Degenerative Diseases of the Peripheral Retina
Paul Baker
Chirag P. Shah
William Tasman
ACKNOWLEDGEMENTS
The authors and editors wish to acknowledge the contributions of Robert S. Engstrom, Jr., Ben J. Glasgow, Robert S. Foos, and Bradley R. Strautsma, authors of the previous edition of this chapter. Portions of the text and illustrations are included in this revision.
The peripheral retina may be defined as the anterior portion of the retina that begins 3 mm posterior to the equator of the eye and extends anteriorly to the ora serrata. The equator is where the conspicuous vortex veins pass from the choroid into the sclera. This important segment of the retina may be readily visualized with the techniques of ophthalmoscopy, biomicroscopy, and scleral depression. The physician’s observations are recorded on an ocular fundus chart (Fig. 26-1) using a standardized color code (Table 26-1).
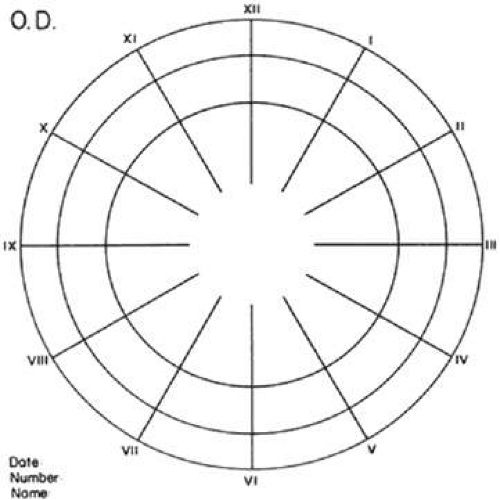 Figure 26-1. Ocular fundus chart. Inner circle represents equator of eye; middle circle represents ora serrata; outer circle represents anterior border of pars plana ciliaris. Radiating lines represent meridians numbered according to clock hours. (Reproduced with permission from Straatsma BR, Foos RY, Spencer LM: The retina: Topography and clinical correlations. In Transactions of the New Orleans Academy of Ophthalmology: Symposium on Retina and Retinal Surgery. St Louis, MO: Mosby, 1969.) |
 |
Examining the peripheral retina and recording the findings requires knowledge of normal topography, anatomic relationships, common developmental variations, significant degenerations, and the manifestations of specific disease entities.
TOPOGRAPHY AND RELATIONSHIPS
The average dimensions of the adult retina from the equator to the ora serrata are 5.07 ± 1.11 mm in the superior meridian, 4.79 ± 1.22 mm inferiorly, 5.81 ± 1.12 mm nasally, and 6.00 ± 1.22 mm temporally. From the ora serrata to the Schwalbe line, which constitutes the posterior border of the limbus, the distance is 6.14 ± 0.85 mm superiorly, 6.20 ± 0.76 mm inferiorly, 5.73 ± 0.81 mm nasally, and 6.53 ± 0.75 mm temporally (Fig. 26-2).1,2
 Figure 26-2. Peripheral retinal topography. Relationship of ora serrata to equator and to the Schwalbe line in the four principal meridians. Average measurements and standard deviations given in millimeters. |
At the equator, the retina has an average diameter of 24.08 ± 0.94 mm in the vertical meridian and 24.03 ± 1.04 mm in the horizontal meridian. From the equator to the ora serrata, the retina diminishes in size so that the average retinal diameter at the ora serrata is 20.41 ±1.09 mm vertically and 20.03 ± 1.04 mm horizontally (Fig. 26-3). Thus, the retina has the shape of a cup that is expanded to its greatest diameter at the equator and is considerably reduced in diameter at its serrated anterior margin.
 Figure 26-3. Retinal shape resembles a cup expanded to its greatest diameter at the equator and reduced in diameter at the ora serrata. Measurements and standard deviations given in millimeters. |
Since the retina is considerably smaller in diameter and circumference at the ora serrata than at the equator (Fig. 26-3), conventional charts of the ocular fundus, which depict the ora serrata as having a diameter and circumference greater than that of the equator, are misleading (Fig. 26-1). These charts should be considered only as diagrammatic projections in which the retina anterior to the equator is disproportionately expanded. In another words, features of the peripheral retina are actually closer together than they appear in the conventional fundus diagram.
Precise measurements of the optic disc diameter and the disc-to-fovea distance are also essential for correlation of topographic and clinical information. In the adult eye, the optic disc has an average vertical diameter of 1.86 ± 0.21 mm and an average horizontal diameter of 1.75 ± 0.19 mm. The center of the fovea is located an average distance of 3.42 ± 0.34 mm temporal and slightly inferior to the temporal margin of the optic disc (Fig. 26-4). Insofar as the disc diameter (approximately 1.75 mm) is the standard for comparison in clinical examination of the retina, the distance from the equator to the ora serrata is approximately three disc diameters.
 Figure 26-4. Dimensions of optic disc and relationship between disc and center of the fovea. Average dimensions and standard deviations given in millimeters. (Reproduced with permission from Straatsma BR, Foos RY, Spencer LM: The retina: Topography and clinical correlations. In Transactions of the New Orleans Academy of Ophthalmology: Symposium on Retina and Retinal Surgery. St Louis: Mosby, 1969.) |
The posterior margin of the peripheral retina is a line joining the points at which the vortex veins pass from the choroid to the sclera.3 This rather constant landmark is 3 mm (nearly two disc diameters) posterior to the equator of the eye.
The anterior edge of the peripheral retina is the ora serrata, an irregularly scalloped border; the irregularities are more pronounced nasally than temporally and have extreme individual variations in contour (Fig. 26-5). Dentate or toothlike processes extend anteriorly from the main contour of this border, and bays or indentations extend posteriorly from the main contour of the ora serrata. At the ora serrata, those projections of the retina toward the vitreous body are termed meridional folds. There is a concentration of dentate processes, ora bays, and meridional folds in the superior nasal quadrant and a progressive decrease in these morphologic features in the inferior nasal, superior temporal, and inferior temporal quadrants (Figs. 26-6 and 26-7). Although individual variations in ora serrata contour may be extreme, studies of adult human eyes demonstrate that both of a patient’s eyes are remarkably similar. The “average” ora serrata has 16 dentate processes, 1 large or giant dentate process, 10 ora bays, and 1 double ora bay.1,2 In clinical practice, morphologic variations in the contour of the ora serrata are most common in the superior nasal quadrant, least common in the inferior temporal quadrant, and subject to a wide range of individual irregularities.
 Figure 26-5. Composite scale drawing depicts peripheral retina, ora serrata, ciliary body, and lens as viewed from posterior aspect. Ora serrata have more dentate processes and ora bays in the nasal quadrants than in the temporal quadrants |
 Figure 26-6. Peripheral fundus showing pre-equatorial retina, ora serrata, and inner surface of ciliary body (smooth portion, pars plana; portion with ciliary processes, pars plicata). Ora serrata in this nasal sector shows largely short dentate processes that are typical; that is, they align with valleys between ciliary processes. On right, a giant dentate process is atypical; that is, it aligns with a ciliary process. |
 Figure 26-7. Dentate process, coronal section. Dentate process shows nonspecific degeneration (including microcystic change) and a cap of dense-staining glial cells on its central surface. Adjacent ciliary epithelium and photoreceptor cells underlying dentate process are largely unremarkable. (Hematoxylin-eosin; ×250.) |
Coursing through the peripheral retina are arterioles and venules that travel separately and are evenly distributed. Arterioles are smaller in caliber and lighter in color than venules; however, to clinically distinguish the arterioles and venules it is usually necessary to trace the vessels posteriorly to an area where accurate differentiation is possible. As vessels extend anteriorly in the peripheral retina their size decreases; they occasionally may travel nearly parallel to the ora serrata and usually become invisible approximately 2 mm posterior to the ora serrata.
Externally, the retina is in contact with the retinal pigment epithelium. Separation of the weak bond between the sensory retina and the retinal pigment epithelium is termed retinal detachment. Internally, the retina contacts the vitreous body. This transparent, gel-like tissue fills two thirds of the globe, has a volume of 4 to 5 mL in adults, and is in contact with the optic disc, ciliary body, zonule, and lens. Although there is some adherence with each of these structures in the normal eye of the young adult, the vitreous is joined most firmly with structures at the vitreous base, a circular band extending anteriorly and posteriorly from the ora serrata. This attachment is firmer temporally than nasally.
In adult eyes studied at autopsy, the anterior vitreous base usually conformed to the contour of the ora serrata and measured 0.26 ± 0.16 mm in the nasal horizontal meridian and 1.32 ± 0.29 mm in the temporal horizontal meridian.1,2
The posterior portion of the vitreous base is the zone of strong vitreoretinal attachment that extends posterior to the ora serrata. In postmortem studies of adult eyes, the posterior vitreous base presented a relatively smooth posterior border; it measured 3.03 ± 0.84 mm in the nasal horizontal meridian and 1.81 ± 0.64 mm in the temporal horizontal meridian.4
The vitreous base is a major factor in the localization and clinical course of developmental variations, degenerations, and diseases. It involves the full circumference of the peripheral fundus, measures approximately 3.2 mm (nearly two disc diameters) anteroposteriorly, generally reflects the anterior contour of the ora serrata, presents a relatively smooth posterior border, extends onto the peripheral retina for a greater distance nasally than temporally, and usually is associated with visibly increased pigmentation in the corresponding portion of the retinal and ciliary body pigment epithelium.
These findings are characteristic of the peripheral retina and adjacent structures in the normal eye of the young adult; the peripheral retina undergoes changes throughout life. The peripheral retina in an infant has brilliant surface light reflexes and becomes increasingly white and translucent near the ora serrata. This translucency and some retinal redundancy in the infant accentuate the abrupt anterior termination of the retina at the ora serrata. However, the Lange fold, a detachment of the retina immediately posterior to the ora serrata, is a laboratory artifact seen during postmortem examination and in surgically enucleated eyes of infants as a result of the extremely strong vitreoretinal attachments in the posterior portion of the vitreous base. Anterior to the ora serrata, the pars plana is underdeveloped in infants; therefore, the ciliary processes are relatively close to the ora serrata.
The peripheral retina becomes fully developed early in life. As the eye reaches full size by age 6 or 7 years, the peripheral retina, ora serrata, and pars plana assume adult characteristics.
During the aging process, there is progressive loss of the light reflex observed on the peripheral retinal surface following young adulthood. The peripheral retina invariably develops specific forms of degeneration; the retinal pigment epithelium becomes progressively more granular, and the adjacent vitreous body develops degenerative changes.
DEVELOPMENTAL VARIATIONS
Several developmental variations of the peripheral retina, defined as localized topographic and structural deviations related to ocular development, are superimposed on the normal topography, structure, and relationships.
MERIDIONAL FOLD
A meridional fold is a radially oriented, ridgelike elevation on the peripheral retina that projects into the vitreous. It is aligned with a dentate process or with the middle of an ora bay, originates at the ora serrata, and extends posteriorly for 0.6 to 6 mm. The surface of the fold is slightly irregular; the thickened retina contains irregular cystoid degeneration (Fig. 26-8).
 Figure 26-8. Meridional fold in a young patient. Retina is thickened along course of fold, which shows microcystoid change near the surface and a cap of dense-staining glial cells along its surface. Middle and outer layers of the retina are largely unremarkable. Pigment epithelium shows focal redundancy anteriorly. (Hematoxylin-eosin; ×150.) |
Meridional folds are present in 26% of the population and are bilateral in 55% of affected patients; thus, they are present in 20% of all eyes (Table 26-2). Meridional folds are multiple in 27% of affected eyes; they are most common in the superior nasal quadrant.5,6
 |
MERIDIONAL COMPLEX
A meridional complex is the occurrence of a dentate process and a ciliary process within the same meridian. When this abnormal alignment occurs, the dentate process is exceptionally large, is usually combined with a meridional fold, and is continuous with an enlarged ciliary process. It is often associated with peripheral retinal excavation in the corresponding meridian (Fig. 26-9). The large dentate process and meridional fold are composed of excessive, disorganized, somewhat degenerated retinal tissue (Fig. 26-10).
 Figure 26-9. Meridional complex (arrow). Note its basic constituent, an atypical dentate process, which aligns with and extends to an enlarged ciliary process. Complex also has a meridional fold that extends along the dentate process and posteriorly into the peripheral retina. |
 Figure 26-10. Microsection of meridional complex through atypical dentate process and its meridional fold. Anteriorly (on the left) the complex shows marked redundancy of pigmented epithelium in its outer aspect and a dense glial plaque on its inner aspect. Posteriorly (on the right) there is microcystoid change, nonspecific degeneration, and dense-staining glial cells along its surface. (Hematoxylin-eosin; ×63.) |
Meridional complexes are present in 16% of the population, are bilateral in 58% of affected patients, and thus are present in 12% of all eyes (Table 26-2). The complexes are multiple in 45% of the affected eyes; they are most common in the superior nasal quadrant.
PARS PLANA CYST
Cysts of pars plana are another variant of the peripheral fundus. They are clear cystoid spaces located between the pigmented and nonpigmented epithelium located just anterior to the ora serrata (Fig. 26-11). They typically lie between pars plana radiations and have the appearance of clear, half-inflated balloons. The overlying vitreous and the surrounding ciliary pigment epithelium are unchanged.6
 Figure 26-11. Three pars plana cysts just anterior to ora serrata. |
ORA SERRATA PEARLS
Another peripheral fundus variant, the ora serrata pearl, is a glistening opacity that typically lies over an oral tooth. It is a drusen-like structure that shows staining qualities of an acid carbohydrate on pathologic examination. It varies in size from a pinpoint to a pinhead. The incidence of these pearls increases significantly with age, but they have been noted in all age groups. They are not related to other peripheral pathology and are likely of developmental origin.7
ENCLOSED ORA BAY
Enclosed and partially enclosed ora bays are relatively uncommon developmental variations. These are oval islands of pars plana epithelium located immediately posterior to the ora serrata and are completely or almost completely circumscribed by the peripheral retina (Figs. 26-12 and 26-13). The enclosed ora bay is composed of a thin layer of nonpigmented pars plana epithelium surrounded by neurosensory retina. Enclosed and partially enclosed ora bays are evident in 6% of patients, are bilateral in 8% of affected individuals, and are present in 3% of all eyes (Table 26-2). These lesions are equally prevalent nasally and temporally near the horizontal meridian.8,9
 Figure 26-12. Partially enclosed ora bay in a 20-year-old woman. Posteriorly, the ora bay extends 1.8 mm behind general line of ora serrata, and the retina shows a large area of typical cystoid degeneration. Anteriorly, the ora bay is embraced by two long dentate processes that converge toward, but do not meet, a prominent ciliary process of the pars plicata. (×12.) |
 Figure 26-13. Enclosed ora bay in a 35-year-old man. Anteriorly, two broad dentate processes converge and join to enclose a bay (island of pars plana). Posteriorly there is a focus of retinal thinning (peripheral retinal excavation; arrow). (×12.) |
PERIPHERAL RETINAL EXCAVATION
Peripheral retinal excavation appears as a small oval depression in the retina. Usually this lesion is aligned with a meridional fold or complex and located 1 to 7.2 mm posterior to the ora serrata (Figs. 26-13 and 26-14). The focal depression may be surrounded by margins that appear to be elevated; however, microscopic examination reveals that the depression corresponds to a focal loss of the inner retinal layers and that the surrounding tissue is normal (Fig. 26-15).
 Figure 26-14. Meridional complexes with peripheral retinal excavation. Two complexes can be seen anteriorly; both contain meridional folds (the fold of complex on the right is discontinuous). Peripheral retinal excavation (arrow) is aligned with the complex on the left (×12.) |
 Figure 26-15. Peripheral retinal excavation. The notable loss of tissue from the retinal surface extends to the inner nuclear layer. Centrally, the middle retinal layers show degeneration, but outer layers of retina are intact. (Hematoxylin-eosin; ×250.) |
Peripheral retinal excavation is present in 10% of patients, is bilateral in 43%, and therefore is evident in 8% of all eyes (Table 26-2). Half of the affected eyes contain two or more areas of focal excavation, and most of the excavations are located in the superior nasal quadrant.
Developmental variations of the peripheral retina are present in about 20% of eyes. These conditions have certain common features: They are present at birth, persist throughout life, tend to occur symmetrically in anatomically corresponding positions in both eyes, and are commonly associated with an abnormal alignment of a dentate and ciliary process in the same meridian.5
Clinically, these developmental abnormalities are readily identified in the peripheral retina. The ridgelike elevation of a meridional fold is best seen by scleral depression and indirect ophthalmoscopy. A meridional complex should be suspected (even though the ciliary processes are not visible) when a large dentate process, a meridional fold, and peripheral retinal excavation occur in the same meridian. An enclosed ora bay appears as a depressed, bright red area that simulates a retinal hole. Although identification of an enclosed ora bay is aided by the presence of a thin epithelial layer extending across the base and by the absence of any elevation of the surrounding retina, in some instances, distinction between an enclosed bay and a retinal hole is impossible. Peripheral retinal excavation presents as a small retinal pit that may be adjacent to or up to four disc diameters posterior to the ora serrata. This form of focal depression probably has been often mistaken for a full-thickness retinal break; therefore, knowledge of developmental variations is essential to the appropriate diagnosis of a peripheral retinal lesion.
In clinical studies, retinal breaks posterior to meridional folds have been noted in a number of eyes with rhegmatogenous retinal detachment.10 Retinal tears may also develop at or near the posterior margins of enclosed ora bays.9 Therefore, when retinal detachment is present, the ophthalmologist must carefully search for meridional folds, meridional complexes, enclosed ora bays, peripheral retinal excavations, and any associated retinal breaks.
TROPHIC PERIPHERAL RETINAL DEGENERATIONS
Peripheral retinal degeneration (i.e., irreversible retrograde change) is evident in every adult. For classification, degeneration may be regarded as trophic when the primary process is a loss of retinal tissue, tractional when the process is related primarily to tugging or pulling of vitreous or zonule on the retina, and trophic and tractional when both retinal tissue loss and vitreous-zonule traction are involved. The principal peripheral retinal degenerations are noted in Table 26-3.
 |
TYPICAL CYSTOID DEGENERATION
The most common form of degeneration of the peripheral retina is typical cystoid degeneration. Spaces develop in the outer plexiform and inner nuclear layers and coalesce to form interlacing tunnels. They are separated by pillars that extend from the inner to the outer retinal layers, giving the inner surface a uniformly stippled appearance (Fig. 26-16). The stippled depressions correspond to retinal pillars; the intervening rounded domes result from the intraretinal cystoid spaces.11 Degeneration begins at the ora serrata, particularly at the base of dentate processes, and extends posteriorly and circumferentially to form a band that may encircle the eye and extend from the ora serrata to the equator (Fig. 26-17).
 Figure 26-16. Typical and retinal cystoid degenerations. A. Degeneration of nerve fiber layer with persistence of delicate vertical columns of Müller’s cells. Superficial capillary plexus courses through the cystoid cavities, and surviving ganglion cells are subtended on the inner aspect of the inner plexiform layer (arrow). Outer retinal layers are well preserved. B. Extensive degeneration of middle retinal layers with broad cellular columns (between cystoid cavities) composed of Müller’s cells and remnants of outer plexiform layer and inner nuclear layer (vertically stretched). Outer nuclear layer also shows degeneration. Inner plexiform layer (arrow) is intact. C. Overlapping reticular (on the left) and typical (on the right) cystoid degeneration. Note combined degenerative effect on the inner plexiform layer (arrow) of both types of cystoid degeneration. Superficial small arteriole retards progression of reticular cystoid degeneration. (Hematoxylin-eosin, ×250.) (Reproduced with permission from Foos RY: Senile retinoschisis: Relationship to cystoid degeneration. Trans Am Acad Ophthalmol Otolaryngol; 4:33, 1970.) |
 Figure 26-17. Typical and reticular cystoid degeneration found immediately behind the ora serrata and about enclosed ora bay near cut edge of calotte. Posteriorly, note the conspicuous vascular pattern of degeneration (seen as gray background), finely stippled surface pattern, and angular free margins (related to limitation by surface vessels). |
Typical cystoid degeneration may be noted in infants at 1 year of age; it is always present in both eyes of patients older than 8 years of age, usually increases in area with advancing age, and is most extensive in the superior and temporal quadrants (Table 26-3).12,13
RETICULAR CYSTOID DEGENERATION
Reticular cystoid degeneration of the peripheral retina is almost invariably located posterior to and continuous with typical cystoid degeneration. It is characterized by a prominent linear or reticular pattern that corresponds to the retinal vessels and by a finely stippled internal surface. Areas of involvement are single or multiple, form the shape of an irregular angle, and are often demarcated posteriorly by retinal blood vessels (Fig. 26-17).14 Spaces develop in the nerve fiber layer and are divided by delicate retinal pillars (Fig. 26-16).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


