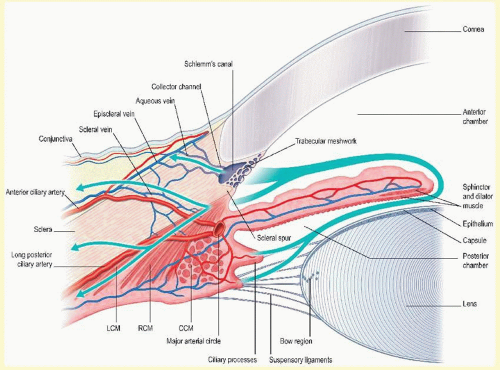
The aqueous humor is a transparent, colorless solution continuously formed from plasma by the epithelial cells of the ciliary processes. It is secreted into the posterior chamber from where it passes from the posterior chamber through the pupil into the anterior chamber and is drained at the anterior chamber angle. Most of the aqueous drains into the venous circulation via the trabecular meshwork, Schlemm canal (SC), scleral collector channels, and aqueous and episcleral veins; the remainder drains into the orbit via the interstices of the ciliary muscle, ciliary body lymphatics, the suprachoroidal space, and the sclera (Fig. 6.1). The composition and formation of aqueous resembles that of cerebrospinal fluid.1 Aqueous humor is thought to serve several functions:
1. Aqueous delivers oxygen and nutrients to, and removes waste products, blood, macrophages, inflammatory products, or other debris from, the posterior cornea, crystalline lens, and perhaps the anterior vitreous, structures that are necessarily avascular.
2. Continuous formation and drainage of the aqueous helps maintain the intraocular pressure (IOP), necessary for maintaining the shape and internal alignment of the ocular structures and, consequently, optimal optical properties.
3. The aqueous maintains a transparent and colorless medium of lower refractive index between the posterior cornea and the lens, and thus constitutes an important component of the eye’s optical system.
Circulation of the aqueous in the anterior chamber occurs via hydrostatic phenomena, including mechanical forces caused by eyeball and head movements, thermal currents resulting from the temperature differential between the warmer vascular iris and the cooler avascular cornea, and the pressure gradients between the posterior chamber, anterior chamber, and episcleral veins. As the fluid bathes the anterior lens, iris, and corneal endothelium, its composition is altered as a result of the exchange of nutrients, cellular waste products, and other substances within these structures. The entire volume of the aqueous humor is replaced every 90 to 100 minutes.2
Continuous formation and drainage of the aqueous is essential to the good health of the eye. In the absence of aqueous circulation, the cornea is thickened, the anterior chamber is absent, the iris is partly atrophic, and the lens is cataractous.3
This chapter reviews the anatomy and physiology of aqueous humor circulation, from formation to drainage. The ciliary body and its secretory mechanisms, the blood-aqueous barrier, the aqueous humor composition, the methods of measuring the aqueous flow rate, and factors affecting it, the pathways of aqueous flow within the eye, and the aqueous outflow system are all discussed.
ANATOMY OF THE CILIARY BODY
The ciliary body forms a ring along the inner wall of the eyeball and extends anteriorly from the scleral spur and iris to the ora serrata posteriorly. The greater part of the ciliary body mass is accounted for by the ciliary muscle, the bundles of which are arranged in three regional orientations: radial, circular, and longitudinal. When viewed in transverse section, the ciliary body appears as an isosceles triangle. The base of the triangle faces anteriorly, while one of its sides lies along the sclera, separated from it only by a potential space continuous with the suprachoroidal space. The other side, or inner portion of the ciliary body, is divided anatomically into two parts: the posterior portion (pars plana) and the anterior portion (pars plicata). Projecting inwardly from the pars plicata are approximately 70 villuslike structures: the ciliary processes. Viewed posteriorly, the ciliary processes appear as radial ridges, to which collectively the name corona ciliaris has been given. It is the ciliary processes that are responsible for aqueous formation.
The ciliary processes are long and slender in early life but become more blunt in later years. Their dimensions vary but average 2 mm in length anteroposteriorly, 0.5 mm in width, and 1 mm in height.4 The processes are greatly convoluted. Structurally, they consist of capillaries surrounded by a loose connective tissue, encircled by a double epithelial layer. This structure provides a large surface area for capillaries to be in close proximity to the double layer of epithelium and for the epithelium to face the posterior chamber. This arrangement maximizes access of the ciliary body secretions into the small space of the posterior chamber.
FIG. 6.1 Schematic representation of the primate anterior ocular segment. Arrows indicate aqueous humor flow pathways. Aqueous humor is formed by the ciliary processes, enters the posterior chamber, flows through the pupil into the anterior chamber, and exits at the chamber angle via the trabecular and uveoscleral routes. (Modified from Kaufman PL, Wiedman T, Robinson JR. Cholinergics. In: Sears ML, ed. Pharmacology of the Eye: Handbook of Experimental Pharmacology. Berlin, Heidelberg: Springer-Verlag; 1984:149-191. Reprinted with permission.)
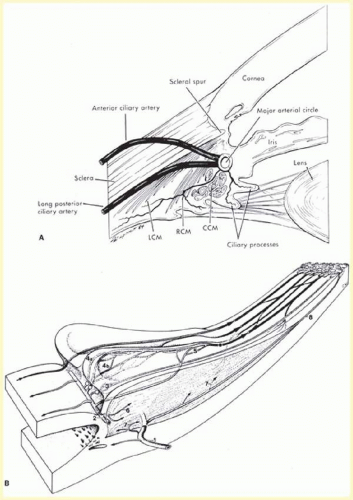
The blood supply of the ciliary body has a dual origin.4,5,6,7,8,9,10,11,12 The two (medial and lateral) long posterior ciliary arteries, which penetrate the sclera posteriorly and travel anteriorly in the suprachoroid, give rise to the major arterial circle of the iris, the vascular structure that supplies the inner and anterior division of the ciliary muscle, ciliary processes, and iris.12 The seven anterior ciliary arteries, which penetrate the sclera anteriorly after supplying the extraocular rectus muscles, also contribute to the major iris arterial circle, and the outer and posterior areas of the ciliary muscle, and the peripheral (anterior) area of the choroid. The microvasculature of the ciliary processes, arising from the short radial ciliary arteries, which in turn arise from the major arterial circle of the iris, is arranged into three distinct vascular areas. The first of these is located at the anterior end of the major processes, with venous drainage achieved via venules passing the ciliary body. The second and third vascular areas supply the major and minor ciliary processes and are drained posteriorly by venules located at the margin of the ciliary processes. The system of ciliary process venules in turn drains mainly through the vortex system of the choroid. Each short radial ciliary artery has many branches, providing an extensive capillary network (Fig. 6.2). The capillaries of the ciliary processes are large, thin-walled, and highly fenestrated. Thus, the capillary network of the ciliary processes provides a large surface area of highly permeable vessels to initiate the process of aqueous formation.
The capillaries are surrounded by the stroma, which consists mainly of loose connective tissue and collagen. A basement membrane, which is the thickened anterior continuation of Bruch membrane separating choroid and retinal pigment epithelium, separates the stroma from the epithelial layers.
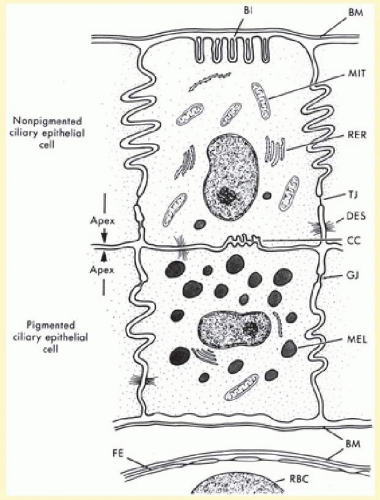
The ciliary epithelial cells have been subject to intensive study by light and electron microscopy. A striking feature is the interdigitation of the lateral surfaces of adjacent cells and the basal infoldings (Fig. 6.3), which are characteristic features of secretory epithelia concerned with fluid transport.13 The relation of the two epithelial cell layers is of importance because as the secreted aqueous is derived from an ultrafiltrate of blood in the stroma of the ciliary body, transport must occur across both layers. The double-layered ciliary epithelium itself is derived from anterior continuations of the retinal pigmented epithelium (forming the pigmented layer), and the neuroepithelium from which the retinal cells are derived (forming the nonpigmented layer). However, during embryogenesis, invagination of the neuroepithelium occurs, with the result that the apical surfaces of each cell layer in the ciliary epithelium face one another, while the basolateral surface of the nonpigmented layer faces directly into the posterior aqueous chamber. Conversely, the basolateral surface of the pigmented layer is tightly bound to the basement membrane. Cells of the pigmented epithelium contain many melanin granules. Gap junctions are present between the lateral interdigitations of the pigmented cells. Desmosomes also occur between the lateral interdigitations of the pigmented and nonpigmented epithelia and between their apical membranes.
The cells of the inner nonpigmented epithelium possess numerous intermediate-sized mitochondria, and the rough endoplasmic reticulum is particularly well developed, indicative of active protein synthesis. Small vacuoles may be present in large numbers near the apex of these cells. Occasionally, a few pigmented granules may be seen. Tight junctions are present in the lateral interdigitations between the nonpigmented cells (Fig. 6.3), thus forming a barrier for the passage of larger molecules between the cells. This important physiologic barrier, constituting part of the blood-aqueous barrier, is discussed further in a later section.
The internal limiting membrane of the ciliary body is a more complex and thicker structure than its posterior counterpart on the retina, in part because it serves as the basement membrane for the inverted nonpigmented ciliary epithelium, and as the site of insertion of the zonular fibers,4 to which the lens is attached.
FORMATION AND SECRETION OF AQUEOUS HUMOR
Early in the 20th century, aqueous humor was regarded as a stagnant fluid.14 However, this misconception was revoked after a number of experiments designed to investigate this were carried out, including Seidel’s procedure,15 in which a cannula connected to a reservoir of indigo carmine dye was inserted into the anterior chamber of the rabbit eye. The reservoir was raised, thus creating a pressure of 15 mm Hg, and the dye was seen to enter the anterior chamber and subsequently the episcleral veins. From this, it was concluded that aqueous humor is continuously formed and drained, and it is to a large extent from this historic work that the modern study of aqueous humor dynamics has developed.
Other aspects of the anatomy and physiology of aqueous drainage were discovered subsequently. Boerhaave first described the presence of the aqueous veins,16 and Ascher17 observed a clear fluid in the veins of the episclera and demonstrated by means of external compression with a glass rod that these veins were interconnected with veins containing blood. Goldmann18 demonstrated that these vessels contained aqueous humor by injecting fluorescein intravenously and observing the dye entering the anterior chamber and subsequently the aqueous veins. Ashton19 identified an aqueous vein in a living human eye, and postmortem examination using a neoprene cast showed that there was a direct passage between the vessel and Schlemm’s canal.
Three physiologic processes are known to contribute to the formation and chemical composition of the aqueous. These are diffusion, ultrafiltration (and the related dialysis), and active secretion. The first two are passive and, therefore, require no active cellular participation. Diffusion of solutes across cell membranes occurs down a concentration gradient. Substances with high-lipid solubility coefficients that can easily penetrate biological membranes move readily in this way. Ultrafiltration is the term used to describe the bulk flow of blood plasma across the fenestrated ciliary capillary endothelia, into the ciliary stroma, which can be increased by augmentation of the hydrostatic driving force. This process is responsible for the formation of the reservoir of the plasma ultrafiltrate in the stroma, from which the posterior chamber aqueous is derived, via active secretion across the ciliary epithelium. Active secretion requires energy, normally provided via the hydrolysis of adenosine triphosphate (ATP). The energy is used to secrete substances against a concentration gradient.
FIG. 6.2 A: Blood supply to the ciliary processes. LCM, longitudinal ciliary muscle; RCM, radial ciliary muscle; CCM, circular ciliary muscle. B: Vascular architecture in the human ciliary body. (1) Perforating branches of the anterior ciliary arteries; (2) major arterial circle of the iris; (3) first vascular territory. The second vascular territory is depicted in 4a, marginal route and 4b, capillary network in the center of this territory; (5) third vascular territory; (6 and 7) arterioles to the ciliary muscle; (8) recurrent choroidal arteries. Light circles, terminal arterioles; dark circle, efferent venous segment. (A, Reprinted from Caprioli J. The ciliary epithelia and aqueous humor. In: Hart M, ed. Adler’s Physiology of the Eye. 9th ed. St Louis, MO: Mosby Year-Book; 1992:228-247, with permission.) (B, Reprinted from Funk R, Rohen JW. Scanning electron microscopic study on the vasculature of the human anterior eye segment, especially with respect to the ciliary processes. Exp Eye Res. 1990;51:651-661, with permission.)
FIG. 6.3 Schematic diagram of nonpigmented and pigmented epithelial cells. Note apices of cells facing each other. BI, basal infoldings; BM, basement membrane; CC, ciliary channels; DES, desmosomes; FE, fenestrated capillary endothelium; GJ, gap junction; MEL, melanosome (MEL); MIT, mitochondrion; RBC, red blood cell; RER, rough endoplasmic reticulum; TJ, tight junction. (Reprinted from Caprioli J. The ciliary epithelia and aqueous humor. In: Hart M, ed. Adler’s Physiology of The Eye. 9th ed. St Louis, MO: Mosby Year-Book; 1992:228-247, with permission.)
Of these three processes, active secretion is believed to contribute the most to the chemical composition and volume of the posterior chamber aqueous, accounting for 80% to 90% of total aqueous humor formation.20,21,22,23,24,25,26,27,28
SECRETION
Secretion implies an active process that selectively transports some substances across the cell membrane. Because energy is consumed, substances can be moved across a concentration gradient in a direction opposite to that which would be expected by passive mechanisms alone. One example of this is the ability of the thyroid gland to accumulate iodide at up to 40 times the circulating plasma level.26,29 Aqueous humor exhibits increased ascorbate, lactate, and certain amino acid concentrations as compared with plasma, as a consequence of active secretion.1
Another way of testing for the presence of an active metabolic process is to apply specific metabolic inhibitors to the ciliary body and observe the effect on aqueous secretion. For example, systemic30 or intravitreal injection31 of ouabain (an inhibitor of the enzyme sodium-potassium-activated adenosine triphosphatase [ATPase]—Na+/K+ ATPase) results in a decrease of up to 70% in aqueous formation, in various species. The topical administration of vanadate (also a Na+/K+ ATPase inhibitor) lowers aqueous secretion in rabbits32,33 and monkeys.34 Oubain, as well as several other ion transport and channel blocking drugs, significantly reduce aqueous humor formation in arterially perfused bovine eyes. Bumetanide (a specific inhibitor of Na-K-2Cl cotransport) and furosemide (a nonspecific anion transport inhibitor) reduce aqueous humor formation by 35% and 45% in bovine eyes in vitro. Similarly, 4,4′-diisothiocyanatostilbene-2,2′-disulfonic acid (DIDS, a probable inhibitor of the Cl-HCO3 exchanger, the Na-HCO3 cotransporter, and chloride channel) reduces aqueous humor formation by 55% in bovine eyes and 25% in porcine eyes in vitro,35,36 and 5-nitro-2-(3-phenylpropylamino)-benzoic acid (NPPB, a chloride channel blocker in nonpigmented cells) reduces aqueous humor formation 25% in bovine eyes in vitro.35 Also, catecholamines such as epinephrine, norepinephrine, isoproterenol, and dopamine that stimulate aqueous humor formation in humans also stimulate Na-K-Cl cotransport.37 Acetazolamide, and other specific inhibitors of the enzyme carbonic anhydrase, decrease the formation of aqueous by 40% to 60%.38,39,40 A reduction in temperature, which inhibits most active metabolic processes, also results in a decrease in aqueous formation, to a greater extent than would be expected if only diffusion were operating.1,41
Active transport systems usually exhibit a limit beyond which an increase in substrate concentration produces no further increase in transport. When this limit is reached, the system is said to be saturated. Thus, the fact that a transport mechanism for a substance can be saturated provides evidence of an active system. It has been demonstrated that by increasing the ascorbate concentration in plasma, a level of plasma ascorbate is reached above which no further increase in aqueous ascorbate concentration will occur. This provides evidence that the ascorbate transport system in the eye is saturable.
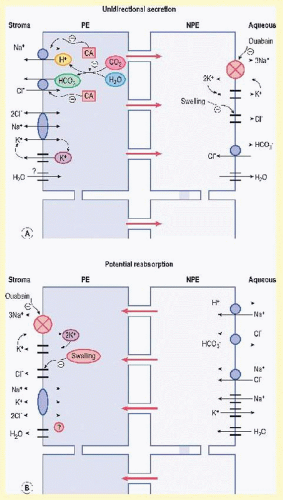
Several membrane active transport systems have been identified in the ciliary epithelium that are known to pump various substances against a concentration gradient, including Na+/K+ ATPase, carbonic anhydrase, Na+-K+-2Cl– symport parallel Cl–/HCO3– and Na+/H+ antiports as well as amino acid membrane transporters (Fig. 6.4). There are also passive transport proteins specific for HCO3– and Cl–. Membrane-bound Na+/K+ ATPase is one important system involved in Na+ and K+ transport and is present mainly along the lateral cellular interdigitations of the nonpigmented ciliary epithelium.30,42,43,44,45,46,47 The transmembrane Na+/K+ transport protein is energized by the Gibbs free energy of hydrolysis of ATP, mediated by the ATPase enzyme intimately associated with it in the membrane. The ATP required for this process is derived predominantly from oxidative metabolism of glucose via Krebs citric acid cycle. The Na+ pump induces a potential difference across the ciliary body, ranging from 6 to 10 mV. Measurements of the potential difference across the ciliary epithelia indicate that the aqueous is positive with respect to the stroma.48 These data are consistent with the hypothesis that Na+ is the primary mover and that active transport of Cl– is probably small in comparison with that of Na+.49 Interspecies differences in the aqueous-plasma ratios of Cl– (e.g., high in human, low in rabbits) might be explained by the relative proportions of Cl– actively transported.50 Transepithelial electrical measurements in the isolated rabbit iris-ciliary body (ICB) indicate that Na+/K+ ATPase and HCO3– are required for active ion transport.51
FIG. 6.4 Pathways for unidirectional secretion (A) and possible reabsorption (B) across the ciliary epithelium. PE, pigmented ciliary epithelial cells; NPE, nonpigmented ciliary epithelial cells. (Reprinted from McLaughlin CW, Zellhuber-McMillan S, Macknight ADC, et al. Electron microprobe analysis of rabbit ciliary epithelium indicates enhanced secretion posteriorly and enhanced absorption anteriorly. Am J Cell Physiol. 2007;293:C1455-C1466, with permission.)
However, more recent studies demonstrating a negative potential difference across the ciliary epithelium have called into question the idea of primary Na+ transport across the ciliary epithelium.52 Transepithelial electrical measurements in the isolated porcine ciliary body epithelium showed an aqueous negative potential difference indicating active Cl– transport.53 Like the human, high aqueous-plasma ratios of Cl– have also been reported in cows, pigs, and sheep in vivo.54
Several studies suggest that active transport of Cl– ions35,37,55 provides the major driving force for aqueous humor formation in most mammalian species.52,53,55,56,57,58,59 This involves stromal Cl– uptake into pigmented cells by electroneutral transporters (Na+-K+-2Cl– symport, Cl–/HCO3– and Na+/H+ antiport) diffusion through gap junctions to nonpigmented epithelial cells, and Cl– exit into the aqueous humor through Cl– channels.59 It is thought that Cl– secretion provides the primary driving force for active water transport across ocular tissues such as the ciliary epithelium.60 Bestrophin-2 (Best2), a protein that is found in the nonpigmented ciliary epithelium and is linked to Ca2+ sensitive Cl– transport, likely plays a role in aqueous humor formation. Best2 null mice have found to have significantly lower IOP compared with normals.61
Water transport across many membranous barriers, including those in the eye, is facilitated by aquaporin (AQP) water channels.62 The AQPs are a family of molecular water channels expressed in animals, plants, and lower organisms that aid in the rapid bulk transport of fluid and with the transport of fluid against an insufficient osmotic pressure gap.62,63 There are at least 13 mammalian AQPs each of which is a small membrane protein approximately 30 kD in size. The eye expresses several AQPs at sites of fluid transport. Two AQPs (AQP160,62,64,65 and AQP460,65,66) are expressed in the nonpigmented ciliary epithelium and have been found to contribute to aqueous humor secretion.65,67 AQP1- and/or AQP4-null mice have decreased IOP and aqueous humor production compared with wild-type normals.62,65 This provides evidence for the role of AQPs in the regulation of IOP and aqueous humor production through transport of fluid.
Histochemical studies have demonstrated several active enzyme systems in the ciliary epithelia. These include nucleotide phosphatases (especially ATPase, as mentioned previously), adenylate cyclase, and carbonic anhydrase, the enzyme that forms HCO3– (the body’s alkaline ion) from CO2 and H2O68,69,70,71,72 by the following reaction:
Carbonic anhydrase catalyzes step I of the reaction, and step II is an almost instantaneous ionic dissociation.73,74 The enzyme is localized in pigmented and the nonpigmented ciliary epithelium of rabbit, monkey, and human75,76 most prominently in the basal and lateral membranes, but also in the cytoplasm. A variety of carbonic anhydrase inhibitors (CAIs) will reduce aqueous secretion, including acetazolamide,77 dorzolamide,78,79,80 brinzolamide,81,82,83 and several biscarbonylamidothiadiazole compounds.40 The site of action of these drugs is intraocular rather than systemic, because the unilateral injection of acetazolamide into the carotid artery lowers the IOP of only the ipsilateral feline eye.84 It has been irrefutably demonstrated that acetazolamide exerts its ocular effects via a reduction in aqueous secretion, mediated by a direct effect on the ciliary epithelial cells.25 Inhibition of the enzyme decreases the rate of Na+ and HCO3– transport into the posterior chamber by equimolar amounts, indicating a linkage of the accession of these two solutes into the posterior chamber of dogs and monkeys.85 Furthermore, inhibition of carbonic anhydrase lowers the aqueous Cl– concentration in primates and the HCO3– concentration in rabbits.23,86 It is now known that the primary reaction catalyzed by carbonic anhydrase, which occurs within the cytosol of the nonpigmented ciliary epithelial cells, is the proteolysis of water to yield OH– and H+ ions. The hydroxide ions so formed react with CO2 catalytically (or noncatalytically when the enzyme is inhibited) to form HCO3–, which is passively transported to the aqueous humor, simultaneously with the active transport of Na+. The protons liberated from water pass into the blood circulation where they are buffered by proteins. The catalytic rate (i.e., when active carbonic anhydrase is present) is 7 µmol per minute, and the uncatalyzed is 0.07 µmol per minute.
Inhibition of the flow of bicarbonate also leads to an inhibition of the flow of Na+. Several hypotheses have been put forward to explain this: (1) inhibition of carbonic anhydrase causes a decrease in HCO3– available for movement with Na+ to the aqueous side to maintain electroneutrality; (2) a reduction in intracellular pH may inhibit Na+-K+ ATPase; and (3) decreased availability of H+ produced by the reaction catalyzed by carbonic anhydrase decreases H+/Na+ exchange and reduces the availability of intracellular Na+ for transport into the intercellular channel.
However, HCO3– constitutes on 20% to 25% of the total anion composition of the aqueous humor in all mammalian species, so that cations secreted are likely predominantly accompanied by Cl-59 as discussed above.
A large excess of carbonic anhydrase has been found in the ciliary processes of all species studied. This has pharmacologic implications when one hopes to reduce aqueous secretion by inhibition of the enzyme. In order to achieve a clinically useful reduction in the secretion and hence IOP, more than 99% of the enzyme must be inhibited.
Topically applied CAIs have been developed for clinical use. Dorzolamide has been used81,87,88 since 1995 and brinzolamide since 1998.81 As a rule, the topically active CAIs have a very high lipid and water solubility, as well as a high-inhibitory potency and efficacy. Sufficient concentration is achieved in the ciliary processes via transcorneal, aqueous humor, and iris absorption after instillation of a single drop.39,88,89 Some studies have found topically applied CAIs to be less effective at lowering IOP than oral acetazolamide,90,91 thus oral CAIs are still in clinical use and are sometimes preferred for the management of ocular hypertension and glaucoma.91,92
In summary, the current understanding of aqueous humor formation is that the driving force for aqueous inflow is derived from transepithelial ion transport through which an osmotic gradient for water movement is generated. The process begins with an ultrafiltrate of plasma in the extravascular spaces of the ciliary stroma. The ciliary epithelium then incorporates certain molecules and ions selectively for concentration and direct active secretion into the posterior chamber, whereas other substances are secreted passively. Chloride secretion appears to play a central role in the aqueous humor formation.
Other substances such as certain amino acids are also actively transported. Some other small molecules probably appear in the aqueous via diffusion or ultrafiltration. The ciliary epithelium also produces peptides that influence aqueous inflow and outflow thus acting as a neuroendocrine system (see Aqueous Humor Composition section).93
BLOOD-AQUEOUS BARRIER
Large molecules such as proteins are present in the aqueous in only small quantities, even if their respective concentrations in the plasma are raised to high levels. In humans, normal plasma total protein levels are 6 g per 100 mL, compared with less than 20 mg per 100 mL in the aqueous, less than 0.5% that of plasma.94,95 Thus, a restraint in the free passage of many solutes from the blood vessels of the ciliary stroma into the aqueous humor exists. This constitutes one component of the blood-aqueous barrier,1,96 the anatomical correlate of which are the tight junctions between the interdigitating surfaces of the nonpigmented ciliary epithelial cells. Bill97,98 demonstrated that albumin and other proteins pass through the ciliary capillary walls at a much faster rate than they enter the aqueous humor and concluded that a barrier to these substances existed at a site other than the vessel walls. Numerous studies have tested the blood-aqueous barrier using a number of different intravascular tracers designed to mimic the behavior of plasma-proteins.2 The conclusion of these studies is that tight junctions between the apicolateral surfaces of the nonpigmented epithelium of the ciliary body, and between the endothelial cells of the iris vasculature, prevent the passage of plasma proteins into the aqueous humor.99,100,101,102,103,104,105,106,107
The blood-aqueous barrier is not absolute. Watersoluble substances of medium molecular weight such as urea, creatinine, and certain sugars may penetrate at varying rates, but all are slower than their transit across capillary walls. Generally, the greater the lipid solubility coefficient of a substance, the greater its ability to penetrate the blood-aqueous barrier and pass to the posterior aqueous chamber.1,108,109,110 In addition, regional differences of permeability in the ciliary body have been noted. For instance, the epithelia of the anterior portions of the ciliary processes of the rabbit are less permeable than the epithelia of the pars plana.102
Substances such as mannitol are used clinically to reduce IOP. They function as hyperosmotic agents, by exploitation of the fact that they penetrate the blood-aqueous barrier only poorly but are distributed widely within the extracellular spaces of the body. Water is drawn from cells and the ocular fluids, balancing the high-osmotic pressure induced in the extracellular space via the high concentrations of mannitol. The resulting loss of water from the eye leads to a reduction in the IOP.1 The effect of hyperosmotic agents is most pronounced in eyes exhibiting pathologically elevated IOP.111
Certain antibiotics (e.g., chloramphenicol, cephalothin, and ampicillin) are known to penetrate the blood-aqueous barrier well, whereas others do so only poorly (e.g., penicillin, methicillin, erythromycin, and gentamicin).
SECONDARY AQUEOUS
The blood-aqueous barrier is fragile and may be disturbed by various noxious stimuli. A corneal abrasion, paracentesis (withdrawal of a small volume of aqueous via a needle inserted into the anterior chamber),112,113,114,115,116 intraocular infection, uveal inflammation, intraocular surgery, and certain drugs, applied topically (such as nitrogen mustard or an anticholinesterase, e.g., echothiophate, diisopropyl fluorophosphate [DFP], demecarium, neostigmine, or physostigmine), or delivered by intracarotid infusion, such as hyperosmotic agents (causing separation of the ciliary epithelial layers, opening of the blood-aqueous barrier, and severe, permanent damage to the pigmented epithelial cells117), are all capable of breaking down the blood-aqueous barrier and inducing changes in the aqueous humor composition (Table 6.1). Disruption of the blood-aqueous barrier has also been reported in the contralateral eyes of patients who have had cataract extraction and lens implantation surgery,118 and after argon laser trabeculoplasty.119 Severe damage to the blood-aqueous barrier occurs with cyclo-destructive procedures used to treat advanced glaucoma and is evidenced by the prolonged or chronic presence of flare (the scattering of light upon slit-lamp examination by increased levels of protein in the anterior chamber).
After breakdown of the blood-aqueous barrier, the resultant aqueous produced is known as “secondary” or “plasmoid” aqueous.1,23,120,121 The most notable change is a marked increase in protein concentration. In this situation, the ionic composition of the aqueous approaches that of a simple dialysate of plasma, and substances that are normally barred from entering the aqueous now do so with ease. The unusually rapid rate of entry of substances such as fluorescein, Evan blue dye, albumin, or fibrinogen (which actually may allow the aqueous to coagulate) can be used as a diagnostic indicator of barrier breakdown.
Many of the processes that disrupt the blood-aqueous barrier also lead to vasodilation. Vasodilation can occur by means of an axon reflex (as may be seen after abrasion of the cornea), a sudden drop in IOP, or inflammation.122,123 In any case, vasodilation may be associated with loss of some of the tight junctions in the iridial vessels, which may help explain the breakdown of the barrier.122
TABLE 6-1. Factors Interrupting the Blood-Aqueous Barrier
I. Traumatic
A. Mechanical
1. Paracentesis
2. Corneal abrasion
3. Blunt trauma
4. Intraocular surgery
5. Stroking of the iris
B. Physical
1. X-ray
2. Nuclear radiation
C. Chemical
1. Alkali
2. Irritants (e.g., nitrogen mustard)
II. Pathophysiologic
A. Vasodilation
1. Histamine
2. Sympathectomy
B. Corneal and intraocular infections
C. Intraocular inflammation
D. Prostaglandins
E. Anterior segment ischemia
III. Pharmacologic
A. Melanocyte-stimulating hormone
B. Nitrogen mustard
C. Cholinergic drugs, especially cholinesterase inhibitors
D. Plasma hyperosmolality
(Reprinted with permission from RL Stamper, MD)
In addition, it has been suggested that plasma proteins and other constituents can leak in a retrograde manner through Schlemm’s canal, and, therefore, account for the breakdown of the barrier after paracentesis.124
Release of prostaglandins causes vasodilation and many other changes associated with inflammation. Evidence points to the possible involvement of this class of compounds with breakdown of the blood-aqueous barrier.121,125,126,127,128,129,130,131 Prostaglandins have been implicated in the irritative response after mechanical trauma to the eye, and cause miosis, vasodilation, release of protein into the aqueous, and elevated IOP.
Pretreatment with inhibitors of prostaglandin synthesis such as indomethacin or aspirin will inhibit breakdown of the blood-aqueous barrier, as well as some of the other manifestations of inflammation ordinarily induced by the aforementioned process.132,133,134,135,136 It may well be that prostaglandin release represents a final common pathway for the action of many different kinds of trauma and irritants. However, small doses of particular prostaglandins (especially prostaglandin F2α [PGF2α] and certain congeners) applied topically to the eyes of cynomolgus monkeys and humans result in a large increase in uveoscleral outflow, with a concomitantly large decrease in IOP, without clinically evident ocular inflammation.129,130,137,138,139,140,141,142 In the past decades, PGF2α analogs such as latanoprost,143,144,145,146,147,148 travoprost and the prostamide, bimatoprost have been approved for clinical use and are now some of the most commonly used drugs in the treatment of primary open-angle glaucoma (POAG) and ocular hypertension (see Uveoscleral Outflow section for greater detail).149,150
AQUEOUS HUMOR COMPOSITION
In the healthy eye, the aqueous humor has a refractive index taken to be constant at a value of 1.336.151 Because this index of refraction is lower than that of the cornea, there is a slight divergence of light rays as they pass the cornea-aqueous interface. Both the viscosity and density of aqueous humor are slightly higher than that of pure water, whereas the osmolality is slightly higher than that of plasma.120,152,153,154,155
The volume of the human anterior chamber is approximately 200 µL,3 whereas that of the posterior chamber is approximately 60 µL.1 This makes chemical analysis of the aqueous quite difficult because of the tiny volume of fluid as well as the relatively poor accessibility of the posterior chamber. Furthermore, it may account for the differences in values for the concentrations of many substances obtained by different investigators.
The greatest difference between aqueous and plasma resides in the very low-protein concentration in the aqueous, which is in the region of 0.5% that of plasma.94,95,152,153,154,155 The composition of protein in the aqueous is also different from that in plasma. The ratio of the levels of the lower molecular weight plasma proteins (such as albumin and the β-globulins) to the higher molecular weight proteins (such as the β-lipoproteins and the heavy immunoglobulins [Igs]) is much higher in aqueous in the normal healthy eye than in plasma.156 However, when the blood-aqueous barrier breaks down (as in uveitis), the composition and concentrations of protein in the aqueous are similar to that of plasma.95 In a recent study that utilized different methods of analysis including mass spectrometry, Western blot, antibody-based, chemokine, and cytokine arrays, a total of 676 nonredundant proteins were identified in the aqueous humor of cataractous, but otherwise normal human eyes.157 Mass spectrometry alone identified 355 proteins most of which were characterized as having structural, enzymatic, or catalytic properties with a small percentage classified as growth factors, cytokines, or receptors.157 In the healthy eye, IgG is present at a concentration of approximately 3 mg per 100 mL,158 whereas IgM, IgD, and IgA are absent, presumably because of their larger molecular structure. In eyes with uveitis, the concentration of IgG increases, and IgM and IgA also appear. In the normal aqueous, trace concentrations of complement proteins and complement regulatory molecules are found.157,159
There are also trace quantities of several components of the fibrinolytic and coagulation system present in the aqueous, with the exception of plasminogen and plasminogen proactivator, which are present at more significant concentration. Only trace quantities of the inhibitors of plasminogen activation are present in the aqueous,160 thereby ensuring that the aqueous outflow pathways remain free of fibrin. The aqueous humor of diseased eyes incorporates significant quantities of all of the major components of coagulation and fibrinolysis, giving rise to the formation of intracameral clots; however, the composition of these clots is different from those that occur in the blood vessels.23
Aqueous humor also contains measurable amounts of mono- and dinucleotides that are thought to play a role in the control of corneal endothelium ion transport and IOP regulation.161,162
The α and γ lens crystallins are present in only small amounts in the aqueous humor of healthy eyes, although the concentration of these proteins increases in cataract.163,164
It has been calculated that in the normal healthy eye, the blood-aqueous barrier behaves as a semiporous membrane with a pore radius of approximately 10.4 nm. The protein concentration in the peripheral portion of the anterior chamber, close to the meshwork, may be much higher than in the more central region because of protein entry directly from the peripheral iris, as demonstrated in monkey and human eyes.165,166,167,168 Inclusion of serum in the perfusand of monkey169 or bovine170 eyes decreases resistance washout. The reduction in washout may be the result of interactions of particular serum proteins and not due to the general level of serum proteins.171
An additional source of proteins in the aqueous humor is the ciliary epithelium itself after de novo synthesis, processing, and secretion. The ciliary body expresses genes encoding a wide array of molecules including plasma proteins, protease inhibitors, neuropeptides, hormone peptides, angiotensin, antiangiogenic proteins, steroidconverting enzymes, and growth factors suggesting that the ciliary epithelium includes neuroendocrine and steroidogenic activities (reviewed in Coca-Prados and Scribano93). Neuropeptides released by the ciliary epithelium into the aqueous humor can serve as messengers in the anterior segment of the eye to possibly regulate inflow and outflow.
The concentration of amino acids is frequently higher in the aqueous than in the plasma.172 At least three transport systems for amino acids have been proposed in the eye,50 one each for the acidic, basic, and neutral groups. A statistical study of the covariation of the concentration of amino acids and related compounds in human aqueous suggested the existence of six transport systems in the ciliary epithelia: three independent mechanisms for neutral amino acids and independent mechanisms for basic amino acids, acidic amino acids, and urea.173
The distribution of ions varies greatly among different species. For example, the monkey has a higher concentration of H+ and Cl– and a lower concentration of HCO3– as compared with plasma. On the other hand, rabbit aqueous has a lower concentration of Cl– and H+ and a higher concentration of HCO3– as compared with plasma.174 The concentration of Na+ in the aqueous is almost the same as in the plasma in many species.1,120,175 However, the osmotic pressure of aqueous is slightly higher than that of plasma with respect to Na+, because of the Gibbs-Donnan equilibrium.
Most species tested have very high concentrations of ascorbate and lactate in the aqueous. Ascorbate is actively secreted into the posterior chamber, and the secretion mechanism will only function in the presence of ATP and a Na+ gradient. The physiologic function of ascorbate remains to be elucidated; however, it is known to be concentrated by the lens epithelium176 and has been shown to have a protective effect against UV-induced DNA damage to lens epithelium.177 Ascorbate may function as an antioxidant, regulate the sol-gel balance of mucopolysaccharides in the trabecular meshwork, or partially absorb UV radiation,178,179 because diurnal mammals have approximately 35 times the concentration of aqueous ascorbate than nocturnal mammals.180
The key oxidant in the aqueous humor, hydrogen peroxide, is normally present181 as a result of reactions of ascorbic acid and trace metals.182 Additional hydrogen peroxide and reactive oxygen species are generated by light-catalyzed reactions, metabolic pathways, and phagocytic or inflammatory processes.181,182 Ascorbate has been found to increase photoproduction of hydrogen peroxide in both bovine and human iridial melanin.183 Hydrogen peroxide affects aqueous outflow in the calf perfusion system.184 Human trabecular meshwork cells exposed to 1 mM hydrogen peroxide show reduced adhesiveness to the extracellular matrix proteins fibronectin, laminin, and collagen types I and IV.185 Extensive and repeated oxidative stress in vivo may result in reduced trabecular meshwork cell adhesion, leading to cell loss that is identified as one of the major culprits in glaucomatous conditions.186,187,188,189,190,191 Decreased antioxidant levels have been found in patients with POAG when compared with aqueous humor from patients with cataracts, suggesting that increased peroxidation may be involved in the development of glaucoma.192 Increased oxidative DNA damage has also been found, along with decreased total antioxidant status, in the aqueous humor and serum of patients with POAG compared with those with cataracts.193
Lactate is produced as a result of the glycolytic degradation of glucose by both the ciliary body and the retina.194 It diffuses into the posterior chamber but is present at only marginally higher concentration than in the plasma at this site. However, it accumulates in the anterior chamber at considerably higher concentration than in the plasma. The activity of lactate dehydrogenase (LDH) and α-hydroxybutyrate dehydrogenase (an isoenzyme of LDH) enzymes and the level of lactate were increased in the aqueous humor of patients with POAG versus patients with cataracts.195
Glucose, urea, and nonprotein nitrogen concentrations are slightly less than that in plasma.1,120 Glucose is thought to diffuse into the aqueous, where its concentration is approximately 80% that of plasma. It also diffuses into the cornea. Its concentration within the corneal endothelium is approximately half that in the aqueous. In diabetes mellitus, the aqueous concentration of glucose is increased. High-glucose levels in the aqueous humor may increase fibronectin synthesis and accumulation in the trabecular meshwork and accelerate the depletion of trabecular meshwork cells. In bovine trabecular meshwork cells grown in high-glucose medium, fibronectin mRNA is significantly upregulated, fibronectin immunofluorescence is more intense, and relative amounts of fibronectin protein are significantly increased.196 Also the chemoattractant potential of fibronectin in aqueous humor is reported to play a role in trabecular meshwork cell loss in glaucoma.197
Oxygen is also present in the aqueous humor, at a tension determined to lie between 13 to 80 mm Hg, depending upon the method of measurement.198,199,200,201,202 The tension of oxygen in the aqueous can be decreased by topical epinephrine, possibly as a result of uveal vasoconstriction199 or by the wearing of polymethylmethacrylate (Perspex) contact lenses, which, by restricting the normal passage of oxygen across the corneal epithelium, cause corneal hypoxia and thus an increase in movement of oxygen from the aqueous, across the corneal endothelium.198
Lipids such as sphingomyelin, phosphatidyl choline, and lysophosphatidyl choline have all been shown to be present in the rabbit aqueous,203 although at a concentration of less than 1 mg per 100 mL, because lipids are largely barred from entry to the aqueous by the blood-aqueous barrier.204 There appears to be a link between the occurrence of lysophosphatidic acid responsiveness in keratocytes activated by injury and the increase in lysophosphatidic acid-like activity in aqueous humor.205
Other substances, such as corticosteroids,206 monoamine metabolites,207 Cr3+ ions,208 vitamin B12,209 sialic acid,210 and hyaluronic acid,211 have all been found to exist in the aqueous of several different species. Hyaluronic acid covering the surfaces of the outflow pathways might prevent adherence of molecules to extracellular matrix components within the cribriform region and thereby prevent clogging of the outflow pathways.212 Knepper et al.213 hypothesize that POAG is characterized by a decreased concentration of hyaluronic acid and increased turnover and downregulation of the hyaluronic acid receptor CD44 in the eye, which, in turn, may influence cell survival of TM and retinal ganglion cells. Corticosteroid regulation of IOP is proposed to occur via 11 β-hydroxysteroid dehydrogenase (HSD)-1 expression that has been localized in the nonpigmented ciliary epithelium of human eyes.214,215,216 This enzyme catalyzes the conversion of cortisone to cortisol which, in turn, induces sodium and concomitant water transport into the posterior chamber, through epithelial sodium channels, including Na+-K+-ATPase,217,218 resulting in aqueous production. Levels of cortisol compared with cortisone in the aqueous humor are normally much greater than in the systemic circulation.219 However, long-term interactions of cortisol in the aqueous with glucocorticoid receptors in the trabecular meshwork could contribute to increasing outflow resistance in individuals susceptible to steroid-induced glaucoma (see section on Trabecular Outflow). Ingestion of the 11β-HSD antagonist carbenoxolone decreased IOP in normal214 and ocular hypertensive215 human eyes. The role of the other compounds within the aqueous is not understood.
Transforming growth factor (TGF) β2 is a component of normal aqueous humor detected in many mammalian eyes157,220,221,222,223 and may play a role in glaucoma pathogenesis. The intrinsic activity of TGF β2 is considered to be an important factor for the maintenance of the anterior chamber-associated immune deviation220,224 (see section on Aqueous Outflow).
As the aqueous flows from the posterior chamber to the anterior chamber, changes occur. Nutrients diffuse into the lens, iris, and vitreous.225 Diffusion from the posterior aqueous into the vitreous is a major contributor to the existence of concentration gradients of low-molecular weight substances in the vitreous.226 Waste products, such as lactate, diffuse from the lens, iris, and corneal endothelium into the aqueous. Some exchanges of small molecules occur across the iridial vessels. Predictably, the chemical compositions of posterior chamber aqueous and anterior chamber aqueous are different.120 To complicate the matter further, some substances appear to be actively transported out of the eye. Paraaminohippurate (PAH), diodrast, and penicillin are examples of large anions that are actively transported out of the eye. The system appears to be similar to that occurring in the renal tubules. This active transport system can be saturated and can also be inhibited by low temperatures and probenecid.1,120 The nonpigmented ciliary epithelium has been implicated as the site of this active transport system within the anterior eye. Another independent transport system actively excretes injected iodide from the aqueous. This latter system resembles iodide transport mechanisms in the thyroid and salivary glands.227 The significance to the normal physiology of the eye of these outward-directed transport systems has not been established. With the discovery that prostaglandins may be actively transported out of the eye,228,229 some have suggested that such mechanisms may be useful to rid the eye of biologically active substances no longer needed, or which may even be detrimental.41 Their removal from the eye to the blood facilitates their excretion via the hepatic route. There are other outwardly directed ion-uptake mechanisms present in the eye. The anterior uvea of the rabbit eye, for example, accumulates the anions cholate, glycocholate, deoxycholate, chenodeoxy-cholate, iodipamide, and o-iodohippurate.230,231
AQUEOUS FLOW
The result of all of the biochemical processes previously discussed is the production of a quantity of fluid that circulates continuously. Many of the biochemical changes caused by diffusion occur as the fluid moves from the posterior chamber, through the pupil, around the anterior chamber, and into the outflow system. Superimposed on this bulk flow is the anterior chamber thermal circulation, which causes the aqueous closer to the cooler avascular posterior cornea (cooled additionally by evaporation of tears from the corneal epithelium) to move downward, while the aqueous closer to the warmer vascular anterior iris moves upward. In addition, movements of the eyes and head modify these flow parameters.
In the human eye, the rate of aqueous formation is approximately 2.5 µL per minute. Because of the formation rate and aqueous chamber volumes in the human eye, approximately 3% of the posterior chamber volume and 1% of the anterior chamber volume are replaced per minute1,120 with the entire volume of the aqueous humor being replaced every 90 to 100 minutes.2 The more rapidly the aqueous is formed, the less is the potential for diffusional exchange with the ciliary processes, lens, anterior iris, and posterior cornea. However, within physiologic limits, changes in the rate of formation probably do not significantly affect the diffusional exchange. Furthermore, the rate of aqueous formation contributes to the regulation of IOP.
METHODS OF MEASURING RATES OF AQUEOUS FORMATION
In 1951, Goldmann232 first described a technique by which the rate of flow of aqueous humor in the eye could be quantified. This technique was based on the measurement of the kinetics of unbound fluorescein in the plasma and concomitant fluorescence in the anterior chamber after intravenous injection.3 Thereafter, other investigators devised techniques for the determination of aqueous flow, generally involving the cannulation of the anterior chamber with a needle, thus permitting drainage of aqueous or infusion of a fluid at a known rate.233,234,235,236,237,238,239 For example, one can inject into the anterior chamber a known amount of dye, radioactively labeled substance, or large molecule, the concentration of which is easily measured. If the substance mixes rapidly with all of the aqueous, repeated sampling of the fluid and measurement of the concentration provides an indirect measurement of bulk flow. The underlying assumption with this technique is that no change occurs in aqueous dynamics as a result of the injection or sampling technique. In practice such an assumption does not hold true, because the blood-aqueous barrier is breached by simple paracentesis.240 Furthermore, this technique assumes that none of the substance leaves the eye by diffusion or any other way except by direct bulk flow (which includes outflow via the uveoscleral pathway).
Later still, other techniques more applicable to the measurement of aqueous formation in the human eye were devised, which did not involve any invasive procedure.241,242,243,244,245,246,247 These methods, discussed in the following section, fall essentially into one of two categories: (1) measurement of the rate of appearance or disappearance of a chemical substance from the aqueous or (2) derivation of the aqueous formation rate from a mathematical formula (to be discussed) after obtaining measurements of the IOP, episcleral venous pressure, and resistance to aqueous outflow.1,120 Each method incorporates intrinsic advantages and disadvantages, and specific sources of error. However, in spite of this, there exists good agreement for the values of aqueous formation obtained, and in several different species.
MEASUREMENT OF FORMATION BY THE RATE OF APPEARANCE OR DISAPPEARANCE OF A CHEMICAL SUBSTANCE FROM THE AQUEOUS
It is possible to inject a substance such as PAH or fluorescein into the bloodstream and maintain a high concentration there. Over a period of several hours, a small but measurable amount diffuses into the aqueous humor and reaches an equilibrated concentration. The injection is then stopped, and the level of the fluorescein or PAH in the blood subsequently declines rapidly, owing to renal clearance. However, the concentration of the substance in the aqueous remains relatively constant over a short period, after which it starts to decrease, as fresh aqueous is formed not incorporating any PAH or fluorescein, because of low-plasma levels. The rate of fresh aqueous formation can be calculated by measuring the declining concentration either by sampling the aqueous first in one eye, then later in the second eye, as in the case of PAH, or by optical means using fluorophotometry, as in the case of fluorescein. Bárány and Kinsey248 developed this technique for PAH, and it was extended for use with fluorescein.246,249,250,251 The technique using fluorescein has been modified by dropping the fluorescein topically onto the eye rather than by injecting it.252,253 The dye in this case gains access to the anterior chamber via corneal absorption. However, there are inherent problems with this approach, specifically, the problem of measurement of fluorescence in the anterior chamber and cornea, and the deduction of aqueous flow from the change in fluorescence over time.3 The first problem was solved by the construction of a slit-lamp fluorometer.254,255 The second was addressed by several investigators who devised several new experimental approaches.50,248,256 Thus, despite the drawbacks of fluorophotometry using topically applied fluorescein, the technique has become the gold standard in studies involving the human eye. Jones and Maurice246 realized that the corneal stroma could serve as a depot from which fluorescein could be introduced slowly into the anterior chamber. This method clarified the important role of the cornea in affecting the kinetics of topically applied drugs and tracers. Maurice’s technique is now used most frequently for the measurement of the rate of aqueous formation in the human eye. The method involves the application of fluorescein topically to the eye, which subsequently penetrates the corneal epithelium and enters the stroma. Fluorescein is not metabolized by the eye and thus can disappear in only three ways: (1) rediffusion through the corneal epithelium and loss with the tears, (2) lateral diffusion into the limbal tissue, or (3) penetration of the endothelium and entrance into the aqueous humor, from where it is washed away by flowing aqueous, or is lost by diffusion into the iris (approximately 10% of fluorescein in the aqueous is lost by this route in the human eye).257 The third pathway of movement of fluorescein from the corneal stroma offers the least resistance, and thus is the major pathway of loss of fluorescein from the stroma.
The advantages of Maurice’s technique are that it is safe, repeatable, and objective. Studies of the human eye can span 18 to 24 hours after application of a single dose of fluorescein. The procedure disturbs the eye minimally, and the subject need not be constrained during the interval of measurement. Furthermore, the technique is reliable even when the rate of flow is not constant.3
In one variation of this technique, fluorescein is introduced into the stroma simply by applying drops topically to the inferior fornix of the conjunctiva.252,258 A waiting period of 6 hours or more allows the dye to become more uniformly distributed within the stroma. In another variation, fluorescein is applied by iontophoresis.246 This procedure involves the introduction of fluorescein into the anterior chamber by forcing it through the cornea via the application of a small electric current. Fluorescence is measured in the stroma and in the anterior chamber at the beginning and end of an interval. Flow is the clearance of the dye during the interval minus the diffusional loss. However, the technique is not applicable to eyes that lack an iridolenticular barrier between the anterior and posterior chambers. Furthermore, the technique measures only that portion of secreted aqueous that passes into the anterior chamber.3
McLaren259 developed a technique of measurement of aqueous flow based on flare. Flare (pathologic scattering of light resulting from the presence of protein in the aqueous resulting from inflammation and breakdown of the blood-aqueous barrier) was induced by argon laser photocoagulation of the iris in rabbits, and a scanning ocular spectrofluorophotometer was used to measure scattering in the anterior chamber. This method was used to study changes in aqueous flow over the diurnal cycle. A technique for the measurement of aqueous flow using corneal and vitreous depots of fluorescein in the rabbit eye has also been described.260,261 It may be concluded that (1) movement of water into or out of the vitreous can cause large changes in the rate of movement of dye from the vitreous to the anterior chamber and can make interpretation of the vitreous method ambiguous and (2) the vitreous method is probably superior for measuring sustained changes of the rate of aqueous flow over at least 10 hours, or perhaps several days, but it cannot be reliably used for measuring changes over shorter periods.
Similar types of studies have been performed using iodide.262 In all cases, it is assumed that the amount of substance leaving the eye by alternative routes is negligible compared with the dilution by fresh aqueous.
Using the method of Maurice and introducing fluorescein by iontophoresis, a value of 2.48 ± 0.17 µL per minute (mean ± standard error of the mean) was calculated for aqueous flow in the human eye.246 In all the techniques in which a fluorescent dye is used to measure aqueous flow, there are other potential confounding factors, such as binding of a proportion of the dye to ocular and/or plasma proteins that must be considered.263 However, under normal circumstances these factors do not compromise the measurements.
MATHEMATICAL DERIVATION OF THE AQUEOUS FORMATION RATE
The other major types of investigational tools used to estimate aqueous formation involve physical measurements. These methods depend on the following algebraic manipulation of the modified Goldmann equation describing IOP in terms of episcleral venous pressure (Pe), aqueous flow (Fin), trabecular outflow facility (Ctrab), and uveoscleral outflow (Fu):
IOP = Pe + ([Fin – Fu]/Ctrab)
Thus
▪ IOP – Pe = ([Fin – Fu]/Ctrab)
and
▪ Fin–Fu = Ctrab (IOP-Pe)
Therefore
▪ Fin = Ctrab (IOP-Pe) + Fu
In order to determine Ctrab and Fu, the eye in a living anesthetized animal may be cannulated with a needle and perfused with a solution of mock aqueous humor264 incorporating radiolabeled albumin (see later in this chapter).265,266 A value for IOP can be obtained by tonometry, or (in experimental animals) cannulation of the anterior chamber with connection via tubing to a pressure transducer. An estimate of Pe can be obtained in experimental animals by direct cannulation of an episcleral vein.267 Noninvasive determinations of Pe in humans and animals involve direct visualization and/or photographic methods to determine the pressure necessary to partially collapse an episcleral vein.268,269 (In practice these procedures would be repeated several times and a mean value calculated, because Pe is not constant throughout the entire episcleral venous system). By substitution into the above equation, Fin may be determined. Fin can also be calculated by the determination of the difference in radioactivity of a perfused radiolabeled solution before entering and after leaving the anterior chamber, the difference being related proportionally to total aqueous flow. However, these approaches are applicable only to experimental animals; their invasive nature makes them unsuitable for use in the human eye.
It is apparent that each of the foregoing methods has inherent errors and assumptions, yet despite this, the results indicate reasonable agreement among the various methods. The study of these methods has added much to the understanding of the factors that influence aqueous formation. In fact, it is not so much the absolute values themselves that are important but, rather, the ability to compare changes in values for aqueous formation under different conditions that has been most informative.
However, of all of these methods, noninvasive fluorophotometry has become the method of choice for the determination of the rate of flow of aqueous. A commercially available modern automated instrument (Fluorotron Master Ocular Fluorophotometer, Ocumetrics, Mountain View, CA) is typically used for the detection of ocular fluorescein levels in humans and animals.270,271,272
FACTORS AFFECTING AQUEOUS FORMATION
The rate of formation of aqueous is not constant. Variations in the formation rate occur hourly and daily.3 Knowledge concerning the cause(s) of this variation is particularly sparse. It is likely that many diverse physiologic systems, including the central nervous, endocrine, and cardiovascular systems, as well as changes in metabolic activity, all influence the production of aqueous.
Aqueous secretion also exhibits a diurnal cycle, decreasing by as much as 50% or more at night1,23,273,274 It is hypothesized that the diurnal cycle of the aqueous humor formation is regulated in part by a factors such as circulating catecholamines, epinephrine, and norepinephrine that have a circadian rhythm and partly by a factor that depends on the activity of the subject.273 Furthermore, the magnitude of the fluctuation in flow rate differs among different individuals.
The ciliary body is innervated by nerves arising from the long posterior and short ciliary nerves, which run parallel to the long posterior and short ciliary arteries. These nerve fibers are of both the myelinated and nonmyelinated variety. Parasympathetic fibers originate in the Edinger-Westphal nucleus of the third cranial nerve, run with the inferior division of this nerve in the orbit, and synapse in the ciliary ganglion.226 Sympathetic fibers synapse in the superior cervical ganglion and are distributed to the muscles and blood vessels of the ciliary body. Numerous unmyelinated nerve fibers surround the stromal vessels of the ciliary processes; these are most likely noradrenergic and subserve vasomotion.23 Sensory fibers arise from the ophthalmic division of the trigeminal nerve and enter the ciliary body, but their distribution and function have not been well studied. However, despite the distribution of nerves to the ciliary body, very little evidence for innervation of the ciliary epithelium itself has yet been found.4
β2-Adrenergic agonists are reported almost exclusively to increase aqueous secretion in primates. Topical epinephrine, norepinephrine, or isoproterenol stimulate secretion in the monkey eye,275,276 and topical epinephrine or terbutaline stimulate aqueous secretion in the human eye.277,278 Whether these processes work at the vascular level to change vascular tone or permeability or their effect is dependent on ciliary epithelial cell surface neurohumoral receptors associated with adenylate cyclase and/or guanylate cyclase activity has not yet been completely elucidated; however, an amassing body of evidence points to the latter.279,280,281,282,283,284,285,286,287,288,289,290,291,292,293,294,295,296
Timolol, a nonselective β-adrenergic antagonist, suppresses aqueous flow in both eyes of ketamine297 but not pentobarbital-anesthetized298 monkeys that have undergone unilateral superior cervical ganglionectomy, suggesting that the relevant β-receptors may be nonjunctional rather than postjunctional and that sympathetic neural tone to the ciliary body may play relatively little role in regulating the aqueous humor formation in the monkey. It is thus not entirely clear to what extent aqueous secretion is under neuronal versus humoral adrenergic control. It is questioned whether β-adrenergic antagonists suppress aqueous humor formation via their effect on ciliary epithelial β2-adrenergic receptors.32,279,281,299,300 There is evidence that classical β-adrenergic receptor blockade may not be involved, and that other receptor types such as 5HT1A may be relevant.301
The α2-adrenoceptor agonists apraclonidine and brimonidine are reported to lower aqueous secretion and IOP in cats, rabbits, monkeys,302,303,304 and humans.305 The effect is thought to be mediated via a postjunctional or nonjunctional α2 receptors present on the membrane of the nonpigmented ciliary epithelium304 but may in part be centrally mediated via imidazoline receptors in some species.306 The effect in monkeys is not abolished by superior cervical ganglionectomy,304 indicating that intact sympathetic innervation is not required for the drugs to lower secretion and IOP. However, intact sympathetic innervation is required for a response to the α2-adrenoceptor agonists clonidine in rabbits307 or brimonidine in cats and rabbits.302 The lack of aqueous flow suppression by brimonidine in pentobarbital-anesthetized monkeys may reflect the suppression of neural and humoral catecholaminergic tone by this anesthetic,308 especially relative to ketamine, which elevates such tone.309
The effects of cholinergic drugs on aqueous humor formation and composition, and on the blood-aqueous barrier, are unclear, with conflicting results arising from various studies. In general, cholinergic drugs cause vasodilation310,311,312 resulting in increased blood flow to the iris, ciliary processes, and ciliary muscle.312,313 The presence of flare (Tyndall effect, indicating increased protein concentration) and/or the detection of cells in the aqueous humor by biomicroscopy indicates that these agents can also cause breakdown in the blood-aqueous barrier.314 Cholinergic agents or parasympathetic nerve stimulation have been reported to increase, decrease, or not alter the aqueous humor formation rate and to slightly increase the episcleral venous pressure.315,316,317,318,319,320,321,322,323 The minimal effect on the rate of aqueous humor formation and episcleral venous pressure are clearly not responsible for the drug-induced decrease in IOP that results from the cholinergic therapy.
Aqueous formation varies directly with the blood pressure in the internal carotid-ophthalmic arterial system in the primate276 but only when mean arterial blood pressure is altered artificially to a physiologically abnormal extent below 70 to 90 mm Hg. For example, ligation of the internal carotid artery causes a profound drop in aqueous secretion. However, formation is not significantly altered by changes in blood pressure within the normal physiologic range for any given species. Ciliary blood flow likely delivers oxygen that is required to sustain the active ionic transport that drives aqueous humor production. Insufficient delivery of oxygen, as occurs when ciliary perfusion is less than 74% of baseline, would compromise aqueous humor production.324
Aqueous formation rate diminishes slightly with age. After the age of approximately 10 years, formation declines by 3.2% to 3.5% per decade.3 The mechanism underlying this decrease is unknown. An age-dependent loss of ciliary epithelial cells has not been described. Some authors have demonstrated a 5.8% loss of trabecular cells per decade in humans,186,325,326 whereas others have reported a loss of corneal endothelial cells at the rate of 3.5% per decade.327 Brubaker3 suggested that the age dependency of the population of ciliary epithelial cells should be studied, because if it is found that aqueous formation parallels the number of secreting cells, it would suggest that although aqueous formation may depend on neuronal or hormonal stimulation, the normal rate of formation may depend on cell count. Alternatively, the decline in aqueous formation could be a result of the changes observed in the fine structure of aging ciliary epithelial cells.328 Hypothermia leads to a decrease in aqueous formation, for example, a drop in body temperature of 7° C (about 19%) leads to approximately a 50% reduction in secretion, reflecting the deactivation of metabolic processes necessary to maintain active secretion.41
The ultrafiltration component of aqueous humor formation is pressure-sensitive, decreasing with increasing IOP. This phenomenon is quantifiable and is termed as pseudofacility because a pressure-sensitive decrease in inflow appears as an increase in the outflow facility when techniques such as tonography and constant pressure perfusion are used to measure outflow facility.235,236,329,330,331,332,333,334 Although some sensory nerve endings exist in the ciliary body, they do not appear to be of the pressure-sensitive variety.4 The initiating event of this pressure-induced response of the ciliary processes remains obscure. Bill and Bárány235 reported that an artificially induced rise in IOP caused a reduction in secretion. This has been confirmed in the monkey.335 An intracameral injection of erythrocytes yielded a partial blockade of the trabecular meshwork, and hence an elevation in IOP. This led to a suppression of aqueous secretion, corresponding to 0.06 µL/min/mm Hg increase in pressure. Therefore with a normal secretion rate in the pentobarbital anesthetized cynomolgus monkey of about 1 µL per minute,336 an increase in IOP of 20 mm Hg should theoretically suppress aqueous secretion altogether. However, this does not in fact occur. It is well established that secretion continues, even against very high pressures. Increased IOP does decrease the blood flow in the ciliary body and may decrease secretion in this manner.331,337,338 In addition to the acute effect of elevated IOP, some patients in the late stages of glaucoma may show hyposecretion and even have normal pressures despite almost totally occluded outflow channels.339 It is not known if this is due to the same mechanism as the acute type of pressure-related hyposecretion. However, there is evidence that much of the perceived reduction in the aqueous secretion in response to increased IOP is caused by measurement artifact235,236,265,335,338,340 and that the real magnitude of pseudofacility in the monkey is less than 0.02 µL/min/mm Hg or less than 5% of total facility.236,341
A decrease in aqueous secretion occurs in association with uveitis, especially uveitis involving the ciliary body epithelium (iridocyclitis). A reduction in IOP is also seen clinically and experimentally in the monkey eye, perhaps mediated by prostaglandin release,342 and probably caused mainly to an increase in uveoscleral outflow rather than to a reduction in aqueous secretion.342,343 Other clinical conditions associated with decreased aqueous production include retinal, choroidal, or ciliary body detachment (Table 6.2).
There are hormonal influences on aqueous secretion. Adrenalectomy in experimental animals leads to a decrease in aqueous formation, probably due to the resultant sharp decrease in the levels of circulating glucocorticoids or epinephrine.1,120 However, in a study of patients who had undergone adrenalectomy,344 it was concluded that both the circadian rhythm of aqueous flow and the daytime response to timolol persist in the absence of the adrenal glands. There was no correlation between endogenous progesterone levels and aqueous humor flow or IOP during the menstrual cycle of 20 healthy, nonpregnant women.345
Decreased plasma osmolality causes an increase in IOP and aqueous formation.346,347 Although aqueous formation is probably increased by an increase in water carried across the ciliary epithelium by the Na+ pump, the IOP increase is primarily the result of water gain to the eye by diffusion from the blood to the vitreous, and probably the aqueous as well.1 This test was utilized at one time for diagnosis of open-angle glaucoma (the water drinking test). However, the effect was not specifically diagnostic for glaucoma and has been abandoned by most ophthalmologists.339 Similarly, increased plasma osmolality (as obtained by administering the hyperosmotic agents mannitol, isosorbide, or glycerine) causes a profound decrease in IOP, primarily because of water movement from vitreous to blood and only secondarily to a decrease in aqueous formation.346,348,349 Some authors report little effect of hemodialysis-reduced plasma osmolality on IOP.350
Other pharmacologic agents are known to decrease aqueous formation, and thus IOP have already been mentioned including β-adrenoceptor antagonists351 such as timolol,352,353,354 betaxolol,355 and others291,356,357,358,359,360,361,362,363 as well as CAIs.40,87,364,365,366,367,368,369,370,371,372
Certain vasodilator substances also reduce aqueous secretion, including the cardiac peptide atrial natriuretic factor (ANF),373 which also reportedly stimulates an intracellular particulate guanylate cyclase and raises the levels of cyclic guanosine monophosphate (cGMP) in the ciliary epithelium.292,296,374,375
In addition, certain of the nitrovasodilators, which are also known to mediate an increase in intracellular cGMP (via activation of a soluble guanylate cyclase), reduce aqueous secretion, including sodium nitroprusside,296,376 sodium azide,296 and nitroglycerin.294 However, Krupin and colleagues377 found that topical sodium nitroprusside or sodium azide increased aqueous secretion in human volunteers. This discrepancy may be dose related.378 Nitrovasodilators may also lower the IOP by enhancing aqueous humor outflow (see Outflow section).379,380,381 The cGMP itself also affects aqueous humor dynamics, for example, intravitreal injection of 8-bromo cGMP in the monkey promotes a reduction in aqueous flow of 15% to 20% and, at higher doses, an increase in outflow facility by 25% to 30%.382 A reduction in aqueous flow in rabbits in response to topical 8-bromo cGMP has also been described.383 Systemic administration of the nitric oxide synthase inhibitor Nw-nitro-L-arginine methyl ester (L-NAME) results in ciliary vasoconstriction that decreases ciliary blood flow and aqueous humor flow in rabbits.271 Other vasoactive drugs, such as the calcium channel antagonists verapamil and nifedipine,384 reportedly reduce aqueous secretion in rabbits. However, topical diltiazem and verapamil increased secretion and IOP in human volunteers.385
The serotonergic antagonist ketanserin reduces the rate of secretion of aqueous in rabbits, cats, and monkeys.386,387 The serotonergic agonist serotonin sometimes reduces the rate of secretion.387 Serotonergic receptors of a 5-HT1A—like subtype have been reported to exist in the iris/ciliary body of rabbits and humans.388,389 The serotonergic agonist flesinoxan has been found to decrease IOP and possibly aqueous secretion in rabbits.390 However, a significant increase in aqueous secretion, but no effect on IOP, was found in monkeys that had been treated with the 5-HT agonist 8-hydroxy-2(di-n-propylaminotetralin) (8-OH-DPAT), indicating the possible presence of a secretion-stimulating 5-HT1A receptor in monkey ciliary epithelium.391 It has been suggested that these receptors may be effectively antagonized by timolol and other β-blockers. Species differences may well account for the conflicting nature of these data, and furthermore, the precise nature of the putative 5-HT1A—like receptor subtype is still in question.388,389
Agonists at the 5-HT2 receptors have been identified as effective ocular hypotensive agents in the primate experimental glaucoma model.392,393 The ocular hypotensive response observed with 5-HT2 receptor antagonists in monkeys386 and humans394,395 may be mediated via pathways not related to their 5-HT2 antagonist activity. It was reported that neither 5-HT1A agonists nor 5-HT2 antagonists decreased IOP in the monkey with laser-induced ocular hypertension.392 R-DOI [R(-)-2-(4-iodo-2,5-dimethoxyphenyl)-2-aminopropane], a selective 5-HT2 agonist, causes a small but significant increase in aqueous humor formation and lowers IOP in normotensive monkeys primarily by increasing uveoscleral outflow.396 The magnitude of the ocular hypotensive response and increase in uveoscleral outflow as well as the slight increase in aqueous humor formation produced by R-DOI are similar to the responses observed with PGF2α-isopropyl ester in monkeys.138,140,397 The fact that functional 5-HT2 receptors have been found in human ciliary muscle and trabecular meshwork cells offers a plausible explanation for the IOP lowering action of R-DOI.398,399
Studies suggest that dopamine (DA2 and DA3) receptors play a role in the aqueous humor secretion. The presence of such receptors in ocular structures remains to be shown definitively, and specific binding of [3H]-spiroperidol to membrane fractions of rabbit ICB has not been demonstrated.400 However, there is evidence, based on adenylate cyclase activation studies, to suggest that there are DA1-receptors in the ciliary body of the bovine and human eye but not in the rodent or rabbit eye.401 The topical administration of dopamine DA2 agonists a DA3 agonist and a DA2/Da3 agonist to rabbits reduces secretion.402,403,404,405 However, this may not represent a local action of the drugs, because IOP is reduced in both eyes after unilateral administration. In contrast, the DA2 agonist, bromocriptine, does not reduce secretion in normal monkeys.406 The ability of these drugs to reduce secretion in the rabbit is blocked by superior cervical ganglionectomy or by pretreatment with a DA2 or DA3 receptor antagonist. These findings suggest that the most likely sites of action are the DA2 and DA3 receptors located on sympathetic nerve endings or ganglia.407 The activation of these receptors has an inhibitory effect on the release of norepinephrine.408 Both orally and topically administered bromocriptine lowers the IOP of human volunteers.409,410,411 The DA2 antagonist haloperidol administered topically lowers the IOP of normotensive rabbits by suppression of aqueous formation.412,413
α1-Adrenoceptor antagonists414,415,416 reportedly reduce secretion rate in rabbits but only by a very modest amount in humans. Unilateral instillation of an antagonist with α1-adrenoceptor selectivity417 reduces IOP in normal rabbits and monkeys, but no change in either outflow facility or aqueous flow was observed in monkeys.418
Certain α2-adrenoceptor agonists are much more effective at reducing the secretion rate and are used clinically, such as apraclonidine419,420,421,422,423,424,425 and brimonidine.302,303,425,426 Selective silencing of α and β adrenergic receptors can reduce IOP.427,428
Purine nucleotides are emerging as relevant to ocular physiology.162,429 Within the eye, nucleotides can exert either an increase in IOP or a decrease depending on the P2 receptor that is stimulated.430 P2Y2 receptors have been found in the ciliary body431,432,433 as well as in the trabecular meshwork.434,435 Patients with POAG present increased levels of nucleotides in their aqueous humors.436,437 The high concentration of nucleotides in glaucoma patients suggests that elevated levels of nucleotides may be responsible for the elevated IOP by activating the P2Y2 receptors. Agonists of the P2Y2 receptor can elevate IOP in rabbits. Conversely, small interfering RNA (siRNA) against the mRNA for the P2Y2 receptors in rabbits produced a profound and long lasting reduction in IOP.438 The use of the siRNA against the P2Y2 receptor may be of interest as new therapeutic approaches to treat the abnormal elevation in IOP present in many glaucoma patients. Adenosine A3 antagonists can alter aqueous humor formation by preventing adenosine-induced activation of chloride channels in human nonpigmented ciliary epithelial cells.58
The circulating renin-angiotensin system is an important determinant in the maintenance of adequate systemic blood pressure and may also be involved in organ-specific blood flow. All recognized renin-angiotensin system components have been identified in the eyes of humans and other species. Angiotensin converting enzyme (ACE) is present in human and rabbit aqueous humor439,440,441 and also in the feline ciliary body.442 Furthermore, angiotensinogen (a precursor of angiotensin I) is present in the nonpigmented ciliary epithelium of the human eye, more in the pars plana than in the pars plicata.443 Angiotensinogen was also found in the blood vessel lumina of the uvea and retina.443 Both the pigmented and nonpigmented layers of the human ciliary epithelium contain prorenin, the prohormone of renin,444 more so in the pars plicata than in the pars plana region.445 ACE inhibitors reduce aqueous secretion when applied topically to rabbit eyes.446 Topical application of 0.1% SCH 33861 reduces aqueous secretion in glaucoma patients, although it is less effective than 0.5% timolol.447 In humans, the oral angiotensin I receptor antagonist, losartan increases outflow facility and decreases the aqueous humor formation.448 However, there has been no successful drug development with this strategy thus far. In addition to the circulatory renin-angiotensin system, there is a tissue-localized system. Local angiotensin II formation can be catalyzed by renin-independent or ACE-independent pathways via chymase or cathepsin G.449 A recently discovered ACE2 can degrade angiotensin II to biologically active angiotensin 1-7, which acts oppositely to angiotensin II via a novel angiotensin receptor type, Mas receptor.450 Angiotensin 1-7 decrease IOP within 1 to 5 hours after intravitreal administration to rabbits, possibly by decreasing the aqueous humor formation.451 Conversely, angiotensin II can decrease outflow facility in monkey eyes.452
Only gold members can continue reading. Log In or Register to continue