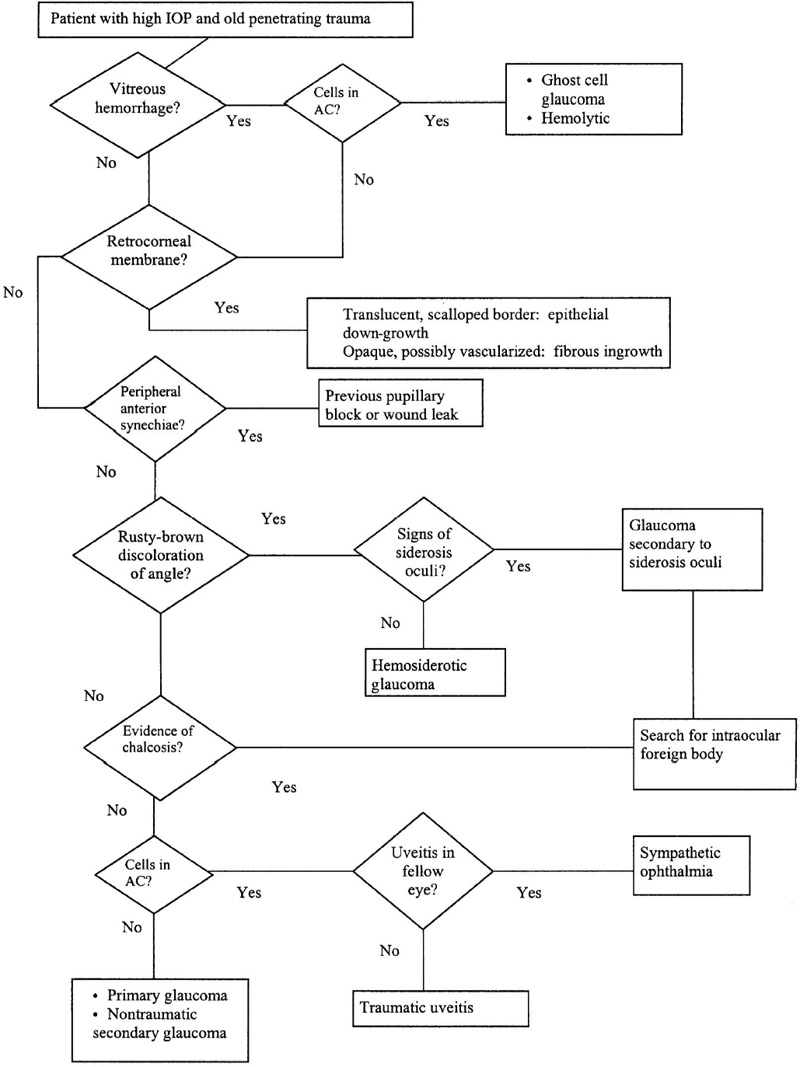
Figure 13–7. Differential diagnosis of high IOP with old penetrating trauma.
Sympathetic ophthalmia warrants special mention. The condition should always be suspected in the fellow eye in cases of penetrating ocular trauma. Once the condition is recognized, it should be treated aggressively with high doses of systemic corticosteroids and/or immunosuppressive drugs, usually for a prolonged period. The exciting eye should be removed if it does not have functional visual potential.103
How Is Glaucoma Secondary to Intraocular Hemorrhage (in Association with Penetrating Trauma) Treated?
Intraocular hemorrhage may complicate penetrating trauma and lead to several types of glaucoma, including glaucoma secondary to hyphema, hemolytic glaucoma, ghost cell glaucoma, and siderotic glaucoma. The management of these discussions is discussed above (see Glaucoma Complicating Nonpenetrating Trauma).
How Is Lens-Induced Glaucoma Treated?
Both lens particle glaucoma and glaucoma secondary to phakoanaphylactic uveitis are initially treated with aqueous suppressants to decrease IOP, corticosteroids to control inflammation, and mydriatics to prevent and/or treat posterior synechiae. If the IOP remains elevated, lens removal is indicated.91.
Relative pupillary block due to a swollen lens is also treated by lens removal. Initially, pharmacologic mydriasis or a laser iridotomy may relieve the pupillary block. If this fails, aqueous suppressants are given until the lens is removed.13
How Is Glaucoma Complicating an Epithelial Cyst Managed?
An epithelial cyst that is causing glaucoma should be widely excised, if possible intact. Large cysts that are adherent to the cornea, iris, or vitreous face are first collapsed using a 25-gauge needle. If the collapsed cyst is small, it is frozen through the cornea after an insulating air bubble is placed in the anterior chamber. Larger cysts may require vitrectomy instruments to remove adherent vitreous and iris, whereas epithelial remnants are frozen as described above. If surgical excision and freezing result in persistent corneal edema, penetrating keratoplasty may be subsequently performed to improve vision.120
How Is Glaucoma Complicating Sheet-Like Epithelial Down-Growth Managed?
Management has two aims: removing epithelial tissue and controlling glaucoma. If there is a Seidel-positive fistula (where the epithelial cells have entered), this should be closed, if necessary with the use of patch grafts.121 Preoperatively, the involved iris is marked with photocoagulation spots. The iris and vitreous with adherent epithelium are removed with vitrectomy instruments through the pars plana. Generous anterior vitrectomy is performed followed by air/fluid exchange. Epithelial tissue on the corneal endothelium, iridocorneal angle, ciliary body, and peripheral retina are treated with transcorneal and transscleral cryotherapy. If there is extensive involvement of the cornea, penetrating keratoplasty may be needed. Despite significant advances in microsurgery, epithelial down-growth remains a highly challenging problem with a high rate of recurrence.94,120
Regarding pressure control, initial management is by aqueous suppressants. Medical treatment usually fails to control pressure, and surgery is required. Conventional filtration surgery has a high rate of failure. A trial of 5-FU as an adjunct to trabeculectomy did not significantly improve pressure control.122 Some authors have reported good results with seton procedures.123
How Is Glaucoma Complicating Fibrous Ingrowth Managed?
Many eyes with fibrous ingrowth remain quiescent, and periodic observation often reveals maturation of the fibrous scar without progressive damage to the globe. However, if glaucoma does occur, the condition is initially managed with aqueous suppressants. If this fails, filtering surgery is attempted. Blind eyes are best treated with cyclodestructive procedures.94
How Is Glaucoma Complicating Siderosis Bulbi Managed?
The pressure elevation is initially managed with aqueous suppressants. If this fails, filtering surgery may be needed. If there is poor visual potential, evidenced by a subnormal or extinguished ERG, cyclodestructive procedures may be more appropriate. In the presence of good visual potential, and decreasing ERG amplitudes on serial testing, removal of the foreign body is needed to limit further retinal damage. However, this may be difficult if the foreign body is encapsulated.
How Is Glaucoma Secondary to Chalcosis Managed?
The pressure elevation is initially managed with aqueous suppressants. If this fails, filtering surgery may be needed. The foreign body is removed by vitrectomy techniques. Cataract extraction and/or vitrectomy may be needed to improve vision.
GLAUCOMA SECONDARY TO CHEMICAL INJURY
Definition
What Is Meant by Glaucoma Secondary to Chemical Injury?
Chemical injury to the eye may be caused by acids or alkalis. Alkaline chemicals, which may penetrate into the anterior chamber within seconds of contact, usually cause more severe anterior segment damage, including anterior segment ischemia. In contrast, acidic chemicals cause coagulation of tissue proteins, which limits the penetration resulting in more superficial injuries, unless the exposure is prolonged and the acid concentration is high. Both types of injury, especially alkali-induced, may be associated with glaucoma.
What Is the Mechanism of Glaucoma Secondary to Chemical Injury?
Immediately after injury, glaucoma may occur due to anterior segment shrinkage124 and increased uveal blood flow, which may be prostaglandin-mediated.125 Anterior chamber inflammation, with hypopyon in more severe cases, may develop and contribute to the pressure rise. However, in some cases damage may be so severe as to cause ciliary shutdown, which may result in hypotony.126
In the next few weeks to months, there is ongoing repair and scarring, associated with some degree of inflammation. In this phase, pressure elevation may be a result of trabecular meshwork damage that occurred at the time of injury. Glaucoma may also occur as a result of peripheral anterior synechiae formation from inflammation or pupillary block associated with posterior synechiae to the lens. The lens may become cataractous and contribute to the pressure rise by producing pupillary block or by a phacolytic mechanism when lens materials are released.127
In later phases, when the repair processes are complete, glaucoma is usually due to trabecular damage and/or the formation of peripheral anterior synechiae.128
Epidemiology and Importance
What Are the Settings In Which Chemical Injury Occurs?
Chemical injuries are relatively common. They may occur in the home, most commonly from detergents, disinfectants, solvents, cosmetics, drain cleaners, oven cleaners, ammonia, bleach, and other common household alkaline agents. In an agricultural setting, fertilizer and pesticides tend to be the offending agent. Chemical injuries occurring in industry are usually caused by caustic chemicals and solvents. When strong alkalis and acids are used as an assaultive weapon, the injuries are usually severe. Ocular alkaline injuries are slightly more common than acid injuries.129
Diagnosis and Differential Diagnosis
How Is Glaucoma Secondary to Chemical Injury Evaluated?
The following classification is a useful guide for assessment of severity and prognosis of the ocular injury:129–131
- Grade 1 (good prognosis): Corneal epithelial damage; no ischemia.
- Grade 2 (good prognosis): Cornea hazy but iris details seen; ischemia involving at least one-third of the limbus.
- Grade 3 (guarded prognosis): Total loss of corneal epithelium; stromal haze blurring iris details; ischemia involving one-third to one-half of the limbus.
- Grade 4 (poor prognosis): Cornea opaque, obscuring view of iris and pupil; ischemia involving more than half the limbus.
The corneal changes due to chemical injury make it difficult to measure the IOP by Goldmann applanation tonometry or Shiøtz tonometry. A Tonopen or pneumatonometer may be more useful to assess IOP. If the ocular injury is unilateral, these instruments may be calibrated against a Goldmann applanation tonometer in the other eye.13
After healing is complete, patients usually have variable degrees of corneal scarring with vascularization, usually associated with conjunctival scarring in the form of symblepharon. This makes it difficult to evaluate the optic disc and visual fields. The consensual reaction of the fellow eye may indicate optic disc damage (or coexisting extensive retinal disease). Ultrasound examination may detect advanced optic disc cupping, although normal ultrasound does not exclude glaucomatous cupping. Visual fields may be evaluated by confrontation, or formal perimetry (static or kinetic) using larger stimuli.13
What Is the Differential Diagnosis of Glaucoma Secondary to Chemical Injury?
The differentiation between acidic and alkaline injuries is very important, as the latter tend to be more detrimental to the eye. History taking may reveal the nature of the offending agent. Testing the conjunctival cul-de-sac with litmus paper may be informative.
The combination of high IOP, corneal epithelial ulceration, corneal stromal haze and ulceration, and variable degrees of uveitis up to hypopyon may be caused by microbial keratitis, as well as by chemical injury. In most cases, adequate history taking will immediately differentiate between the two conditions. Furthermore, chemical injury that is severe enough to cause iritis is typically associated with limbal ischemia, which is not usual in the setting of microbial keratitis.
In the late phases, the corneal scarring caused by chemical injury should be differentiated from other causes of corneal scarring such as corneal infection (viral, bacterial, fungal, protozoal) and autoimmune disease such as ocular cicatricial pemphigoid and the Stevens-Johnson syndrome.
Treatment and Management
How Is Glaucoma Secondary to Chemical Burns Managed?
The immediate management of an acute chemical injury is copious irrigation of the eye, together with removal of any material retained in the cul-de-sac. Irrigation is continued until pH testing of the conjunctiva reveals a normal pH. Topical steroids (with antibiotic cover) and cycloplegics are given to treat inflammation. However, topical steroids are used with caution, as they are liable to increase the risk of corneal melting, particularly in the second and third week following injury.132 Topical citrate, ascorbate and tetracycline may be used to limit collagenolysis.133 A bandage contact lens is useful to promote reepithelialization.
Management of glaucoma in this early phase of chemical injury is limited to aqueous suppressants and hyperosmotic agents. However, because failure of reepithelialization of the ocular surface may be impaired by topical medications, systemic medications may be preferred. Miotics are relatively contraindicated as they may aggravate anterior segment inflammation, as well as contribute to posterior synechiae that may culminate in pupillary block.13
In the intermediate phase of chemical injury (weeks to months), glaucoma may occur due to pupillary block. In such cases, initial management is by vigorous mydriatic-cycloplegic therapy. If this fails to relieve the condition, an Nd:YAG laser iridotomy may be needed. If the cornea is not clear enough to permit laser treatment of the iris, a surgical iridotomy is required. If it is judged that pupillary block is secondary to the lens, cataract extraction is indicated.
In the late phases of chemical injury, the initial management of glaucoma is medical, but filtering surgery may be required. Extensive conjunctival scarring may make conventional filtering surgery impossible, in which case glaucoma shunting procedures (or alternatively cyclodestructive procedures) should be considered.13
GLAUCOMA SECONDARY TO RADIATION INJURY
Definition
What Is Meant by Glaucoma Secondary to Radiation Injury?
This is glaucoma secondary to radiotherapy for the treatment of intraocular, periocular, and intracranial neoplasms.
What Is the Mechanism of Glaucoma Secondary to Radiation Injury?
There are several mechanisms whereby radiation can cause glaucoma. Neovascular glaucoma may be caused by radiation-induced iris and anterior chamber angle neovascularization. Hemolytic glaucoma may occur if intraocular hemorrhage complicates radiotherapy of intraocular tumors. Elevated episcleral vein pressure may result from generalized telangiectasia of the conjunctiva after anterior segment irradiation.134
Epidemiology and Importance
What Is the Incidence of Glaucoma Following Radiation Injury?
In a series of 169 patients with uveal melanomas treated with local irradiation, neovascular glaucoma occurred in 22 (13%) and was more frequent in eyes with larger melanomas and those exposed to higher radiation dosages.135
Diagnosis and Differential Diagnosis
How Is Glaucoma Secondary to Radiation Injury Diagnosed?
Regardless of the type of glaucoma, there will always be a history of irradiation, either for an intraocular tumor (external beam irradiation or brachytherapy), an orbital or eyelid tumor, an intracranial tumor, or a tumor in the head and neck area. In the case of neovascular glaucoma, the pressure rise does not occur immediately after irradiation, and there is typically a latent period between irradiation and the appearance of neovascularization. In contrast, hemolytic glaucoma and glaucoma due to elevated episcleral venous pressure may appear relatively early following irradiation.
Neovascular glaucoma may present with corneal edema if the IOP is in the 50 to 60 mm Hg range. There is usually flare in the anterior chamber, and new vessels are seen on the iris. Gonioscopy will reveal new vessels in the angle; the angle may be open or there may be broad peripheral anterior synechiae. Fundus examination may show evidence of an ablated intraocular tumor and/or radiation retinopathy (retinal hemorrhages, microaneurysms, cotton-wool spots, optic disc, or retinal neovascularization).
If the cause of IOP elevation is hemolytic glaucoma, there will be signs of hyphema or vitreous hemorrhage. Red-brown cells (macrophages laden with hemolytic debris) may be seen in the anterior chamber, and if excessive, may deposit on the angle, especially inferiorly (see above).
Glaucoma due to raised episcleral venous pressure is suspected when there is no intraocular cause of glaucoma together with dilatation and telangiectasia of the episcleral vessels. Gonioscopy may reveal blood in Schlemm’s canal.
What Is the Differential Diagnosis of Glaucoma Secondary to Radiation Injury?
The differential diagnosis of neovascular glaucoma, hemolytic glaucoma, and glaucoma secondary to elevated episcleral venous pressure is discussed elsewhere in this book.
Treatment and Management
How Is Glaucoma Secondary to Radiation Injury Managed?
Regardless of cause, glaucoma secondary to radiation injury is initially managed with aqueous suppressants. In the case of neovascular glaucoma, steroids and cycloplegics are also needed to control the associated iritis, whereas miotics are avoided as they may aggravate the iritis by increasing leakage from new vessels. The definitive management of neovascular glaucoma, hemolytic glaucoma, and glaucoma secondary to elevated episcleral venous pressure is discussed in Chapters 6,13 and 14.
GLAUCOMA SECONDARY TO ELECTRICAL INJURY
Definition
What Is Meant by Glaucoma Secondary to Electrical Injury?
This is a typically transient pressure rise that has been reported following accidental and therapeutic electrical injury such as electroshock therapy and cardioversion.136–138
What Is the Mechanism of Glaucoma Secondary to Electrical Injury?
The pressure spike that occurs after electrical injury may be related to release of pigment from the iris pigment epithelium. Venous dilatation and contraction of the extraocular muscles also may be involved in the pathogenesis of glaucoma.13
Epidemiology and Importance
How Common Is IOP Rise After Electrical Injury?
Glaucoma secondary to electrical injury is typically a transient condition, and it may or may not leave signs in the eye. Therefore, its true incidence is unknown.
Diagnosis and Differential Diagnosis
How Is Glaucoma Secondary to Electrical Injury Diagnosed?
There is usually a history of either accidental electrical injury or therapeutic electrical injury in the form of cardioversion or electroconvulsive therapy. By the time the patient is seen, the IOP may be normal. The only sign of previous injury may be loss of pigment from the iris pigment epithelium evidenced by transillumination defects in the iris seen on retroillumination. There may be dispersed iris pigment on the anterior capsule of the lens, the iris, and the corneal endothelium. Gonioscopy may also reveal pigment dispersion on the angle.
What Is the Differential Diagnosis of Glaucoma Secondary to Electrical Injury?
Transient glaucoma associated with pigment dispersion may also be seen in other conditions such as pigmentary glaucoma, uveitis, and the pseudoexfoliation syndrome. The differential diagnosis of pigmentary glaucoma is discussed in Chapter 9.
Treatment and Management
How Is Glaucoma Secondary to Electrical Injury Managed?
Due to the transient nature of the condition, treatment is seldom required.
GLAUCOMA SECONDARY TO THERMAL INJURY
Definition
What Is Meant by Glaucoma Secondary to Thermal Injury?
This is glaucoma secondary to thermal injury of the eye, usually caused by house fires and flash fires of combustible vapors and gases.
What Is the Mechanism of Glaucoma Secondary to Thermal Injury?
Glaucoma is usually associated with severe facial burns involving the eyelids. The main underlying mechanism is increased orbital pressure from orbital congestion.139 Severe burns are associated with shift of water from the intravascular to the extravascular space,140 particularly to the periocular extravascular space, which can cause swelling and tightness of the eyelids. This shift of fluid from the intravascular compartment may cause dangerous hypotension and hemoconcentration. Therefore, the administration of large quantities of intravenous fluids in severely burned patients is essential to maintain blood pressure. This is an additional factor contributing to orbital congestion. It is also possible that the IOP increases secondary to pupillary block caused by orbital pressure on the globe, displacing the lens anteriorly.139
Typically, the severely burned patient does not develop periorbital edema until a few hours after the injury. Therefore, early after the injury, the IOP may be normal, only to rise once orbital congestion sets in.
Epidemiology and Importance
What Are the Risk Factors for Glaucoma Secondary to Thermal Injury?
The main risk factor for glaucoma after thermal injury is the occurrence of orbital congestion, which is more liable to occur in association with facial burns, but may also occur in severe burns sparing the face.
Diagnosis and Differential Diagnosis
How Is Glaucoma Secondary to Thermal Injury Diagnosed?
In most cases, the severely burned patient is seen by the ophthalmologist in an emergency room or a burns unit, and the patient may not be amenable to full examination. On arrival at the hospital, some severely burned patients are able to cooperate for ocular examination, possibly to relate previous ocular problems and to permit visual acuity testing with a near-vision test card. Other patients are pharmacologically paralyzed and given mechanical pulmonary ventilation shortly after arrival, which limits cooperation for examination even though they may be fully conscious and aware.
Periorbital edema does not set in until a few hours after the injury. Furthermore, periorbital edema may occur even if the face is spared from a direct burn. Therefore, if the patient is found to have a normal IOP, examination should be repeated a few hours later so as not to miss an IOP rise associated with delayed orbital congestion.139
Treatment and Management
How Is Glaucoma Secondary to Thermal Injury Managed?
The immediate management of a severely burned patient with ocular injury consists of irrigation of the eyelids and conjunctival sacs to remove any particulate material. Singed eyelashes are removed with a moist sponge to prevent them from entering and irritating the eyes. Burned skin is treated with silver sulfadiazine when there is no known allergy to sulfonamides. Sulfacetamide ophthalmic ointment may also be applied to the globes. In general, aminoglycosides are best avoided to lessen the chance of emergence of resistant strains.
If the IOP is found to be high in association with severe periocular edema, lateral canthotomy is indicated. If possible, local anesthesia should be injected through unburned skin. Canthotomy wounds are treated with an ophthalmic antibiotic ointment.139
Future Considerations
What Are the Future Considerations for Traumatic Glaucoma?
Traumatic glaucoma is largely a preventable disease. Protective eyewear can effectively reduce the incidence of ocular trauma, both in sports and in workplaces. In an epidemiologic study of eye injuries sustained by 59 professional basketball players, 57 players (96.6%) were not wearing protective eyewear at the time of injury.141 In the United States, it is estimated that close to 1,000 eye injuries occur daily in American workplaces; up to 90% of these injuries could be prevented by the use of protective eyewear.142 Eye injuries related to assault are more difficult to prevent than eye injuries occurring in other settings. Public health efforts to reduce the use of alcohol, drugs, and firearms may reduce the incidence of injuries related to assault.3
If eye trauma does occur, it is preferable to refer the patient to a specialized eye trauma center. In the United States, there are several eye trauma centers nationwide that report to the National Eye Trauma System, which was “developed to provide optimal clinical care for severe ocular injuries, to foster research on eye injury, and to increase awareness of ocular trauma as a public health problem.”143 This may a serve as a model for more effective management of eye trauma.
Finally, the development of new antiglaucoma medications (such as prostaglandin agonists) may increase the options available for medical management of traumatic glaucoma.
References
7. Ilsar M, Chirambo M, Belkin M: Ocular injuries in Malawi. Br J Ophthalmol 1982;66:145–148.
10. Macewen CJ: Eye injuries: a prospective survey of 5671 cases. Br J Ophthalmol 1989;73:888–894.
17. Coles WH: Traumatic hyphema: an analysis of 235 cases. South Med J 1968;61:813–816.
26. Rakusin W: Traumatic hyphema. Am J Ophthalmol 1972;74:284–292.
27. Read J, Goldberg MF: Comparison of medical treatment for traumatic hyphema. Trans Am Acad Ophthalmol Otolaryngol 1974;78:OP799.
36. Rakusin W: Urokinase in the management of traumatic hyphaema. Br J Ophthalmol 1971;55:826–832.
40. Bartholomew RS: Viscoelastic evacuation of traumatic hyphaema. Br J Ophthalmol 1987;71:27–28.
44. Phelps CD, Watzke RC: Hemolytic glaucoma. Am J Ophthalmol 1975;80:690–695.
48. Campbell DG: Ghost cell glaucoma following trauma. Ophthalmology 1981;88:1151–1158.
60. Brucker AJ, Michels RG, Green WR: Pars plana vitrectomy in the management of blood-induced glaucoma with vitreous hemorrhage. Ann Ophthalmol 1978;10:1427–1437.
66. Lauring L: Anterior chamber glass membranes. Am J Ophthalmol 1969;68:308–312.
69. Mooney D: Angle recession and secondary glaucoma. Br J Opthalmol 1973;57:608–612.
79. Pavlin CJ, Foster FS: Ultrasound biomicroscopy in glaucoma. Acta Ophthalmol Suppl 1992;204:7–9.
83. Sihota R, Sood NN, Aggarwal HC: Traumatic glaucoma. Acta Ophthalmol Scand 1995;73:252–254.
86. Levene R: A new concept of malignant glaucoma. Arch Ophthalmol 1972;87:497–506.
90. Giles CL: Uveitis in childhood. I. Anterior. Ann Ophthalmol 1989;21:13–19.
91. Shields MB: Textbook of Glaucoma. Baltimore: Williams & Wilkins, 1998;252–268.
92. Jenson P, Minckler DS, Chandler JW: Epithelial ingrowth. Arch Ophthalmol 1977;95:837.
93. Chandler P, Grant WM: Lectures on Glaucoma, Philadelphia: Lea and Febiger, 1965;234–243.
94. Solomon KD, Stark WJ, Smith P, Maumenee AE, Green WR: Epithelial, fibrous, and endothelial proliferation. In: Ritch R, Shields MB, Krupin T (eds): The Glaucomas. St. Louis: CV Mosby, 1996:1325–1361.
96. Swan KC: Fibroblastic ingrowth following cataract extraction. Arch Ophthalmol 1973;89:445–449.
99. Allen JC: Sympathetic ophthalmia: a disappearing disease. JAMA 1969;209:1090.
100. Liddy L, Stuart J: Sympathetic ophthalmia in Canada. Can J Ophthalmol 1972;7:157–159.
106. Allen JC: Epithelial and stromal ingrowths. Am J Ophthalmol 1968;65:179–182.
115. Shields JA: Primary cysts of the iris. Trans Am Ophthalmol Soc 1981;79:771–809.
128. Girard LJ, Alford WE, Feldman GL, Williams B: Severe alkali burns. Trans Am Acad Ophthalmol Otolaryngol 1970;74:788–803.
129. Roper-Hall MJ: Thermal and chemical burns. Trans Ophthalmol Soc UK 1965;85:631.
131. Ballen PH: Treatment of chemical burns of the eye. Eye Ear Nose Throat Mon 1964;43:57–61.
136. Berger RO: Ocular complications of electroconvulsive therapy. Ann Ophthalmol 1978;10:737–743.
137. Berger RO: Ocular complications of cardioversion. Ann Ophthalmol 1978;10:161–164.
140. Davies JWL: Physiological Responses to Burn Injury. London: Academic Press, 1982;45–105.
142. Roll D: Eyes are the prize. Occup Health Saf 1998;67(3):32–36.
143. Parver LM: The National Eye Trauma System. Int Ophthalmol Clin 1988;28:203–205.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


