Chapter 77 Intermittent exotropia
Definition
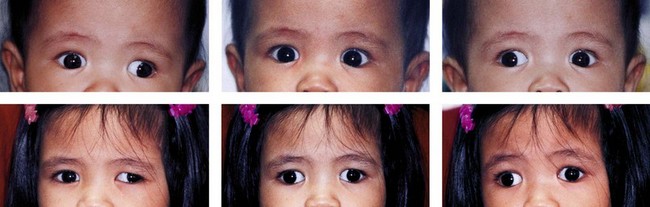
Intermittent exotropia (X(T)) is a strabismus condition with outward drifting of either eye interspersed with periods of good alignment or orthotropia (Fig. 77.1). Monocular eye closure may occur during exodeviation. Near stereoacuity is often normal during periods of alignment, though it may deteriorate if the condition progresses.
Cause
1. An imbalance between active convergence and divergence,1 although it is not clear that divergence is active.2
3. Abnormalities of extraocular muscle proprioception,4 although the existence of active proprioceptors in extraocular muscles is disputed.5
Epidemiology
X(T) is the most common form of divergent strabismus.6,7 As divergent strabismus is much more common than convergent strabismus in Asia, it is now the most common form of strabismus worldwide.8 The prevalence of exotropia in children less than 11 years of age was estimated as 1%.9 X(T) accounted for approximately half of all cases of exotropia.6 In Singaporean children aged between 6 and 72 months, the prevalence of strabismus was 0.8%, with an exotropia : esotropia ratio of 7 : 1. Sixty-three percent of cases of exotropia were intermittent.10 In Japanese elementary school children, the incidence of X(T) was estimated as 0.12%11 with a slight female predominance.12
Clinical features
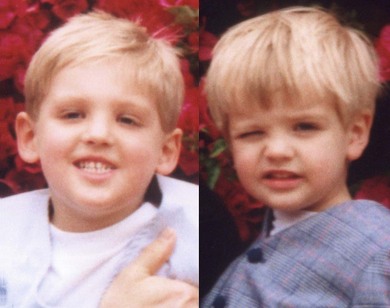
The onset is typically in the second to third year of life,13,14 when an intermittent outward drift of one eye or monocular eye closure in bright sunlight is noted (Fig. 77.2). Monocular eye closure in X(T) has been attributed to photophobia,15 although it is difficult to explain why more light should enter exotropic than orthotropic eyes. Monocular eye closure may be due to diplopia or an abnormal visual percept, or reduction in threshold for bright lights, induced by divergence of the eyes.16,17 It may resolve following surgery.18
It is usually not possible to accurately measure stereoacuity at presentation because the children are too young, but older children with X(T) have normal, or near normal (for age), near stereoacuity.14 One study found reduced visual acuity in one or both eyes of 26% of children at presentation, although this reduction was generally just below age-related normal thresholds and due to anisometropia.14
X(T) is traditionally classified into three types:
1. True divergence excess: the deviation is more than 10 prism diopters (PD) larger when measured at distance fixation than at near.
2. Simulated divergence excess: initially greater at distance fixation, but the misalignment at near fixation increases to within 10 diopters of the angle at distance following disruption of near binocular vision by monocular occlusion.
3. Basic: the size of the misalignment is equal, to within 10 PD, whether the misalignment is measured at distance or near fixation.19,20
The distinction between the types is important in determining the appropriate surgical treatment,21 although this has been disputed.22 The measurements required may be difficult in young children.
One of the most striking neurophysiologic features of X(T) is that children with the condition alternate between a state of apparently normal (or near normal) binocular vision, with normal stereoacuity when the eyes are aligned and a state of suppression, or anomalous retinal correspondence, when the eyes are divergent.23–25 However, binocular function is not entirely normal during ocular alignment in X(T); children with X(T) have reduced positive fusional vergences (reduced convergence in response to a base-out prism).26 Furthermore, suppression can be demonstrated even during periods of normal ocular alignment, indicating that it can be triggered by purely retinal information.27
A subset of children with X(T) have subnormal binocular function even during periods of ocular “alignment” because the “alignment” is actually a small constant divergent misalignment.28 This may underlie the lack of normal stereoacuity seen following treatment of X(T) in some cases.29
While X(T) is not associated with neurodevelopmental abnormalities, it has been associated with the subsequent development of psychiatric disorders.30,31 The reason for this is unknown, but it is unlikely to be due to the consequences of an abnormal appearance in childhood, as it is not seen in children with esotropia.30
Quality of life in intermittent exotropia
The Pediatric Quality of Life Inventory has been used to investigate quality of life in X(T) without significant effects being observed.32 Hatt et al.33 developed a specific quality of life measure based on interviews with children with X(T). They identified concerns about the presence of exotropia, particularly relating to awareness of exotropia by observers, but also awareness on the part of the child of strategies to control exotropia, such as blinking. They also identified parental anxiety about exotropia as the most significant concern.34
Clinical evaluation
Possible measures of progression or outcome in X(T) are:
• Angle (size) of misalignment.
• Stereoacuity (for near and/or distance fixation).
• Deterioration of convergence.
• Deterioration to constant exotropia (+/− development of strabismic amblyopia).
Accurate measurements of stereoacuity and convergence are not consistent in children under the age of 4 years, and control, constancy, and angle (particularly at distance) are also challenging to measure in this group. Any therapy for children under the age of 4 years with X(T) is necessarily based on imperfect clinical measurements, making assessment of the effect of therapy difficult. Thus, many clinicians defer treatment until later, despite the theoretical benefits of early therapy.14
The traditional outcome measure for the effect of therapy on X(T) is the size of the angle of the misalignment, with successful outcomes following therapy often taken as angles of between +/− 10 PD of orthophoria.35–38
Ocular alignment (usually with a range of +/−10 PD), is, however, an inadequate outcome measure for treatment of X(T). The measurement given usually includes latent and manifest (tropia and phoria) components of the misalignment. Thus small constant misalignments, both esotropic and exotropic, with worse functional correlates than X(T)s, are included as treatment “successes.”38
Assessing the control of intermittent exotropia
A more relevant measure of treatment of X(T) is the degree of control of the misalignment, as measured by the frequency with which a strabismus is manifest, and the ease with which an induced misalignment can be realigned. Diplopia is not a feature of X(T), and the mechanisms underlying control are obscure, but some children report awareness of their misalignment.33
Two scoring systems for the measurement of control of X(T) are in common usage: the Mayo office based scale,39 and the Newcastle Control Score.40,41
The Mayo scoring system is outlined in Table 77.1. The Mayo Scale is based solely on timed observations.
Table 77.1 The Mayo scale for scoring control in X(T)39
Notes:
The score is measured at distance and near fixation, and so yields an overall control score ranging from 0 to 10.
Levels 5 to 3 are assessed during an initial 30-second period of observation at distance fixation and repeated at near fixation for another 30-second period.
Levels 2 to 0 are then graded as the worst of three rapidly successive trials; an occluder is placed over the right eye for 10 seconds and then removed, measuring the length of time it takes for fusion to be re-established. The left eye is then occluded for 10 seconds and the time to re-establish fusion is similarly measured.
A third trial of 10-second occlusion is performed, covering the eye that required the longest time to re-fuse.
The worst level of control observed following the three 10-second periods of occlusion should be recorded.
If the patient has a microesotropia by simultaneous prism and cover test, but exodeviation by alternate cover test, the scale applies to the exodeviation.
The second scoring system is the Newcastle Control Score for Intermittent Exotropia (NCS).41 The criteria for assigning an NCS are given in Table 77.2. The NCS is based on the criteria for surgical intervention popularized by Rosenbaum.42 These criteria consist of a parental report of the frequency with which a divergent misalignment of the eyes is observed (home control) and an objective assessment of the ease with which the eyes can be realigned following the induction of strabismus with a cover test (office control). Rosenbaum suggested that surgery should be considered if the strabismus was present more than 50% of the time and was poorly controlled on examination. The relationship between these two criteria requires further study, but correlations have been shown between home and office control.43
Table 77.2 The Revised Newcastle Control Score for Intermittent Exotropia41
| NCS criteria | Score |
|---|---|
| Home control (XT or monocular eye closure seen) | |
| Never | 0 |
| < 50% of time fixing in distance | 1 |
| > 50% of time fixing in distance | 2 |
| > 50% of time fixing in distance + seen at near | 3 |
| Clinic control (scored for near and distance fixation) | |
| Immediate realignment after dissociation | 0 |
| Realignment with aid of blink or re-fixation | 1 |
| Remains manifest after dissociation/prolonged fixation | 2 |
| Manifest spontaneously | 3 |
| Total score: n/9 |
One study using the Mayo control score showed that control varied over time, which limits its value as an outcome measure.44 Variability has not been demonstrated with the Newcastle score, but the office control component is likely to behave in the same way. The home control element is potentially subject to observer bias but does have the merit of being a parent-reported outcome measure.
Stereoacuity in intermittent exotropia
In X(T), the eyes usually remain aligned for near fixation, or are capable of realignment in response to the stimulus of presentation of a stereoscopic image. Values of near stereoacuity in X(T) are within age-related norms,45–47 making near stereoacuity a poor measure of severity. Near stereoacuity may be lost completely if X(T) deteriorates to a constant exotropia, although, in some cases, restoration of near stereoacuity can be achieved with surgery.48
The initial abnormality in X(T) is binocular misalignment at distance fixation. Measurement of stereoacuity at distance fixation is, therefore, a potential measure of X(T) severity. The tendency to diverge at larger viewing distances may introduce a “pedestal disparity” between the reference surface and the fixation point, thus lowering stereoacuity.25
Measurement of stereoacuity at distance fixation is technically challenging. Previous studies (Binocular Visual Acuity Test)49 used a liquid crystal system requiring goggles during measurement, limiting its use in young children. It is no longer available. Subsequent studies have utilized the Frisby Davis Distance Stereotest50 and the Distance Randot Test.51
Variable results have been reported of the effect of X(T) on distance stereoacuity, depending on the characteristics of the test used. Distance stereoacuity has been reported as normal or absent.52
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


