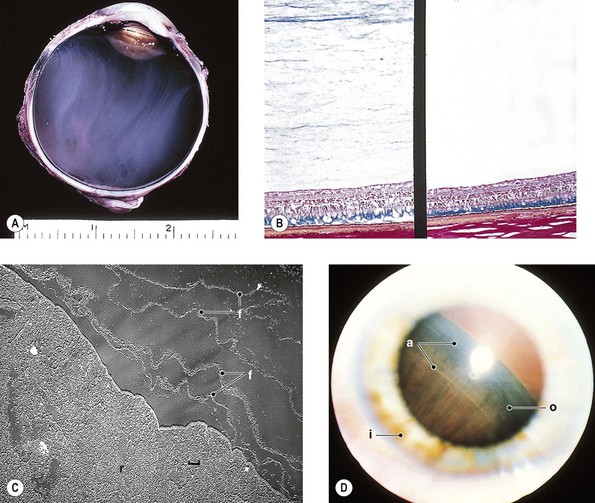
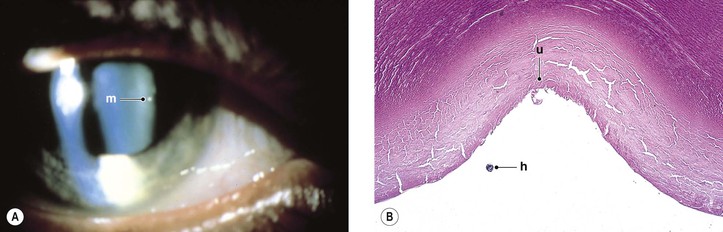
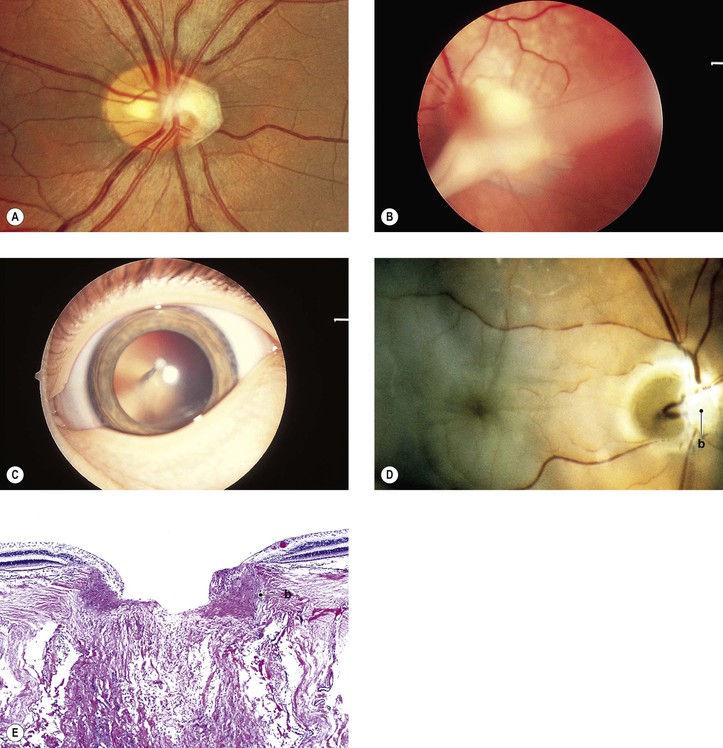
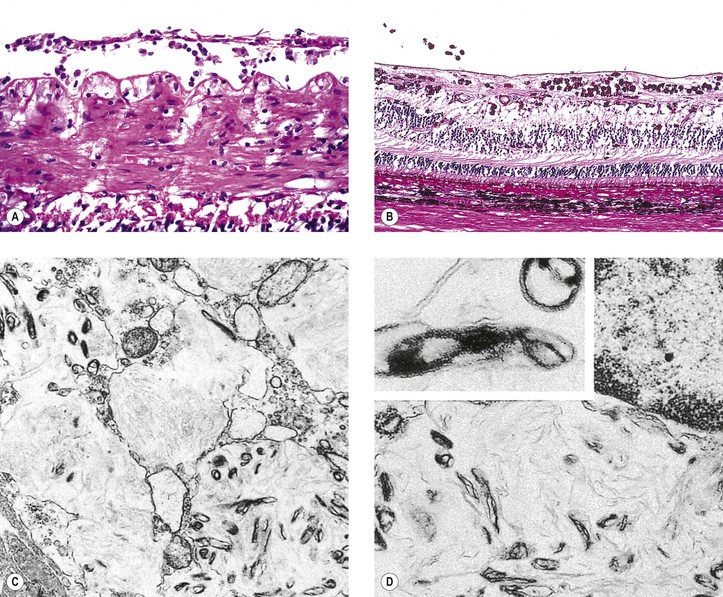
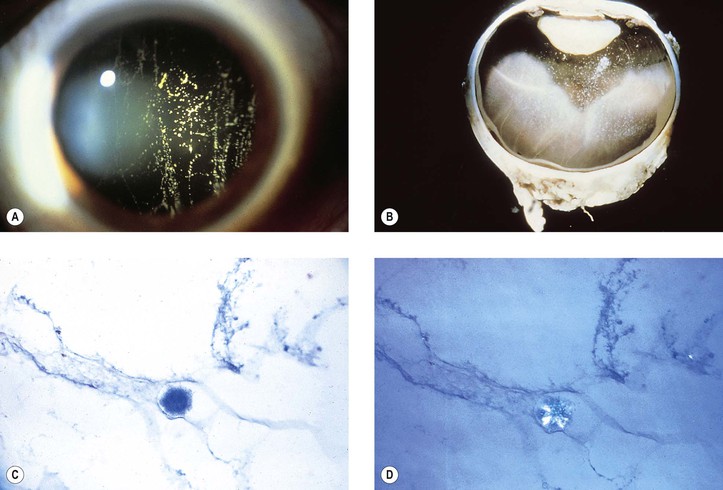
I. The transparent vitreous body, or hyaloid (Fig. 12.1), is one of the most delicate connective tissues in the body. II. Embryology B. The hyaloid vessel, which atrophies and disappears before birth, passes through the canal. C. Persisting remnants of the primary vitreous or hyaloid vessel produce congenital anomalies (see later), the most common being retention of tissue fragments on the back of the lens (Mittendorf’s dot; Fig. 12.2), retention of tissue on the nasal optic disc (Bergmeister’s papilla), and persistent primary vitreous (see Chapter 18). A. Anterior remnants (see Fig. 12.2; see also Fig. 9.3) B. Posterior remnants (Fig. 12.3) 1. Vascular loops from the optic disc may remain within Cloquet’s canal. II. Posterior (congenital retinal septum; ablatio falciformis congenita) A. Posterior persistent hyperplastic primary vitreous (PHPV; see Fig. 12.3) is most often unilateral and present at birth. Poor vision and strabismus are the most common presenting complaints. I. Vitreocorneal adhesions may cause corneal “touch” syndrome (see Fig. 5.5). B. The cornea becomes thickened and edematous in the region of touch. III. Cyclovitreal adhesions may lead to a cyclitic membrane and subsequent neural retinal detachment. IV. Vitreoretinal adhesions may lead to the macular vitreous traction syndrome (cystoid macular edema; Irvine–Gass syndrome; see Chapter 5) or to wrinkling of the internal limiting membrane, namely “cellophane” retina (see Figs. 11.43–11.45). Idiopathic vitreous adhesions may follow partial vitreoretinal separation (posterior vitreous detachment). Muscae volitantes are minute remnants of the hyaloid vascular system or detachments of small folds of poorly differentiated retinal tissue, usually present in the anterior vitreous. II. Separation of the vitreous attachment to the optic disc after posterior vitreoretinal separation may cause a complete or incomplete ringlike floater (vitreous “peephole”; see subsection on vitreous detachment, later). III. Symptomatic degenerative vitreous floaters may have a negative impact on the quality of life. II. Whitish masses (“white balls”) may be seen inferiorly with vitreitis (e.g., sarcoidosis). III. Numerous vitreous opacities, foamy “Whipple” macrophages, may be found in persons with Whipple’s disease (Fig. 12.4). A. Whipple’s disease is a disorder of men, usually older than 35 years of age. C. Ocular findings, in addition to vitreous opacities, include inflammations and ophthalmoplegia. D. Foamy macrophages containing periodic acid–Schiff (PAS)-positive cytoplasm may be found in intestinal and rectal mucosa, mesenteric and extra-abdominal lymphatic tissue, heart, lungs, liver, adrenals, spleen, serous membranes, neural retina, and vitreous. I. Red blood cells in the vitreous compartment (see Figs. 12.11 and 12.12) are most often caused by neural retinal tears but may have other causes. Red blood cells may be subvitreal (between vitreous body and internal limiting membrane of the neural retina) or intravitreal (within the vitreous body). II. Hypoxia of the vitreous body may be demonstrated when blood enters it in a patient who has sickle-cell trait or disease.
Vitreous
Normal Anatomy
Congenital Anomalies
Persistent Primary Vitreous
Persistent Hyperplastic Primary Vitreous (Persistent Fetal Vasculature)
Vitreous Adhesions
Post Nonsurgical and Surgical Trauma
Idiopathic
Vitreous Opacities
Hyaloid Vessel Remnants
Acquired Vitreous Strands and Floaters
Inflammatory Cells
Red Blood Cells

Vitreous
12