![]() 2
2 ![]()
Primary Open-Angle Glaucoma
Karanjit S. Kooner
Definition
How Is Primary Open-Angle Glaucoma Defined?
Primary open-angle glaucoma (POAG) is a chronic, slowly progressive, multifactorial, usually bilateral, though not necessarily symmetrical, optic neuropathy. It is characterized by atrophy and cupping of the optic nerve head, resulting in a distinctive pattern of visual field defects, with or without elevated intraocular pressure (IOP), in the presence of a widely open angle and in the absence of other causes of damage to the nerve fiber bundles.1
Epidemiology and Importance
What is the Etiology of POAG?
The current treatments for glaucoma focus on lowering IOP. This approach may not be enough, as 25 to 38% of patients may continue to lose visual fields and develop blindness even when IOP has been reduced to the normal range.2–4 Hattenhauer and associates’5 research has suggested that 27% of glaucoma patients go blind in at least one eye after 20 years or more with the disease. It is well known that the underlying pathology in POAG is the death of retinal ganglion cells. The cells preferentially damaged in glaucoma are the magnocellular retinal ganglion cells.6,7 Both experimental animal studies of the retina and human autopsy studies of lateral geniculate nucleus in glaucoma also point to the damage of larger retinal ganglion cells that project to magnocellular layers of the lateral geniculate.8–10
The most prevalent theories attempting to explain glaucomatous optic neuropathy are the mechanical theory and vascular theory. In the mechanical theory the emphasis is on the damage to the optic nerve neurons at the level of the lamina cribrosa by the elevated IOP.11 Alternately, the raised IOP may attenuate the sensitive microcirculation to the optic nerve head. On the other hand, the vascular theory suggests that eyes with inherently poor vascular supply to the optic nerve head are more predisposed to damage by elevated or normal IOP.12 But the cause-and-effect relationship between nerve damage and vascularity has not been established. Sponsel and coworkers13 discovered that in patients with glaucoma or ocular hypertension, the eye with the higher velocity of retinal leukocyte flow was associated with better visual function with regard to visual fields and contrast sensitivity. It is controversial whether increased blood velocity translates to enhanced perfusion pressure to a particular area. Further support for the vascular theory came after the development of the laser Doppler flowmetry (LDF) technique to evaluate the circulation of the optic nerve.14 Studies have shown diminished blood flow in the optic nerves of eyes with POAG.15,16 Similarly, optic nerve flow was decreased in patients with low systemic blood pressure and increased in patients with hypertension.17 It is still doubtful whether LDF measures the entire blood flow to the optic nerve head, though most investigators believe LDF penetrates as far as the level of the lamina cribrosa.18 As neither theory could explain all cases of glaucoma, the trend is to combine the two views together.
In the late 1960s and early 1970s another theory was proposed that elevated IOP might block axoplasmic flow at the lamina cribrosa.19,20 The resultant interruption of trophic factors to the ganglion cell body might cause the cells to initiate a suicidal response resulting in programmed cell death or apoptosis.6 The focus now has shifted more to understanding the response of nerve tissue to trauma and aging. Profiting from the data emerging from studies of central nervous system trauma and spinal cord injury, the new concepts of excitatory neurotoxins and apoptosis were applied to understanding the damage in glaucoma. When nervous tissue is severely injured, regardless of the cause, it follows the same common final pathway before neuronal death. The injurious events may relate to ischemia/hypoxia, trauma, hypoglycemia, stroke, and various acute or chronic degenerative and hereditary neuronal diseases.21 The functional damage to the nervous tissue continues to progress even after the primary cause has been removed. These new concepts may help us understand why some glaucoma patients continue to exhibit progressive neuropathy even after an offending factor such as high IOP has been controlled. Moreover, there is evidence that up to 50% of retinal ganglion cell axons may be lost by the time visual field loss and abnormal cupping are detected.22,23
The term secondary degeneration has been applied to progressive neuropathy that spreads to adjacent areas far beyond the initially injured neurons. The aim of therapeutic neuroprotection is to protect these initially spared neurons from the ravages of secondary degeneration. The biochemical events surrounding the area of nerve injury involve the release of the excitatory amino acids glutamate and asparate. These amino acids have the ability to excessively stimulate the nerve and cause neuronal fatigue, toxicity, and ultimately nerve death.24 The cytotoxic effects of glutamate on the inner layers of the retina are well known.25,26 Dreyer and coworkers27 also discovered significantly higher levels of glutamate in the vitreous samples of glaucoma patients compared to normal individuals. Similarly, Brooks and coworkers28 found significantly high vitreal glutamate concentration in dogs with primary glaucoma compared to normal animals. Even relatively minor but chronic elevation of glutamate may be toxic to the retinal ganglion cells.
After the release of glutamate at the injury site, Na+ enters the cell. There is concomitant entry of chloride ions and water, causing cellular swelling. These events constitute the acute phase of neuronal trauma. Depending on the severity of the insult, the cell may recover or proceed to further loss of function and death. In the second or delayed phase there is cellular influx of Ca2+ and once the calcium homeostasis is altered a wide variety of abnormal biochemical reactions ensue. There is release of cytotoxic enzymes such as protease, endonuclease, and lipase that destroy cell membrane. Free radicals accumulate and further disturb the essential metabolic functions of the cells. Glutamate toxicity also releases G protein via its stimulation of metallotropic receptors, which in turn activate phospholipase C. The end result is major disruption of normal cellular function.
Another important pathway for cellular death is apoptosis. This active process is different from necrosis and when triggered by calcium ion imbalance enables the cell to die without liberating its digestive enzymes. Apoptosis appears to be controlled by genes, which might be altered to prevent the deadly program. Quigley and coworkers6 have shown that ganglion cell death in glaucoma shares certain similarities with classic apoptosis. Retinal cells in glaucomatous optic neuropathy display chromatin condensation and involution or shrinkage. Neufeld and coworkers29 have demonstrated increased levels of nitric oxide synthase (NOS) isoforms 1, 2, and 3 in the optic nerve head of patients with POAG. The presence of NOS-1 and -2 suggests that nitric oxide may reach toxic levels in the optic nerve in glaucoma. Excitotoxicity, even when mild, can cause neuronal apoptosis.30 Excitotoxicity of retinal ganglion cells is mediated by overstimulation of a subtype of glutamate receptor, the N-methyl-D-asparate (NMDA). Dreyer and associates31 have shown that agents that interfere with translation or transcription of these proteins are also effective in preventing NMDA-induced excitotoxicity. Overstimulation of NMDA receptors activates NOS, which mediates increased levels of nitric oxide and superoxide anion.
A new sequence of events leading to glaucomatous nerve damage has surfaced. The first stage may be triggered in susceptible patients by factors such as elevated IOP. In the second stage, damaged ganglion cell axons either come under the influence of neurotropin deprivation and/or release excitatory amino acids. With the loss of neurotrophic support of the ganglion cells, slow death is inevitable. There is also the consensus among the proponents that these events are interconnected and once initiated are hard to control with present-day therapy for glaucoma.
Hayreh et al32 raised the issue of nocturnal hypotension in the development and progression of glaucomatous optic neuropathy. The physiologic drop in blood pressure at night, for example, may have adverse effects on a glaucoma patient with compromised optic nerve circulation. Hayreh’s group33 also prospectively investigated the effects of topical beta-blocker eyedrops on nocturnal blood pressure, heart rate, and visual field function. The study showed that in patients with normal-tension glaucoma, on beta-blocker therapy, there was a significantly more marked visual field progression (p =. 0003) than in those not using topical beta-blockers. These patients also exhibited significantly greater decrease in mean diastolic blood pressure (p =. 009) at night compared to patients with ischemic optic neuropathy.
The age-dependent reduction in the number of optic nerve fibers is also an important consideration.34 High-pass resolution and histologic studies have suggested the average loss of 10,000 nerve fibers every year after the age of 40 years. As the average number of nerve fibers is approximately 1.2 million, a person in his or her mid-80s may have lost approximately 40% of neurons, due to age-related events.
Is POAG Restricted to a Particular Geographic Area?
There is good evidence that POAG is a worldwide disease.35 Some estimates suggest that at the end of the 20th century, over 60 million people were affected by glaucoma throughout the world and nearly 10% of those affected were blind bilaterally.36 No race, community, or continent is immune from the disease. A large number of glaucoma-based epidemiologic studies have been conducted in different parts of the world and have yielded useful information, though they lack uniformity of design and definition of the disease.
The World Health Organization (WHO) Program for the Prevention of Blindness has tried to estimate the distribution of POAG based on the populations in nine different regions defined by the World Bank.37 Of the total global POAG patient population, the percent distribution in the different regions is as follows: established market economies, 17.6%, former socialist economies of Europe, 7.2%; Latin America and the Caribbean, 6.7%; sub-Saharan Africa, 19.4%; Middle East/North Africa/southwest Asia, 5.2%; China, 20.1%; India, 12.9%; other Asian and Pacific countries (high income), 3.6%; and other Asian and Pacific countries (low income), 7.2%. Therefore, developing countries account for approximately 70% of the world’s POAG cases.
In Africa, the majority of the population is black, with pockets of whites scattered throughout the continent. North Africans have Caucasian features. Due to various reasons and especially socioeconomic conditions in Africa, the prevalence of blindness is the highest in the world and rates of 3.6 to 5.2% have been reported.37 In Ivory Coast, Ahnoux-Zabsonre et al38 retrospectively reviewed charts of 33,000 patients attending a private clinic. There were 24,751 black and 8,249 white subjects. They found a prevalence of 2.1% in black and 0.75% in white patients. In both groups the prevalence rate increased with age. In black patients the mean age at detection of POAG was 46.4 ± 12.5 years, whereas it was 52.8 ± 12.2 years for white patients. Of the 571 patients with POAG, 38.5% had normal tension glaucoma. In an epidemiologic study in Cameroon looking at causes of unilateral blindness, Moussala et al39 found POAG responsible for 22% of cases, following closely cataract and ocular trauma. Ouertani et al40 examined all 856 individuals over the age of 40 years for POAG in one county of Tunisia and detected prevalence rate of 2.68%. They also found direct correlation between the prevalence rate and increasing age. The rate was 0.54% in subjects between 40 to 50 years, 1.71% in those between 51 to 65 years, and 50.63% in individuals over 65 years. Ninety-one percent of patients found to have glaucoma were unaware of the condition and 30.4% suffered from advanced disease. In the tiny nation of Togo, Balo and Talabe41 noted that 66.87% of patients with POAG were under 45 years old; 65.12% were male and 34.88% were female. Optic nerve head cupping was significantly greater in the left eye compared to the right (p < .02). Glaucoma was responsible for 17% of blindness in 523 patients found to have visual impairment in the rural communities of Central Ethiopia.42 Nwosu43 conducted a 1-year study looking for new cases of blindness at a teaching hospital eye clinic in Anambra State, Nigeria. He found that of 257 patients with blindness, glaucoma was responsible for 22.2% of visual impairment in at least one eye. A community-based cross-sectional study in the Segou region of Mali examined 5,871 inhabitants of three rural districts.44 Bilateral blindness rate was 1.7% and glaucoma accounted for 8.1% after cataract and trauma. The prevalence of POAG in central Tanzania during a survey of ocular diseases in adults was 3.1%.45 The subjects were examined from six randomly selected eligible villages.
In contrast to the results of the above studies, the prevalence of POAG in South Pacific islanders is rare. During a trachoma survey in 1955, Mann and Loschdorfer46 found only one case of POAG among 13,268 inhabitants of Papua, New Guinea.
Asia is populated by different races with varied facial features and skin color. India has a population of nearly a billion people and the WHO estimates that nearly 9 million inhabitants are blind, and that glaucoma may be responsible for 12.8% of the cases.47 The Vellore Eye Survey was conducted in Vellore in South India, and examined 972 individuals between the ages of 30 and 60 years.48 The prevalence of POAG, primary angle-closure glaucoma, and ocular hypertension were 4.1 (0.08–8.1), 43.2 (30.14–56.3), and 30.8 (19.8–41.9) per 1,000 inhabitants, respectively. The main drawbacks of the study were lack of subjects over the age of 60 years and a low response rate of only 50.3% from the eligible individuals. A similar population-based, cross-sectional study was carried out in the city of Hyderabad.49 The investigators wanted to determine the prevalence and cause of moderate visual impairment. There were 2,522 total participants of all ages, with a high response rate of 85.4%. Primary angle-closure glaucoma and POAG accounted for 0.4% and 2.0% of moderate visual impairment respectively.
China is the world’s most populated nation, with over a billion citizens. China is a relatively homogeneous society, and the prevalence of primary closed-angle glaucoma is greater than POAG. Hu50 conducted an epidemiologic survey in Shunyi County of Beijing and found prevalence rate of 0.41% for primary angle-closure glaucoma and 0.11% for POAG. Both conditions were responsible for 9.28% of the blind and 16.67% of visually impaired patients. Compared to the glaucoma prevalence of 0.60% for the entire study population, the prevalence in subjects over 40 years was 1.40%. Another study in Tongcheng County of Anhui Province found a prevalence rate of 0.31% for primary angle-closure glaucoma and 0.07% for POAG.51 The overall prevalence of glaucoma was 0.38%, whereas in individuals over the age of 40 years the rate was 0.71%. Gao et al52 examined 331 patients with glaucoma at the Third Affiliated Hospital of China Medical College and 275 patients at the eye clinic of Kyushu University in Japan during a 2-year period. Glaucoma patients made up 1.5% of the 22,869 patients in the former institute and 1.8% of the 15,585 outpatients of the latter. At the China Medical College the distributions of the various glaucomas were primary angle-closure glaucoma (76.4%), POAG (4.8%), secondary glaucoma (11.8%), and congenital glaucoma (5.7%). In comparison, the findings from Japan were primary angle-closure glaucoma (34.5%), POAG (12.7%), secondary glaucoma (22.2%), exfoliation glaucoma (14.9%), and congenital glaucoma (10.9%). A well-designed nationwide glaucoma survey was carried out in Japan under the auspices of the Japanese Glaucoma Research Club in 1988–89.53 Of the 5,092 subjects evaluated, 1.6% showed IOP abnormalities, whereas 5.1% had optic disc changes. On further examination, prevalence of POAG was found to be 0.5% while 1.4% of the subjects were diagnosed with low-tension glaucoma.
The Melbourne Visual Impairment Project was a population-based study designed to assess the distribution and causes of eye diseases in Melbourne, Australia.54 The investigators examined 3,271 residential subjects and 403 nursing home patients. The response rate was 83% for the former and 90.2% for the later. In the residential population the prevalence rate for POAG was 1.7% (95% confidence limits =1.21, 2.21). Nearly half of these participants were unaware of their disease. Primary angle-closure glaucoma was detected in two persons (0.06%), whereas six (0.2%) had secondary glaucoma. Age was a significant risk factor as the prevalence rate increased from 0.1% in people between 40 to 49 years to 9.7% in those between 80 to 89 years. A person’s gender played an insignificant role. The prevalence rate for glaucoma in nursing home patients was 2.36% (95% confidence limits = 0, 4.88).
Bonomi et al55 examined 4,297 persons (73.9% participation rate) in rural areas of northern Italy who were over 40 years of age. The investigators looked for ocular hypertension, POAG, primary angle-closure glaucoma, and normal-tension glaucoma, and found prevalence rates of 2.1%, 1.4%, 0.6%, and 0.6% respectively. In Western Scotland, Ghafour et al56 analyzed blind registration forms of new 647 legally blind patients for the fiscal year 1980. Overall, glaucoma accounted for 14.6% of legal blindness and was the second most common cause behind senile macular degeneration (29.8%). In a geographically well-defined county in central Sweden, the investigators identified glaucoma population with the help of data from local hospitals and pharmacies.57 The prevalence of glaucoma was 1.4% in individuals over 45 years of age.
The prevalence of glaucoma in Western developed countries was evaluated by Tuck and Crick.58 They analyzed data from eight surveys and estimated prevalence rates for POAG in mainly white Caucasians 40 to 89 years of age to be 1.2%. This estimate ranged from 0.2% for individuals in their 40s to 4.3% for those in the 80s. The age distributions were 7% less than 55 years, 44% between 55 and 74 years, and 49% older. They also indirectly estimated incidence from the prevalence results (implied incidence), and calculated the rate to be 0.11% per year in persons between 55 and 74 years.
St. Lucia in the West Indies is home to a relatively homogeneous black population. The investigators used a cluster sampling method and examined 1,679 individuals older than 30 years.59 The prevalence rate for glaucoma was high, being 8.8%.
How Common is POAG in the United States?
In the United States, glaucoma as a composite group is the second most frequently reported principal diagnosis at office visits to ophthalmologists after cataract.60 It makes up about 15% of all visits relating to illness or injury in ophthalmology. Among patients making return visits for the care of their previously treated eye condition, glaucoma accounted for about 20%. Among all the glaucoma-related office visits for the 2-year period of 1991–92, the diagnostic coding in descending order of frequency were unspecified glaucoma (63.2%), open-angle glaucoma (20.7%) and borderline glaucoma (14.0%). The open-angle glaucoma category was composed of POAG (10.7%), open-angle glaucoma, unspecified (9.2%), and other open-angle glaucoma (0.8%). In individuals 65 years and older, glaucoma was the third most commonly reported principal diagnosis. Although glaucoma accounted for 3.2% of all diagnoses in persons between 65 and 74 years of age, it was higher (4.4%) in persons 75 years and over. When comparing the principal diagnosis of glaucoma with all other ophthalmic and nonophthalmic diagnoses, it was the 13th most frequently mentioned condition. Glaucoma is also the second leading cause of legal blindness in America.61 In African-Americans, however, it is the most common cause of blindness and visual impairment.61 Of all adult glaucoma, POAG constitutes 60 to 70%. Approximately 80,000 Americans are blind from the disease, and 2 to 3 million have glaucoma.62 As a majority of patients are asymptomatic during the early and intermediate stages of the disease, it is estimated that approximately half of the patients may be unaware of their disease.63 Therefore, for physicians and government health planners alike, POAG poses a grave challenge. The population-based Baltimore Eye Survey examined 5,308 inhabitants of East Baltimore and discovered 161 (3.03%) cases of POAG.64 In 1975, the Framingham Eye Study found a prevalence of 3.3% for POAG among 2,477 individual examined.65
Has There Been an Increase or Decrease in POAG Over the Years?
There is some evidence, that the prevalence (the number of cases of a disease in a defined population at a defined point in time) or the incidence (the number of new cases of a disease during a defined period of time) of POAG has increased over the years. The sampling data collected by the National Ambulatory Medical Care Survey (NAMCS) of the Division of Health Care Statistics of the National Center of Health Statistics, Centers for Disease Control and Prevention, has provided useful information.60 In patients 65 years of age and older, between 1975 and 1992, glaucoma changed from being the ninth most mentioned morbidity-related principal diagnosis to the fifth. During 1975–76 there were 2.3 million glaucoma related visits and by 1991-92 the numbers showed a 284.6% increase to 8.7 million per year. Increased visit rates were observed in all age groups over 45 years. For example, in individuals 65 years of age and older, the rate for glaucoma visits increased from 5.7 visits per 100 subjects in 1975 to 19.9 visits per 100 subjects in 1992. These increased rates were observed in both sexes. According to the National Health Interview Survey (NHIS) individuals reporting a glaucoma-related condition increased from 5.7 conditions per 1,000 persons in 1977 to 10.4 conditions per 1,000 persons in 1991. Between 1982 and 1991, in persons 65 years and older, the reporting of a glaucomatous condition increased from 41.8 conditions per 1,000 persons to 57.8 conditions per 1,000 persons. However, more cases are also being discovered nowadays because of factors like better detection methods, the aging population, and heightened public awareness. As glaucoma is a disease of the elderly who are now living longer because of better health care, we can expect to encounter more cases of glaucoma in the 21st century.
What Are the Demographic Characteristics of Patients with POAG?
There are several risk factors for developing POAG and not every patient has all the known risk factors (Table 2–1). While some factors appear to complement each other, there are several that may very well operate independently. It is well accepted that POAG is a disease of the elderly and the risk increases with aging.65–67 This high prevalence in older populations may be explained on the basis of prolonged exposure to raised IOP or deteriorating microcirculation of the optic nerve head.
Several studies have demonstrated that increased IOP is associated with greater prevalence of POAG63 and glaucoma-related visual field defects in established POAG patients.68 This clinical observation is amply supported by experimental studies in primates and experience with treating patients with acute glaucoma.69 In practice, however, patients show great variability in response to elevated IOP. Population-based studies have shown that only one-tenth or less of individuals with raised IOP will have accompanying glaucomatous visual field loss.63 Longitudinal studies with ocular hypertensives have revealed that barely one-tenth of such subjects develop glaucoma over a ten-year period.70 Normal IOP may be observed in almost one-sixth of well-established glaucoma patients even on repeated examinations.63 Other deficiencies include the lack of a practical and economical means for monitoring 24-hour continuous IOP, or at least a reliable diurnal pressure. Zeimer and associates71 reported that in some glaucoma patients, IOP may be elevated upon awakening but drop precipitously within half an hour. Thus, a physician may fail to gauge the true nature of pressure spikes.
Age over 40 years Elevated IOP African American ancestry Family history of glaucoma Ocular trauma Topical, systemic, or endogenous corticosteroids Myopia Diabetes mellitus Hypertension Carotid vascular disease Dysthyroid disease Acute blood loss Anemia Vascular insufficiency Migraine headaches |
Race is an important risk factor, and African-Americans are four to five times more likely to develop POAG than other races.66,72,73 The disease also strikes them early and they usually present with severe damage at the first visit. Moreover, the glaucomatous process is more refractory to treatment and results in a higher rate of blindness.66 It is estimated that one in 10 elderly blacks and one in 50 elderly whites have glaucoma. In the Barbados Eye Study, a population-based prevalence survey, IOP was significantly higher in the black participants compared to their white counterparts.74,75 The mean values for the black and white individuals were 18.7 ± 5.2 mm Hg and 16.5 ± 3.0 mm Hg, respectively. Similarly, IOP greater than 21 mm Hg was present in 18.4% of blacks and 4.6% of whites. The prevalence of POAG in the black population was 7% and the odds of having IOP greater than 21 mm Hg was five times higher in this group. Conversely, examination of 2,773 Australian aborigines revealed no case of POAG.76 The Health and Nutrition Examination Survey of 1971 to 1974 also found that black Americans had slightly higher IOPs than their white counterparts.77 Mean IOPs of all groups increased with age, and there was positive correlation with systemic blood pressure.
A family history of glaucoma should always raise a red flag. Such a history may be found in 13 to 25% of glaucoma patients.78 Both autosomal-recessive and -dominant transmission may be involved. Miller79 examined 75 immediate descendents of patients with POAG between the ages of 15 and 60 years and performed tonography together with careful evaluation for glaucoma. The results showed that 8% had definitive POAG, 36% had suspicious outflow value, and 56% had no evidence of glaucoma. The average ages of the three groups were 48.5, 39.6, and 32.5 years, respectively. More recently in the Baltimore Eye Survey, the investigators calculated relative risk for developing glaucoma for a person with a sibling diagnosed with POAG to be 3.7-fold.80
Perfusion pressure is the difference between arterial pressure and venous pressure. IOP raises venous pressure at the exit point of the eye and thus affects intraocular blood flow. Decreased intraocular blood flow lowers perfusion pressure. Even normal IOP has an impact on the perfusion pressure, because it exceeds orbital venous pressure. Similarly, IOP induced ischemia can result from impaired autoregulation in a patient because of vasospastic disease, atherosclerosis, platelet or clotting abnormalities, and systemic hypertension.81
There is a well-known association of both systemic hypertension and hypotension in patients with glaucoma.81–84 Many patients with POAG and normal-tension glaucoma exhibit elevated blood pressure.85 Similarly, low systemic blood pressure is also a risk factor in glaucoma.82,86 It is believed that chronic hypertension may cause ischemia, and low systemic blood pressure may reduce local perfusion of the optic nerve head, especially when the eye has elevated IOP or poor autoregulation.87 Equally important is to understand the effect of physiologic nocturnal hypotension on the progression of glaucomatous field loss. Patients who exhibit greater nocturnal hypotension tend to show progressive field loss even at well-controlled IOP.
There is a close association between glaucoma and diabetes mellitus.88 Clinically, diabetic patients show an almost threefold increase in the prevalence of POAG, elevated IOP, increased IOP response to topical steroids, and large cup-to-disc (C/D) ratios as compared to nondiabetic individuals. The prevalence rate of diabetes in patients with glaucoma is reported to be 6 to 11%. On the other hand, glaucoma may provide a beneficial effect on the incidence of proliferative diabetic retinopathy. Patients with POAG and individuals exhibiting exaggerated IOP response to steroids both show increased prevalence of diabetes mellitus and positive glucose tolerance test. It is important to remember that both glaucoma and diabetes mellitus lead to blindness if undetected and untreated early on. Other common associated features of diabetes mellitus and POAG are hereditary components, tendency to produce eye damage over time, an asymptomatic nature, and the possibility of early detection.
Gender may be important, as some studies have found ocular hypertension more frequent in females and POAG more in males.83,89 Myopia may coexist in 3 to 18% of patients with glaucoma.90 The association between high myopia (>10 diopters [D]) and glaucoma is particularly significant (p < .001). Some of the high myopia-related factors implicated in the development of glaucoma are a structurally weak optic nerve in myopia, impaired aqueous outflow, choroidal vascular changes, strong familial tendency, and angle malformation. The Blue Mountain Eye Study, carried out in an Australian white community, found that glaucoma was associated with 4.2% of eyes with low myopia (> –1.0 D to < –3.0 D) and 4.4% of eyes with moderate to high myopia (> –3.0 D) compared to 1.5% of eyes with no myopia.91 This two- to threefold risk of glaucoma in myopic subjects was maintained even when other risk factors and IOP were excluded.
Thyroid disorders are frequently associated with glaucoma. Cockerham and associates92 reviewed charts of 500 patients with thyroid-associated orbitopathy and found that 120 (24%) had IOP greater than 22 mm Hg but less than 30 mm Hg. Of this group, 2% developed glaucomatous field defects over a follow-up period of 48 months. Several factors may cause raised IOP in patients with thyroid disorders, such as increased episcleral venous pressure secondary to orbital congestion, excessive mucopolysaccharide deposition in the trabecular meshwork, a direct thyrotoxic effect, or a genetic predisposition to glaucoma.
The Collaborative Glaucoma Study93 conducted between 1960 and 1973 was a prospective study that examined 5,000 subjects in five centers for risk factors that may influence the development of POAG-like visual field defects. Such defects were seen in 1.7% of the eyes. But during a period of 5 years, 98.54% of eyes with initial pressure of less than 20 mm Hg showed no glaucoma-like visual field defects compared to 93.34% of eyes with pressures greater than 20 mm Hg. Significant variables relating to glaucomatous visual field defects were reduced outflow facility (C-value 0.186 vs. 0.250), age (54.56 vs. 44.13 years), IOP (19.83 vs. 16.74 mm Hg), cup-to-disc (C/D) ratio (0.33 vs. 0.24), and pressure increase after water drinking (2.72 vs. 1.43 mm Hg). The authors stressed the multifactorial nature of glaucoma.
Are There Any Immunologic Factors Important in POAG?
Several immunologically based diseases such as rheumatoid arthritis, thyroid disturbances, migraine and Raynaud’s phenomenon are seen in patients with POAG. Wax and coworkers94 have found serum antibodies to retinal proteins and retinal immunoglobulin deposition in an eye with glaucoma. Similarly, an immunologic basis of glaucoma was also suggested by David and coworkers,95 who found an association of human leukocyte antigen HLA-DR3 allele in Caucasian patients with glaucoma. But a Spanish study found a frequency of HLA-DQA1 alleles similar in both patients with POAG and the controls.96 However, the study showed the association of POAG with other genetic markers such as acid phosphatase ACP*C alleles located at the chromosome 2p23. Recently Gil-Carrasco and associates97 detected haplotype HLA-DRB1* 0407-DQB1*0302 among Mexican Mestizo patients with POAG. They suggested that this haplotype with the disease may be the result of linkage disequilibrium or the influence of a neighboring gene.
Do Any Social and/or Economic Factors Contribute to Developing POAG?
Apart from black race, no socioeconomic, education, or occupation factor appears to have any significant effect on the prevalence of POAG. Once the disease is established, all the aforementioned factors become crucial depending on the patient’s ability to pay for the doctor visits and medications, access to health care, and understanding of the disease process.
Are There Any Genetic Considerations for POAG?
There is a strong familial association in POAG.98 The disease does not appear to follow any set familiar pattern, but a history of POAG in close relatives is much more significant than in distant relatives. Paterson99 examined 50 siblings of patients with POAG and detected the disease in 8%. Out of 125 patients suffering from POAG, Biró100 found that 16 (12.8%) were hereditary in nature.
The discovery of defective genes is an important milestone in the pursuit of early diagnosis and cure. It is essential to understand the genetic nomenclature of glaucoma in order to follow the recent advances and discoveries. To simplify the matter, glaucomas have been classified into POAG, primary closed-angle glaucoma, and congenital glaucoma. The corresponding prefixes for glaucoma loci are GLC1, GLC2, and GLC3. As new loci are discovered they are given an alphabetical letter after the GLC prefix. The first two genetic loci discovered for POAG were named GLC1A and GLC1B. Of the current eight genes or genetic regions assigned to GLC nomenclature, six relate to POAG, GLC1A–F, and two to congenital glaucoma, namely GLC3A-B. In 1993, Sheffield et al101 mapped the GLC1A region to chromosome 1q21-q31 and the group later narrowed the region to a 3-cM region between the markers D1S3665 and D1S3664 in juvenile open-angle glaucoma patients. The mutated gene was identified as myocilin by Stone et al102 in 1997. Escribano et al103 had earlier isolated myocilin or trabecular meshwork-induced glucocorticoid response protein (TIGR) from the ocular ciliary body. The TIGR gene is made up of three exons and is capable of encoding a 501 amino acid chain protein. The third exon has been identified as the site of all glaucoma-related mutations. Yokoe and Anholt104 found that the amino acid sequence encoded by the third exon was homologous to the frog olfactomedin gene and may form multimers. Wirtz and coworkers105 were successful in mapping a sixth gene for POAG, GLC1F, to 7q35-q36 in a family with a strong family history of glaucoma.
Is Community-Based Screening for POAG Helpful?
The detection and diagnosis of POAG in population-based studies is not easy. Screening surveys that do not include applanation tonometry, dilated fundus evaluation, and automated visual field examination are apt to miss significant numbers of patients. The value of IOP measurement may vary according to the time of the day as both intraday and interday fluctuations are well recognized.106 Approximately one-sixth of all POAG patients may show IOP levels below 22 mm Hg consistently during population-based studies.63 At a single screening, almost one-third to one-half of the patients with POAG may show pressures below 22 mm Hg.107 On the other hand, not all patients with high pressures have glaucoma or will develop glaucomatous optic nerve damage.63 Optic disc examination by direct ophthalmoscopy also has interobserver and intraobserver variations.108 Visual field testing, though very useful, has its own drawbacks such as time required for testing and short-term or long-term fluctuations. At a public glaucoma screening, Yamada et al109 found frequency-doubling technology perimetry superior to Damato campimetry. The former targets larger optic nerve fibers in the magnocellular pathway, which are selectively affected in early glaucoma.7 Glaucoma screenings in general are quite useful but cumbersome and time-consuming. It is now recommended that it would be more economical to target at-risk populations, such as subjects over 40 years of age, African-Americans, and the elderly.
How Common Is Blindness in POAG?
In the United States there is no central agency for blindness registration. Therefore, we can only estimate the number of blind individuals. The definitions of legal blindness and visual impairment are also not standardized worldwide and therefore pose difficulties in comparing their prevalence. Legal blindness in North America is defined as best corrected visual acuity of 20/200 or less or a visual field of less than 10 degrees in the better eye. The WHO defines blindness as visual acuity of less than 3/60 (0.05) or corresponding visual field loss in the better eye with best possible correction.47 Visual impairment corresponds to visual acuity of less than 6/18 (0.3) but equal to or better than 3/60 (0.05) in the better eye with best possible correction. It is estimated that 71% of blindness in the world is from three conditions: cataract, trachoma, and glaucoma. Approximately three-fourths of all blind individuals reside in Africa and Asia. The estimates by WHO suggest that depending on geographic location, glaucoma is responsible for 5.7 to 22.7% of all blindness worldwide. It may be fair to estimate that around 10% of global blindness may be from glaucoma. The country with the largest percent of glaucoma-related blindness is China, where more than half of the world’s patients with POAG are believed to reside. In the United States, the estimate for legal blindness from glaucoma is 16.2 cases per 100,000 population.110 Most experts believe that these data underestimate the real problem by two- to threefold because of underreporting of blindness in the country.
How Much Does the General Population Know About Glaucoma?
The knowledge about glaucoma is quite scanty in the general population. In Germany, Pfeiffer and Krieglstein111 surveyed 2,600 men and women over the age of 14 years. Only 30.0% of the subjects had heard about glaucoma. The awareness was greater in individuals who wore glasses or contact lenses (44.0%). The symptoms believed to be associated with glaucoma were blurred vision (39.0%), pain (28.0%), and difficulty in reading (22.0%). Approximately 11.0% knew that there were few subjective symptoms in glaucoma while 29.0% thought they would be able to feel elevated IOP. Two factors responsible for poor vision were believed to be excessive reading (16.0%) and smoking (11.0%). Therapeutic measures mentioned for glaucoma included surgery (63.0%), laser treatment (26.0%), and medications (23.0%). The sources of glaucoma information were friends (44.0%), doctors (13.0%), and opticians (2.0%). There was little correlation between knowledge of glaucoma and a person’s education, profession, and income.
Does Glaucoma Reduce Life Expectancy of Patients?
Several studies have looked at the question of adverse effects of glaucoma on life expectancy of persons with glaucoma.112,113 Hiller and associates114 used data from the Framingham Eye Study and Framingham Heart Study to see if raised IOP or a history of treatment for glaucoma is associated with decreased survival. They divided patients into three groups: low pressure (<20 mm Hg), medium pressure (20–25 mm Hg), and high pressure (> 25 mm Hg). The death ratio for the group with medium IOP relative to the group with low pressure was 1.04. The group with high pressure had a corresponding death ratio of 1.56. The data suggested that high IOP or presence of glaucoma is a marker for decreased life expectancy.
Diagnosis and Differential Diagnosis
What Are the Presenting Symptoms of POAG?
There may be no symptoms or the patient may present with nonspecific symptoms (Table 2–2). These patients may visit an ophthalmologist as part of a routine eye checkup or in relation to some symptom of an ailment such as diabetes mellitus, hypertension, thyroid dysfunction, anemia, or some cardiovascular function.
Asymptomatic Blurry vision, decreasing vision Ocular pain Difficulty driving, especially at night Frequent change of glasses |
What Are Some of the Most Pertinent Questions to Ask the Patient?
Once glaucoma is suspected, the comprehensive evaluation should relate to present or past ocular history, family and social history, medical history, use of topical and/or systemic drugs, and any drug allergies. Rule out local or systemic contraindications to the use of glaucoma medications such as certain cardiovascular, bronchospastic, central nervous system, and renal disorders. For example, the physician may want to avoid topical beta-blockers in patients with asthma, and carbonic anhydrase inhibitors in patients with history of renal stones.
How Is a Patient with POAG Evaluated?
After a complete history one needs to know the status of the best corrected visual acuity. Some patients may notice a dramatic drop in their vision for the first time after the good eye is covered. Pupillary reflexes should be checked to rule out subtle or early relative afferent pupillary defect. Other steps are described below.
Is IOP Elevated in All Patients?
As previously mentioned, not all patients exhibit elevated IOP at all times. The term normal tension or low-tension glaucoma is reserved for patients who never show raised IOP. This does not mean that IOP stays normal at all times in these patients. It may be rising at certain times of the day, and this observation has prompted some to recommend diurnal or serial tonography. Alternatively, IOP may be checked at different times of the day on different visits. Goldmann-type applanation tonometry is preferred for standardized testing. Time of the day should always be recorded for diurnal comparison in the future. IOP is influenced by both physiologic and pathologic factors, and it is always prudent to perform multiple pressure measurements over a period of days or weeks to better assess the patient’s pressure status. The average diurnal variation of IOP is approximately 6 mm Hg, and patients with glaucoma may exhibit variations of up to 30 mm Hg.115
Why Is Gonioscopy Essential?
A careful evaluation of the anatomic angle helps to exclude patients with narrow angles, angle closure, or other secondary forms of glaucoma. Excessive pigmentation may suggest trauma, pigment dispersion, pigmentary glaucoma, pseudoexfoliation of the lens, or intraocular tumor. Prominent angle recession may explain unilaterally elevated IOP. In an obviously quiet eye, it is important to rule out any prior use of topical corticosteroids.
How Should the Optic Disc and Nerve Fiber Layer Be Examined?
A critical part of glaucoma evaluation, the posterior fundus including the optic nerve head, is ideally examined through a dilated pupil.116 The use of a slit-lamp biomicroscope and a magnifying aid allows a stereoscopic evaluation.117 Periodic stereo photography provides a more practical and inexpensive objective follow-up of the status of the optic nerve head. The nerve fiber layer may be evaluated by using red-free illumination from a direct ophthalmoscope or a biomicroscope. The posterior fundus should be carefully examined to rule out other causes of glaucoma-like visual field defects (Table 2–3). The new nerve fiber analyzers using scanning laser or confocal laser provide more objective evaluation of the optic nerve head.118,119 Thus, interobserver and intraobserver errors are excluded.108,120 Three-dimensional computer assessment of the optic disc has taken disc evaluation one step closer to a perfect objective test.121 If these facilities are not available, then a detailed description and drawing of the optic disc or a mono-photograph should suffice.
Tilted disc Disc drusen Optic pits and other congenital defects Retinal or choroidal diseases |
The changes on the optic nerve head are not similar in all types of glaucoma, and glaucomatous eyes may lose retinal nerve fibers before clearly visible changes on the disc are evident.122 After evaluating the size and shape of the disc, attention is directed to the surface of the nerve head. Compared to focal nerve damage, it is more difficult to diagnose diffuse nerve fiber loss. The characteristics of glaucomatous optic nerve damage are enumerated in Table 2–4. The C/D ratio should be noted in both the horizontal and vertical meridians. A vertically oval cup in the absence of a vertically elongated disc, C/D disparity of >0.2 between the eyes, notching, thinning of neuroretinal rim, and optic disc pallor in the presence of hemorrhage are some of the salient features of glaucomatous damage. Peripapillary atrophy or choroidal sclerosis and thinning of the retinal arterioles may be signs of ischemia. In a patient with POAG, splinter hemorrhage on the disc may be accompanied by a new nerve fiber bundle defect.123 Disc hemorrhage may represent an acute ischemic event and is seen more frequently in patients with systemic hypertension.
Asymmetrical cupping Vertically oval cup Generalized enlarged cup Thinning or notching of the disc rim Disc hemorrhage Peripapillary atrophy Baring of lamina cribrosa Nasalization of optic nerve head blood vessels Thinning of disc arterioles Baring of circumlinear blood vessels |
Four different types of glaucomatous optic discs have been described in glaucoma. The focal glaucomatous disc is characterized by localized neuroretinal rim loss at the inferior and/or superior pole of the optic nerve head.124 With progressive deepening, the lamina cribrosa becomes exposed and is called laminar dot sign. There is a close correlation between the enlarged cup volume and glaucomatous visual field loss.125 Associated peripapillary atrophy is also quite common. Myopic glaucomatous discs are tilted with a shallow appearance, a myopic temporal crescent of peripapillary atrophy, and thinning of the superior and/or inferior neuroretinal rim in the absence of signs of degenerative myopia.126 Senile sclerotic or atrophic glaucomatous optic discs show diffuse neuroretinal rim tissue loss.127 There is an associated complete ring of peripapillary atrophy and choroidal sclerosis. Eyes with generalized enlargement of the optic disc cup are characterized by enlarged round cups with no localized areas of neuroretinal rim loss or pallor. The majority of patients with glaucoma, however, tend to exhibit signs of two or more disc types.
Detection of optic nerve fiber damage is central to the diagnosis of POAG. It is also believed that damage to the optic nerve head occurs ahead of any recognizable change in the visual fields.122,128 An optic nerve head with a large cup is also more susceptible to raised pressure as compared to an eye with a small or no cup. Larger cups may be associated with higher levels of IOP. Iester and Mikelberg129 found no morphometric differences between high-tension glaucoma and normal-tension glaucoma patients as measured by scanning laser ophthalmoscopy. In patients with advanced glaucomatous optic atrophy, factors responsible for progressive visual loss are elevated IOP and noncompliance with treatment.68
How Should the Visual Field Be Evaluated?
The visual field is measured by the automatic static threshold method or by employing carefully the manual combined kinetic and static threshold technique. In cooperative patients, a fair amount of field defects may be detected by a quick confrontation method. There are a number of well-recognized field defects seen in glaucoma patients regardless of the type of the disease130 (Table 2–5). These defects are the consequence of damage to the nerve fiber layer of the retina. The earliest changes may appear in the paracentral area in the form of decreased sensitivity or scotomas. The latter may be relative or absolute in nature. If the patient has developed a notch on the nerve head, it may be possible to predict the location of the field defect. As the disease progresses, the scotomas coalesce to form an arc-shaped defect often called arcuate scotoma. A nasal step may appear superiorly or inferiorly and is a frequent finding. An arcuate scotoma and a nasal step may join to form a much larger defect ultimately appearing as an altitudinal defect. In glaucoma there is usually a spillover to the other half of the field, in contrast to the neat bisection seen in central nervous system lesions. There is a well-accepted concept of localized and diffuse loss in glaucoma.131 The former includes arcuate and paracentral defects, while the latter manifests as a reduction in sensitivity over the whole visual field. The localized loss is attributable to normal IOP, whereas the diffuse loss appears to be associated with high IOP.132
Arcuate defect Nasal step Paracentral scotoma Generalized depression Altitudinal defects |
Most patients find visual field testing quiet frustrating and cumbersome. It is therefore crucial for the physician to spend some time explaining the procedure and its importance. An experienced and competent technician can play an important role in alleviating the fears of the patient. The patient’s refractive error should be corrected and an appropriate reading is essential. Miotic pupils should be dilated with the same mydriatic agents each time and the pupil size measured. The visual field changes from small pupils and the interference from the rims of corrective lenses may complicate an already difficult situation.
Is Electrophysiologic Testing Helpful in Glaucoma?
Various electrophysiologic tests have proved not very helpful in glaucoma. For instance, luminance or standard-flash electroretinogram (ERG) is altered only in advance glaucoma.133 Pattern ERG (PERG) has been found to be abnormal in several studies in patients with glaucoma, but the abnormalities do not match with other psychophysical test results in glaucoma.134 The pattern visual-evoked potential (PVEP), on the other hand, is abnormal only in half of the patients with glaucoma.135 Graham and coworkers136 have used multifocal PVEP to determine visual field loss in glaucoma. In their study involving 43 glaucoma patients, the bipolar PVEP corresponded well with Humphrey visual field defects.
How Is a Patient with POAG Diagnosed?
A patient with POAG may present with any one or more of these prominent features: (1) elevated IOP, (2) increased cupping and atrophy, and (3) glaucoma-like visual field defect.
(1) How Should a Patient with Elevated Pressure Be Evaluated?
A patient may present with raised pressure in one or both eyes (Fig. 2–1). A majority of patients with elevated pressures show an inequality of values in both eyes or even relatively normal pressure in one eye. Sometimes one eye may show a lag period of several months to several years before the IOP starts to rise.
What Are the Gonioscopic Features?
The iridocorneal angle is moderate to wide open and all the angle structures are prominent. If the angle is narrow or closed the patient should be accordingly managed (see Chapter 5). A patient may have angle recession in one or both eyes, and a history of ocular trauma is useful (see Chapter 13). This is also an opportunity to rule out other causes of raised IOP such as pigmentary glaucoma, pigment dispersion, inflammatory membranes and deposits, foreign bodies, anterior segment inflammation, and intraocular tumors. If there are features of raised episcleral pressures present then the management is different (see Chapter 6).
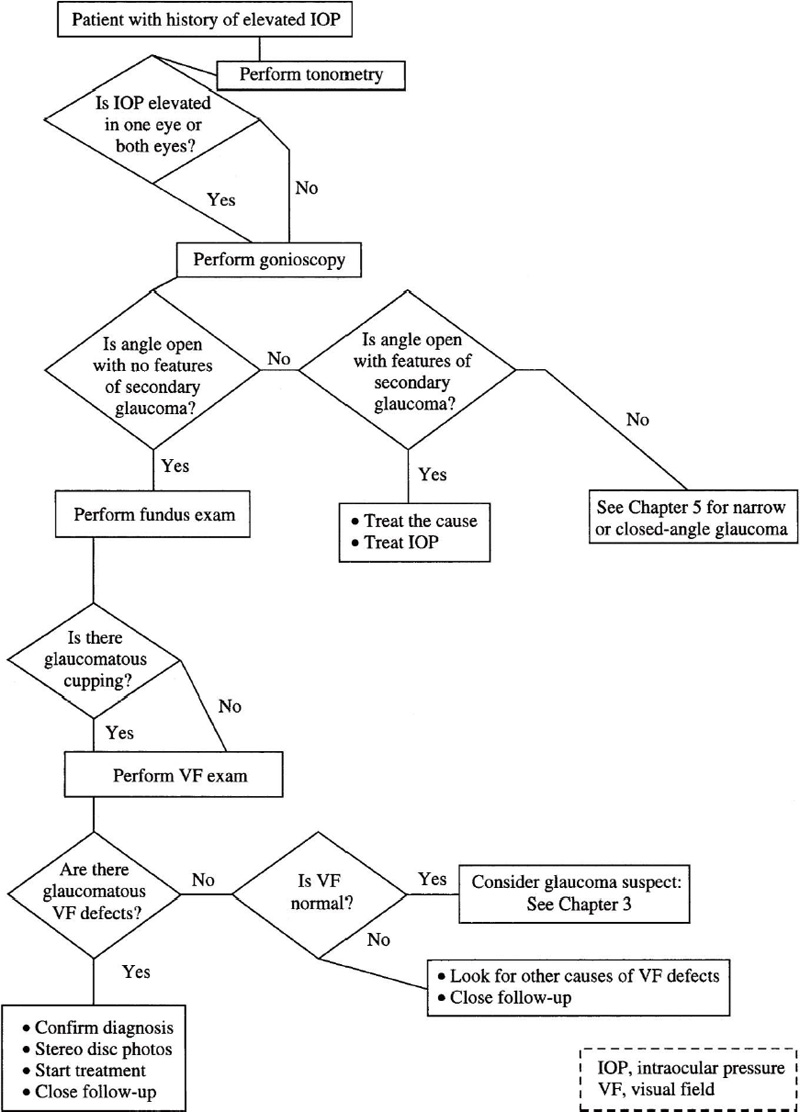
Figure 2–1. Management of a patient who presents with elevated IOP.
Is There Glaucomatous Cupping?
The changes on the optic nerve head should be carefully evaluated and compared with the other eye. If the optic disc changes are asymmetrical then there should be a very high suspicion for glaucoma. Occasionally, the disc features may suggest glaucomatous damage but still appear symmetrical. In such a situation visual fields and other risk factors would help to rule out physiologic cupping or congenital deformity of the optic nerve disc.
Are There Glaucomatous Field Defects?
In most patients visual field examination is most crucial. If the fields are normal in both eyes, then the patient may have any of the three diagnoses depending on the IOP, optic nerve head, and risk factor: glaucoma suspect (ocular hypertensive), physiologically large cups, or congenital deformity of the optic nerve head. When there are typical glaucomatous field defects in one or both eyes, then the glaucoma diagnosis is more likely as long as the IOP and optic nerve head features support the clinical impression. All efforts should be made to rule out conditions that may mimic glaucomatous field defects as discussed previously.
(2) How Is a Patient with Increased Cupping and Optic Atrophy Evaluated?
The features of glaucomatous optic nerve damage have been discussed before, and all other conditions that may simulate glaucomatous damage should be ruled out. A patient may show signs of damage in only one eye and this should alert the clinician to exclude secondary causes of unilateral nerve damage such as congenital deformity, trauma, inflammation, space-occupying lesions, and past or present use of topical corticosteroids (see Fig. 2–2).
Is the IOP Normal or High?
Careful measurement of IOP may reveal normal, low, or raised pressure in one or both eyes. A single pressure reading is noncontributory and may have to be repeated at different times of the day. Elevated IOP aids in the diagnosis but a normal or low pressure does not exclude glaucoma.
What Does Gonioscopy Reveal?
Gonioscopy is an essential step in the evaluation of patients manifesting suspicious optic disc changes. A closed angle may suggest primary or secondary angle-closure glaucoma and the management is discussed in Chapter 5. A patient exhibiting signs of narrow angle may be harboring combined mechanism glaucoma or impending angle-closure glaucoma, or may be a glaucoma suspect. If the iridocorneal angle is open, then the list of differential diagnosis is long. This individual may have POAG, low-tension or normal-tension glaucoma, ocular hypertension, secondary glaucoma, physiologic cupping, or congenital optic nerve deformity. The next step is evaluation of the visual fields.
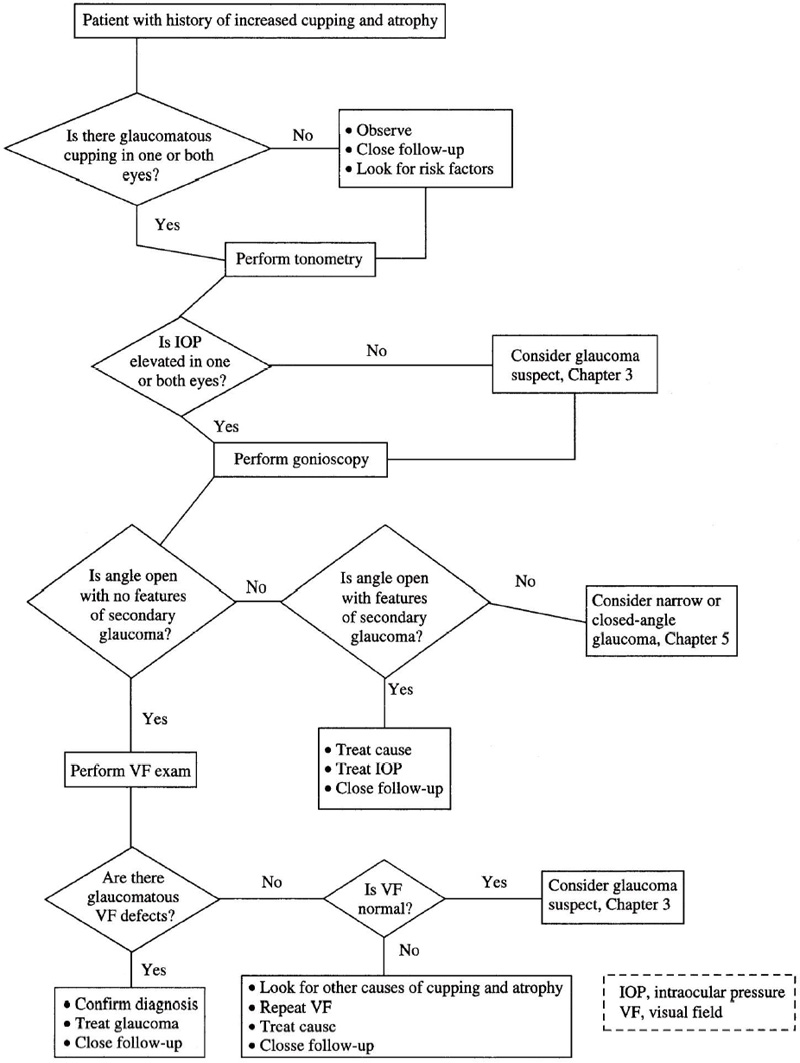
Figure 2–2. Management of a patient who presents with history of increased cupping and atrophy.
Are the Visual Fields Normal or Abnormal?
The visual field examination may reveal characteristic changes in one or both eyes but may also be normal in both eyes. In the latter situation, one has to consider ocular hypertension, physiologic cupping, and/or congenital deformity. A patient with glaucomatous visual field defects in one or both eyes and normal pressures may harbor normal- or low-tension glaucoma. On the other hand, a patient with typical glaucomatous field defects in one or both eyes and high IOP needs to be carefully evaluated for secondary causes of elevated pressure before a diagnosis of POAG is established.
(3) How Is a Patient Who Presents with Glaucomatous Visual Field Defects Evaluated?
It is not uncommon that a diagnosis of glaucoma is initially entertained when a patient shows suspicious field defects during the course of some other ocular investigations. If in doubt, the visual fields may be repeated to rule out short-term or long-term fluctuations in patient responses. The glaucomatous field defects may be unilateral or bilateral and one should rule out other causes of glaucoma-like field changes (Table 2–2). The next step is to check ocular tensions (Fig. 2–3).
How Are the Ocular Pressures?
The IOP may be elevated in one or both eyes and a record of past pressures would be very helpful to better understand the range of IOP fluctuations. In any case, knowledge of the status of the iridocorneal angle would be very helpful.
What Does Gonioscopy Reveal?
The iridocorneal angle may be open, narrow, or closed. The last condition should point to both primary and secondary types of angle-closure glaucoma. Similarly, an open-angle should suggest either POAG or other varieties of secondary open-angle glaucomas. A patient with narrow angles may present some difficulty in categorizing and usually needs careful follow-up and evaluation. Finally, fundus examination should help us to narrow in on the ultimate diagnosis.
What Does the Fundus Examination Show?
A thorough evaluation of the optic nerve head includes looking for signs of glaucomatous changes and any differences in the extent of damage between the two eyes. Though asymmetrical cupping is quiet common in POAG, symmetrical damage does not rule out the diagnosis. The final diagnosis should be made taking all pieces of information together.
Treatment and Management
The treatment and management of a patient with POAG poses a great challenge for the physician. Like many other chronic diseases, POAG may cause havoc to the mental, physical, economical, and social well-being of the patient. It is essential, therefore, to mentally prepare the patient while the investigations are progressing. After the diagnosis is confirmed and the initial status of the optic nerve structure and function is documented, it is time to break the news to the patient. Many physicians find it helpful if a family member is also present at the discussions. The physician should emphasize the lifelong commitment to therapy and follow-up. Different therapies, including topical and systemic medications, lasers, and mechanical surgeries, should be explained. An estimate of the target pressure should also be a top priority as the therapy is begun, and henceforth all efforts are focused to maintain IOP at that level or below. The beneficial effect of reduced IOP on progression of glaucomatous damage is well documented.137,138
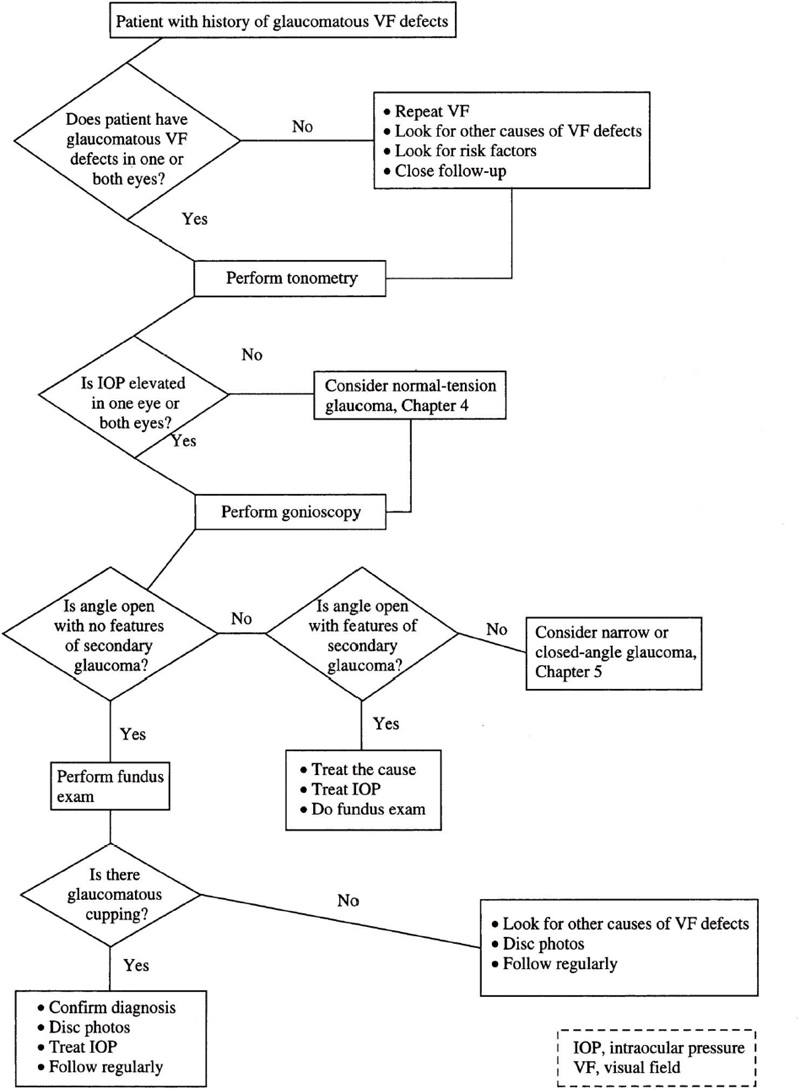
Figure 2–3. Management of a patient who presents with history of glaucomatous visual field defects.
What Is the Initial Therapy of POAG?
This depends on multiple factors such as the height of IOP, extent of disease damage, age, local and systemic contraindications to therapy, social support, and mental status of the patient. If the IOP is very high (e.g., >35 mm Hg) it may be appropriate to begin with more than one medication. Otherwise, it is best to add one medication at a time. In this way, not only the response of therapy but also the dosage and side effects of each drug can be evaluated. To minimize diurnal effects on the IOP, many clinicians advocate monotherapy when considering additional topical therapy.
What Is the Definitive Treatment for POAG?
It may take months before the most appropriate combination of drugs is found. Chapter 18 provides a detailed description of individual drugs used to treat glaucoma, and Chapter 19 discusses various surgical procedures employed in managing the disease. The first agent of choice for most clinicians is still a beta-blocker. Both selective and nonselective agents are available. The chief contraindications are restrictive airway disease, bradycardia, and cardiovascular compromise. For the second position agent, one may choose between a prostaglandin analogue and an α-agonist. Latanoprost is the only prostaglandin analogue available and is very effective in reducing IOP, presumably by increasing uveoscleral outflow. The long-term side effects are still not known. Alphaclonidine and brimonidine are the two α-agonists currently available in the United States, and their long-term use is marred by a high degree of associated allergic conjunctivitis. If two different agents are unable to control IOP, some clinicians may consider argon laser trabeculoplasty next over adding another drug. The main considerations are noncompliance by the patient and the inability to bear the higher cost of medical therapy. For the third-agent spot, there is a choice between a topical and an oral carbonic anhydrase inhibitor (CAI). The two topical CAIs are dorzolamide and brinzolamide. Local allergies for both the agents are a concern for long-term use. Systemic CAIs are acetazolamide and methazolamide; the former also has a parenteral form. Oral therapy is associated with untoward systemic effects such as nausea, weakness, dizziness, insomnia, renal stones and skin rashes. The remaining antiglaucoma drugs are the miotics and epinephrine or its derivatives. Miotics are inexpensive but are associated with side effects such as miosis, ciliary spasm, myopia, and cataract formation, and noncompliance is a problem. Epinephrine-type drugs may cause annoying local irritation, headaches, elevated blood pressure, and cystoid macular edema in aphakes.
Argon laser trabeculoplasty is an effective way of reducing IOP. The advantages include its effectiveness and that it is performed in the office under topical anesthesia only. The availability of apraclonidine has reduced the chances of transient postoperative pressure spikes. The disadvantages are a lack of long-term control and ineffectiveness in young adults.
A number of other surgical procedures are employed for uncontrolled glaucoma, namely trabeculectomy with or without antimetabolites, setons, and various cyclodestructive procedures (see Chapter 19).
What Is a Target Pressure?
Target pressure refers to an arbitrary range of pressure that a treating physician may feel is unlikely to cause further damage to the optic nerve.139 As is obvious from the definition the pressure may vary from patient to patient and even in the same patient over the course of the disease. The minimal pressure that a clinician may try to achieve initially is reduction by 25 to 30%. Later the target pressure depends on variables such as age, race, degree of glaucomatous damage, compliance, and associated systemic ailments. The target pressure therefore, is an ever-changing number that the physician and patient both try to achieve with reasonable means. As a rule of thumb, the greater the damage, the lower the initial target pressure. It is always important to remember that there are factors other than pressure alone that may be responsible for glaucomatous damage.
How Common Is Noncompliance in Patients with Glaucoma?
Patient compliance with medications is an important challenge faced by all physicians. The close relationship between poor patient compliance to either medical or surgical therapy and progressive glaucomatous visual loss is well established.68,140 It is such a complex problem that new noncompliance reasons are being confronted every day. In glaucoma patients some of the well-known reasons for noncompliance are lack of awareness of the severity of the disease, cost of medications, side effects of therapy, and helplessness under deteriorating visual status. Various helpful techniques that may help compliance include patient education, tailor-made topical therapy, family involvement in the management of the disease, support groups, and constant encouragement. The time spent in confronting noncompliance is well spent, as studies have shown that one-third or more patients do not take their medications as prescribed.141,142
What Is the Follow-Up Schedule for Patients with POAG?
The follow-up schedule should be tailor-made for individual patients. Apart from the level of control and severity of glaucomatous damage, other factors that may influence a patient’s follow-up visits include noncompliance and degree of family/ social support. It is essential to inquire about side effects of therapy, measure visual acuity, check IOP, and examine the optic nerve at each visit. Visual field evaluation and gonioscopy should also be done periodically. A patient with uncontrolled IOP and/or deteriorating optic nerve may have to be seen every day or weekly until the condition is stabilized. After adequate control, the visits may be increased to every 1 to 4 months. A compliant, stable patient may need to be seen only two to three times a year. A visual field examination and optic nerve photography/imaging may be performed one to two times yearly.
What Is the Cost of Glaucoma Medications?
Whenever initiating medical therapy or changing medications, it is worthwhile to consider the cost of drugs. This is all the more important because most patients with glaucoma are elderly, on fixed income, and may be taking several other drugs concurrently. Several studies have looked at the question of the cost of glaucoma medications.143,144 In 1999, Fiscella and coworkers145 calculated daily patients cost of glaucoma medications. The costs per day for various drugs were beta-blockers $0.30 to $0.81, brimonidine $0.90, and latanoprost $0.92, respectively.
Is There Any Information Available Regarding Characteristics of Office Visits by Glaucoma Patients?
The data collected by the NAMCS have provided useful sampling information on various aspects of office visits by glaucoma patients.60 In the most recent 2-year survey report of 1991–92, there were 17.5 million visits made by patients who were listed with the principal diagnosis of glaucoma. This translated to an average of 8.7 million visits per year or 3.5 visits per 100 persons per year. The visit rate for persons 75 years of age and over was considerably higher, being 26.8 visits per 100 persons. Moreover, during the same period 3.2 million more visits were by patients with glaucoma as their secondary or tertiary diagnosis. As would be expected, 92.8% of glaucoma visits were made by individuals at least 45 years of age, but over 61.3% of all patients were female. The average visit rate for females was 4.2 visits per 100, whereas for males the rate was 2.8 per 100 persons. Visit rates increased by age in both sexes, but no significant difference was observed for age-specific rates by sex in any age group. Nearly 88% of all visits were made by white patients. The average visit rate for white individuals was 3.7 visits per 100 persons, whereas it was 3.0 visits per 100 black persons. The findings from the NAMCS in 1992 showed that black patients accounted for about 36% of the glaucoma-related visits to the hospital outpatient departments compared to approximately 61% by the white patients. There were some geographical differences in the office visit rates. In the South the visit rate was 4.3 visits per 100 persons compared to 2.1 visits per 100 persons in the West.
General ophthalmologists saw about 76% of glaucoma patients, and the rest were taken care of by glaucoma specialists. Although 68.1% of all new patients were referred by other physicians, only 6.8% of glaucoma patients had such a referral. Even the referral rate for patients with diagnoses other than glaucoma was better—31.6%. Patients making return visits composed 90%, of the total, whereas 10% of visits were by new patients. Approximately 17% of all visits made by subjects in age group of 45 to 64 years were for new problems compared to 9% of those 65 years of age and older. The mean physician–patient contact time during glaucoma visits was 21.7 minutes compared to 17.3 minutes for other office visits.
What Are the Sources of Payments for Office Visits?
For the period 1991–92, payment sources for patient visits were Medicare (61.9%), private insurance (36.6%), self-payment (18.8%), Medicaid (8.0%), Health Maintenance Organization/prepaid (7.1%), other government (4.7%), other (2.9%), no charge (1.2%), and unknown (0.8%).
What Are the Reasons for Patient Visits?
The NAMCS provides detailed information on the reasons for office visits by glaucoma patients during 1991–92. The various reasons, in descending order of frequency, were diagnosis of glaucoma (46.9%), diagnostic screening and preventive measures (27.2%), treatment (9.7%), symptoms (9.4%), other (5.8%), and test results (1.0%). Among patients returning for diagnostic tests, about one-third had one diagnostic test, and approximately half had two diagnostic tests.
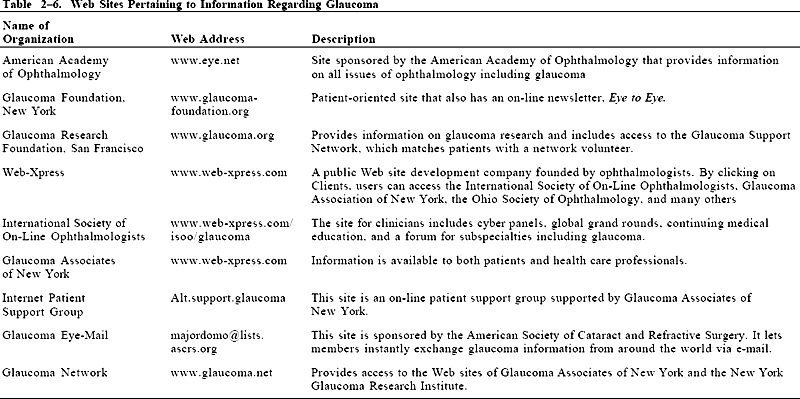
Are There Any Resource Centers for Glaucoma Information?
There are several national and international organizations concerned with the problems associated with glaucoma. Table 2–6 lists Internet Web sites providing a wide range of information concerning glaucoma.
Are There Public Awareness Programs for Glaucoma?
The largest public-awareness program is the glaucoma portion of National Eye Health Education Program (NEHEP), funded by the National Eye Institute in 1991. The National Society to Prevent Blindness (NSPB) has a very active ongoing program schedule such as Glaucoma High-Risk Alert, National Glaucoma Awareness Week, an Eye-Saving Sabbath, a National Center for Sight information clearinghouse, Fight For Sight research awards, an industry safety program, a patient brochure series, implementation of a screening pilot study, and formation of a coalition of African-American organizations. The chief aim of all the programs is to make the public fully aware of the importance of periodic ophthalmologic examinations especially among high-risk groups.
What Type of Counseling Is Required in POAG?
As eyesight is so essential for social and economical health, many glaucoma patients fall into depression, often feeling desperate and helpless. The treating physician should be aware of the signs and symptoms of depression and be willing to provide information and support. The family members can be a great source of information regarding the extent of the problem. Drug-related psychiatric side effects might be resolved by altering medications. The most common offenders are CAIs and beta-blockers. Employers may need letters from the physician explaining the extent of visual disability and other handicaps. For example, the patient may not be able to return to jobs requiring the use of heavy machinery or night shifts. Some patients may benefit from currently available low visual aids. Others may require referrals to glaucoma resource centers, social agencies, and psychiatrists.
What Is the Effect of Glaucoma on the Patient’s Quality of Life?
Visual loss including other social and economical factors may adversely affect a patient’s quality of life. Sherwood and coworkers146 compared the quality of life between patients with glaucoma and a control group. In the former group there was a statistically significant difference in physical functioning, role functioning, social functioning, mental health, and health perceptions. Similarly, they showed statistically significant differences in day vision, night vision, far vision, near vision, glare impact, and overall vision. Patients with glaucoma also complained significantly more of day sleepiness, lack of energy, and eye aches. Increasing glaucoma damage was associated with decreasing quality of life perception. Mobility performance was found to be decreased in individuals with glaucoma as compared to persons with normal vision.147 For instance, the former walked, on the average, 10% slower than the latter. Herbert and associates148 found that compared to white Americans, black Americans tend to rely more on family, immediate community, and religion to cope with the effects of disease on their lives.
Future Considerations
Where Is Glaucoma Research Heading?
There is an acute need for ways to diagnose glaucoma early and to provide neuroprotection to healthy as well as injured ganglion cells. Genetic testing for defective genes opens a new avenue toward early diagnosis and possible therapy. Borrás and associates149 have demonstrated transfer of genes to the trabecular meshwork and expression of recombinant proteins in rabbits after injection of replication-deficient adenovirus vectors into the anterior chamber. Similarly, Kaufman and coworkers150 used a herpes viral vector (ribonucleotide reductase defective HSV-1, hrR31) to deliver the lacZ reporter gene to living cat and rat eyes.
A device that can measure IOP continuously without the patient having to visit a physician would also answer the difficult question of diurnal variation. Accordingly, medical therapy might be altered to address IOP fluctuations during the course of the day.
The field of neuroprotection has opened exciting possibilities. Current research is focusing on determining relevant mechanisms involved in retinal ganglion cell degeneration by studying cellular changes in the optic nerve and retina. The ultimate aim is to prevent retinal ganglion cell loss. Neufeld and associates151 have demonstrated inducible nitric oxide synthase (NOS-2) in the optic nerve heads from human glaucomatous eyes and from rat eyes with chronic, moderately elevated pressure. They treated rats with unilateral elevated pressure with aminoguanidine, an inhibitor of NOS-2 for 6 months and compared that to an untreated group. At the end of the study the untreated group showed pallor and cupping, whereas the treated group appeared normal. When they calculated retinal ganglion cell loss by labeling with Fluoro-Gold, the cell loss in the treated group was 10% compared to 36% in the other group. The investigators believe that excessive nitric oxide released by reactive astrocytes stimulates the production of peroxynitrite, which is toxic to the axons of retinal ganglion cells at the level of lamina cribrosa. This epic finding opens new doors for designing neuroprotective agents in the near future. Drugs that block excitotoxic ganglion cell loss or those that bar NOS, such as arginine analogues, may have a role in the treatment of glaucoma. Memantine, which blocks excessive or pathologic NMDA receptor-linked ion channel activity but relatively spares normal or physiologic activity, is being tried in clinical glaucoma trials in the United States as a potential neuroprotective agent.152,153 It is already used for the treatment of dementia and Parkinson’s disease.
Acknowledgment
This work is supported in part by an unrestricted research grant from Research to Prevent Blindness, Inc., New York, New York.
References
21. Schumer RA, Podos SM: The nerve of glaucoma. Arch Ophthalmol 1994;112:37–44.
23. Quigley HA, Addicks EM, Green WR: Optic nerve damage in human glaucoma: III. Quantitative correlation of nerve fiber loss and visual field defect in glaucoma, ischemic neuropathy, disc edema and toxic neuropathy. Arch Ophthalmol 1982;100:135–146.
35. Leske MC: The epidemiology of open-angle glaucoma: a review. Am J Epidemiol 1983;118:166–191.
36. Quigley HA: Number of people with glaucoma worldwide. Br J Ophthalmol 1996;80:389–393.
37. Thylefors B, Négrel AD: The global impact of glaucoma. Bull WHO 1994;72;323–326.
53. Shiose Y: Method for glaucoma screening in a multicenter collaborative study in Japan. Chibrer Int J Ophthalmol 1990;7:42–48.
62. Hiller R, Kahn HA: Blindness from glaucoma. Am J Ophthalmol 1975;80:62–69.
67. Bengtsson B: The prevalence of glaucoma. Br J Ophthalmol 1981;65:46–54.
84. Hayreh SS: Systemic arterial blood pressure and the eye. Eye 1996;10:5–28.
88. Becker B: Diabetes mellitus and primary open-angle glaucoma. Am J Ophthalmol 1971;71:1–14.
 on G, Zúñiga J, et al: HLA-DRB and HLA-DQB loci in the genetic susceptibility to develop glaucoma in Mexicans. Am J Ophthalmol 1999;128:297–300.
on G, Zúñiga J, et al: HLA-DRB and HLA-DQB loci in the genetic susceptibility to develop glaucoma in Mexicans. Am J Ophthalmol 1999;128:297–300.98. Becker B: The genetic problem of chronic simple glaucoma. Ann Ophthalmol 1971;4:351–354.
100. Biró I: Notes upon the question of hereditary glaucoma. Ophthalmologica1951;122:228–238.
112. Belloc NB: Expectation of life for persons with glaucoma. J Chron Dis 1963;16:163–171.
117. Jonas JB, Papastathopoulos K: Ophthalmoscopic measurement of the optic disc. Ophthalmology 1995;102:1102–1106.
140. Kass MA: Compliance and prognosis in glaucoma. Arch Ophthalmol 1985;103:504–509.
144. Kooner KS, Zimmerman TJ: The cost of antiglaucoma medications. Ann Ophthalmol 1987;19:327–328.
145. Fiscella R: Costs of glaucoma medication. Am J Health Syst Pharm 1998;55:272–275.
148. Herbert A, Burns A, Garcia-Siekavizza, et al: Capturing the uncaptured. An anthropological approach to quality of life prevention in glaucoma patients. Invest Ophthalmol Vis Sci 1996;37 (suppl):36.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


