![]() 14
14 ![]()
Neovascular Glaucoma
Cuong D. Vu and John J. Alappatt
Definition
How Is Neovascular Glaucoma Defined?
Neovascular glaucoma (NVG) is a type of secondary angle glaucoma attributed to new blood vessel formation in the angle. It is the end stage of a variety of ophthalmic disorders whose common feature is widespread retinal hypoxia (Table 14-1).
Epidemiology and Importance
Why Is Prompt Recognition and Treatment of NVG Important?
NVG is a serious complication with significant potential for devastating visual loss. Once in its fulminant stage, the likelihood for successful outcome is markedly reduced. The best visual outcomes occur with prompt recognition of this complication in its earliest stages and proper treatment of the underlying etiology.1
What Are the Demographic Characteristics of Patients Who Develop NVG?
There is no age, gender, race, or ethnic group predilection for the development of NVG. Because close follow-up examination is a key factor in the detection of the early stages of NVG, patient compliance is a major factor.
| Systemic vascular disease Carotid occlusive disease Carotid cavernous fistula Giant cell arteritis Sickle cell disease |
| Ocular vascular disease Diabetic retinopathy Central vein occlusion Central artery occlusion Branch vein occlusion Coats’ disease (retinal telangiectasia) Eales’ disease Retinopathy of prematurity Persistent hyperplastic primary vitreous Anterior segment ischemia |
| Other ocular disease Chronic uveitis Chronic retinal detachment Primary rhegmatogenous Sticklers’ syndrome Retinoschisis Trauma |
| Endophthalmitis |
| Intraocular tumor Uveal melanoma Metastatic carcinoma Retinoblastoma |
| Therapy Radiation treatment Postvitrectomy diabetic eye |
What Are the Biologic Characteristics of Patients Who Have NVG?
There is no particular blood level of antibodies, chemicals, enzymes, or cellular constituents that is diagnostic of NVG. However, patients may demonstrate systemic features consistent with their underlying etiology. Diabetics may be poorly controlled with elevated serum glucose. Patients with carotid occlusive disease often have concomitant heart disease, hypertension, and significant obstruction on carotid Doppler testing. Glaucoma is a risk factor for central retinal vein occlusion (CRVO).
What Are the Social And Economic Factors of Patients Who Have NVG?
Effective prevention and treatment of NVG is dependent on timely diagnosis and management. Thus, social and economic factors predisposing to poor compliance and follow-up must be considered.
What Are the Personal Habits of Patients Who May Develop NVG?
There are no personal habits such as tobacco use, diet, or physical exercise likely to contribute to the development of NVG. A history of noncompliance with medical treatment is a risk factor for late detection of NVG.
What Are the Genetic Characteristics of Patients Who May Develop NVG?
There are no genetic characteristics that favor the development of NVG.
What Are The Major Entities that Lead to NVG?
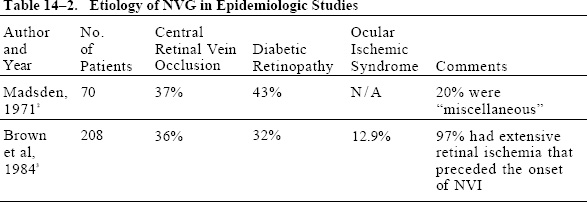
The medical literature contains many possible etiologies to consider in patients with NVG, but diabetes mellitus, CRVO, and ocular ischemic syndrome (OIS) are the primary underlying diseases to consider. There are two large epidemiologic studies on the causes of NVG (Table 14-2). The Madsen2 study reviewed hemorrhagic glaucoma in 70 patients in a Denmark eye facility. The Brown et al3 study is a retrospective review of 208 patients with NVG in a major urban eye hospital.
What Is the Pathogenesis of NVG?
NVG is a complication thought to be secondary to angiogenic factors produced by the ischemic retina that enter the anterior chamber.1 Various substances have been suggested as the underlying common agent. Of note, vascular endothelial growth factor (VEGF) has been shown to induce a noninflammatory iris neovascularization in nonhuman primate eyes when injected at a concentration comparable to that found in human eyes with neovascular glaucoma.4 There is evidence that the angiogenic factor originates from the posterior segment of the eye. NVG has been observed following noncomplicated laser posterior capsulotomy, which presumably permitted angiogenic factors access to the anterior chamber.5 Additionally, neovascularization of the iris (NVI) has been observed to begin at the peripheral iridotomy site in a patient with iris bombé.6
Diagnosis and Differential Diagnosis
How Is NVG Diagnosed?
In the classic presentation of fulminant NVG, patients complain of pain, photophobia, and decreased vision. Visual acuity is typically in the hand motion to counting fingers range. The secondary closed angle results in extremely high intraocular pressure (IOP), producing conjunctival injection, steamy cornea, and inflammation. Slit-lamp examination demonstrates NVI and ectropion uvea (a flattened iris anterior face and rotation of the iris pigment epithelium anteriorly). Gonioscopy reveals angle closure, with the inferior portion being the last to seal off. Fundus examination often shows an ischemic retina and thus the underlying disorder.
There may be great variability in clinical presentation in each individual case of NVG. For example, IOP may be normal or reduced in NVG secondary to OIS.
How Is NVI Differentiated from Normal Iris Vasculature?
Abnormal iris vessels have characteristic features that differentiate them from normal iris vessels. Normal iris vessels have a nonarborized intrastromal orientation. Iris neovascularization first appears as buds of vessels, resembling glomeruli. These buds are typically detected first at the pupillary margin. Later stages of NVI show a fine net of blood vessels in an extrastromal location. NVI typically demonstrates angiographic leakage, whereas normal iris vessels do not leak. Any blood vessels that cross the sclera spur are considered abnormal. Later stages lead to arborization into the trabecular meshwork, giving the meshwork a red appearance. It may be difficult to differentiate engorged iris vessels in an inflamed eye from NVI.
How Does the Neovascularization of the Angle Lead to Angle Closure?
Posterior segment hypoxia leads to the production of angiogenic factors that circulate into the anterior segment, stimulating the growth of new blood vessels, usually first at the pupillary margin. It is classically thought that neovascularization of the angle (NVA) does not occur without accompanying NVI, though there are anecdotal accounts that dispute this claim. For example, gonioscopy may detect NVA prior to the detection of NVI.7
Pathologic studies have confirmed the presence of an accompanying “invisible” fibrovascular membrane in cases of NVG. Contraction of this fibrovascular membrane leads to points of synechial angle closure. Coalescence of these points of synechial closure ultimately leads to total angle closure and thus dramatic reduction of trabecular outflow. The progression of NVI to NVA to NVG may occur over days, weeks, months, or years.
| Disease | Characteristic Features |
| Fuchs’ heterochromic iridocyclitis | White, quiet eyes Fine, fragile blood vessels may cross scleral spur Synechiae do not develop No associated retinal ischemia |
| Pseudoexfoliation glaucoma | Target lesion on anterior capsule No associated retinal ischemia |
| Uveitis | No associated retinal ischemia Iris vascularization regresses with steroid treatment No NVA |
What Is the Differential Diagnosis of NVG?
In its early stages, NVG must be differentiated from other disorders with prominent iris blood vessels. There are a number of historical and clinical features that may facilitate this distinction (Table 14-3).
In the fulminant stage, the main differential diagnosis to be considered is acute primary angle closure because it shares with NVG the common features of poor vision, extreme pain, high IOP, congested conjunctiva, and steamy cornea. If examination of the fellow eye also reveals a narrow occludable angle, then a diagnosis of primary angle closure is more likely. Also, pressure on gonioscopy (compression gonioscopy) may force the angle open. In NVG, the angle is sealed and cannot be forced open. Funduscopic exam in NVG is consistent with a hypoxic posterior segment.
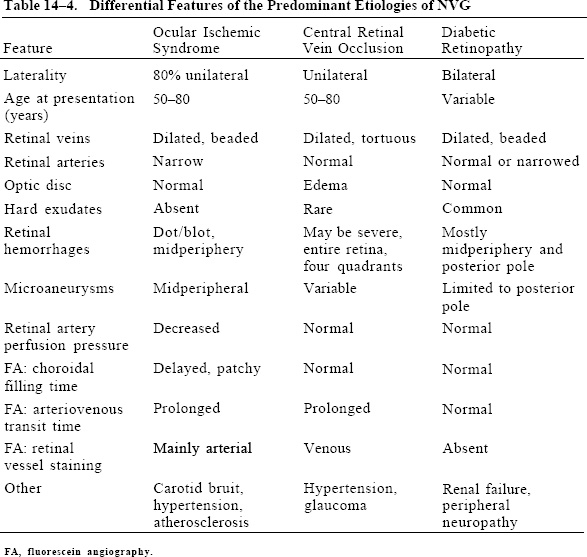
What Are the Key Distinguishing Features of the Main Causes of NVG?
This chapter discusses differentiating between the most likely entities in patients with NVG (Table 14-4). Chapter 11 discusses the primary etiologies of central retinal vein occlusion, diabetes mellitus, and OIS.
Treatment and Management
What Are the General Principles to Consider in Preventing Progression to NVG?
It is crucial to maintain a high clinical suspicion for the potential of the currently managed disease to progress to this complication (Fig. 14–1). Prompt recognition of iris neovascularization is critical to successful management. This is best achieved with standardized high-magnification nondilated examination of the iris, with particular attention to the pupillary margin.
When NVI is detected, determine and treat the underlying cause of posterior segment hypoxia. If examination reveals a fundus without definite hypoxia, always consider the diagnosis of OIS. The goal is to reduce posterior segment hypoxia and thus regress the NVI and NVA before it reaches fulminant NVG.
What Are the Techniques Used to Prevent Progression to NVG?
Panretinal photocoagulation is the preferred means of decreasing posterior segment hypoxia, but it is limited because successful treatment is largely dependent on clear media. Topical glycerin may be used to decrease corneal edema so that one may achieve sufficient improved view for effective treatment. The goal of treatment is to ablate the ischemic retina. Insufficient treatment will not adequately reduce the hypoxic drive to NVG progression. The effectiveness of panretinal photocoagulation in NVI and NVG has been well documented.8,9
Panretinal cryotherapy may be useful in cases where the cornea, lens, or vitreous is too hazy to get adequate laser treatment. The disadvantage of this technique is that it promotes significant breakdown of the blood–retina barrier, stimulating inflammation.
Goniophotocoagulation is a laser treatment directly applied to the iris and angle to reduce NVI and NVA. The effectiveness of this technique is not established. The only documented cases of successful goniophotocoagulation have been performed in conjunction with panretinal photocoagulation.10 In fact, goniophotocoagulation may precipitate inflammation and hasten synechial angle closure.
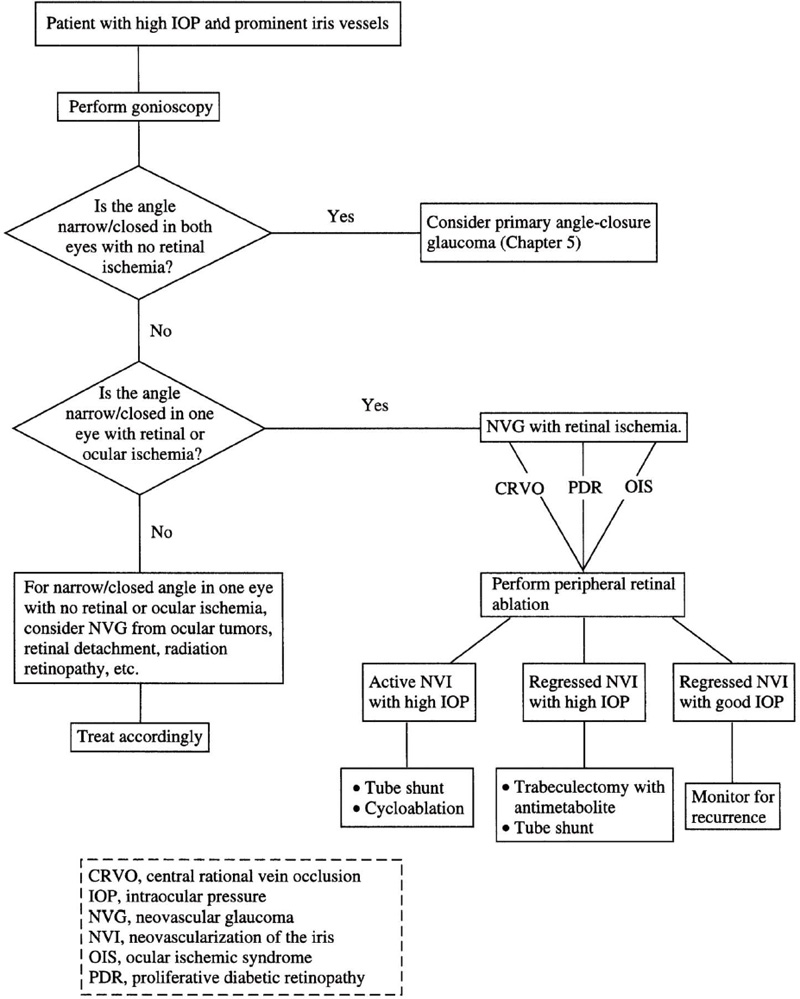
Figure 14–1. Algorithm for managing a patient with NVG.
How Is a Patient with Diabetic Retinopathy Prevented from Progressing to NVG?
Prompt panretinal photocoagulation should be employed when high-risk proliferative features are found in diabetic eyes. The Diabetic Retinopathy Study demonstrated that vitreous hemorrhage, disc neovascularization, and new areas of retinal neovascularization are ominous features of proliferative diabetic retinopathy.11
Particular caution should be employed in diabetic patients who are status post-cataract surgery or postvitrectomy, as they may quickly progress to fulminant NVG. It is thought that preservation of the posterior capsule during cataract surgery minimizes the risk of worsening retinopathy. The incidence of NVG complicating vitrectomy has been decreasing, presumably due to better equipment and endolaser treatment.12 Systemic features such as hypertension and renal failure are often found concomitantly in diabetics who progress to NVG.
How Is a Patient with Newly Diagnosed CRVO Prevented from Progressing to NVG?
Important data regarding the history of treated and untreated CRVO have been reported by the CRVO study group.13 Particular observations to consider include:
- One-third of initially perfused CRVO may progress to ischemia over 3 years.
- Initially nonperfused CRVO is at 35% risk of developing NVI/NVA.
- Panretinal photocoagulation should commence when NVI/NVA develops.
Differentiating between ischemic and nonischemic status may be difficult secondary to retinal obscuration by retinal hemorrhage. Poor visual acuity, presence of an afferent pupillary defect, and decreased electroretinogram values have also been reported to be predictive of progression to neovascular disease.14 Recommended follow-up schedules may be guided by visual acuity at presentation, as per the guidelines of CRVO study group’s report:
- 20/40 or better: every 1 to 2 months for the first 6 months;
- 20/50 or worse: every month for the first 6 months;
- worsening visual acuity: an ominous sign of progression to ischemic status.
Undilated gonioscopy should be done at each follow-up exam because NVA may develop prior to NVI.7
How Is a Patient with OIS Prevented from Progressing to NVG?
Always consider this diagnosis in cases when the funduscopic exam does not show profound clinical evidence of retinal ischemia or when panretinal photocoagulation does not regress NVI/NVA. Some studies report that only a third of these patients have elevated IOP.1 This decrease in aqueous production is thought to be due to hypoperfusion of the ciliary body. Panretinal photocoagulation should be the first step, though it may not be effective, because OIS also gives rise to anterior segment ischemia late in its course.15 Once surgical revascularization of the carotid occurs, it may lead to an increase in IOP and worsened ophthalmic vessel disease. Internal medicine or cardiology services should be consulted in these patients to rule out carotid disease and concomitant cardiovascular disease.
The Underlying Cause of the NVG Was Diagnosed and Treated and the IOP Is Now Within Normal Limits. What is Next?
Close monitoring and observation are essential because this condition may recur at any time.
What Treatment Options Are Available If the IOP Is Still Elevated Following Complete Treatment of the Underlying Cause of NVG?
The IOP may still be elevated because despite inducing the NVI/NVA to quiescence, the angle is still zipped shut and a permanent angle closure status is maintained. Medical therapy is the preferred means of controlling IOP at this point.
Ocular pressure reduction medications may also be used to obtain a clearer view for diagnostic and treatment purposes. The aim is to maintain acceptable IOP. Avoid pilocarpine and other cholinergics, because they may break down the blood vessel barrier and facilitate increased inflammation. Topical corticosteroids are helpful in reducing inflammation and may be used as indicated.
What Treatment Options Are Available If, Despite Maximally Tolerated Antiglaucoma Medications, the IOP Is Still Elevated?
NVG typically responds poorly to conventional glaucoma surgery. These poor outcomes have prompted a variety of different interventions strategies. The main approaches used are trabeculectomy with antimetabolites, tube-shunt surgery, cyclocryotherapy, and cyclophotocoagulation. In an eye with quiescent neovascularization, trabeculectomy with antimetabolites is considered by many to be the primary option. If there are active vessels present, tube-shunt versus ciliary body ablation is considered (see Chapter 19).
What Are the Data Regarding Success Utilizing Trabeculectomy?
Trabeculectomy without metabolite and without concomitant retinal ablation has a low rate of NVG regression (10–30%), whereas, with panretinal photocoagulation as a preoperative adjunct, a 67% success rate has been reported at 12-month follow-up.16
What Is the Long-Term Success of Trabeculectomy with 5-Fluorouracil (5-FU)?
A retrospective case study of 34 NVG eyes treated with 5-FU and trabeculectomy showed adequate IOP control decreased over time. At 1-year follow-up, 70% were controlled, whereas at 5 years the control rate was only 28%.17 Risk factors identified with poor prognosis in this study included insulin-dependent diabetes mellitus and age younger than 50 years.
What Are the Success Rates of Utilizing Tube-Shunt Surgery for NVG?
The single-plate Molteno has been documented with a satisfactory IOP control rate of about 60% at 1 year and 10% at 5 years.18 Another retrospective study showed that the Baerveldt implant yielded 79% success at 12 months but only 56% after 18 months.19 In both of these studies, success was defined as a final IOP of 6 to 21 mm Hg without the need for additional surgery and without devastating complication.
What Is More Effective in the Management of NVG, Tube-Shunt Surgery or Neodymium:Yttrium-Aluminum-Garnet (Nd:YAG) Cyclophotocoagulation?
In a retrospective case-matched comparative study of 49 patients, satisfactory IOP control was achieved in 66% of tube shunted patients versus 38% of cyclophotocoagulated patients.20
Future Considerations
What Are the Future Considerations in Managing NVG?
Transscleral diode cyclophotocoagulation has emerged as an effective means of lowering IOP in refractory glaucoma. There have been reports of success utilizing diode cyclo and retinal ablation in cases where the view is compromised.21 Threlkeld et al22 noted that diode cyclophotocoagulation for eyes with NVG appeared to have a higher risk of hypotony. Only limited case series are currently available for this technique. There has been a recent report that interleukin-6 is present in the aqueous humor of patients with NVG secondary to CRVO.23 Future modification of the inflammatory factors seen in NVG may provide a new means of imaging NVG.
Acknowledgment
This work is supported in part by an unrestricted research grant from Research to Prevent Blindness, Inc., New York, New York.
References
23. Chen KH, Wu CC, Roy S, et al: Increased interkeukin-6 in aqueous humor of neovascular glaucoma. Invest Ophthalmol Vis Sci 1999;40:2627–2632.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


