II. Endophthalmitis (Fig. 3.1) is an inflammation of one or more coats of the eye and adjacent cavities. III. Panophthalmitis (Fig. 3.2) is an inflammation of all three coats of the eye (and adjacent cavities); it often starts as an endophthalmitis that then involves the sclera and spreads to orbital structures. I. Exogenous C. Postoperative suppurative inflammation in the first day or two after surgery is usually purulent, fulminating, and caused by bacteria. 2. A bacterial infection is also a possible cause of delayed endophthalmitis, especially with less virulent bacteria such as Staphylococcus epidermidis and Propionibacterium acnes (see Chapter 5). II. Endogenous Suppurative inflammation is characterized by a polymorphonuclear leukocytic infiltrate (Figs. 3.3 and 3.4). Tissue necrosis causes a suppurative or purulent exudate (pus). I. Behçet’s disease (see Fig. 3.3) is a chronic endogenous endophthalmitis. D. Plasminogen activator levels may be decreased. E. A hypercoagulable or general vascular endothelial dysfunction is usually found. H. The ocular inflammation is characterized by recurrent iridocyclitis and hypopyon (often motile), usually involving both eyes but not necessarily simultaneously. 2. Small patches of retinal whitening are characteristic. 4. Rarely, a bilateral immune corneal ring (Wessely ring) may occur. I. Biopsy of mucocutaneous lesions shows vasculitis. L. Histologically, the main process appears to be a small or moderate-sized blood vessel obliterative and necrotizing vasculitis. 3. A secondary chronic nongranulomatous inflammatory infiltrate is frequently noted in adjacent tissues (see Fig. 3.4). I. Exogenous: The inflammation is usually secondary to trauma. II. Endogenous (Fig. 3.5) B. The inflammation may be associated with viral infections such as rubella and subacute sclerosing panencephalitis (SSPE); bacterial infections such as syphilis; local ocular (nonsystemic) entities such as pars planitis, Fuchs’ heterochromic iridocyclitis, uveal effusion (see Chapter 9), and glaucomatocyclitic crisis (Posner–Schlossman syndrome; see Chapter 16); and systemic diseases such as Reiter’s syndrome, Behçet’s disease (see earlier), Kawasaki’s disease (mucocutaneous lymph node syndrome), phacoanaphylactic endophthalmitis (the uvea usually shows a chronic, nongranulomatous uveitis; see Chapter 4), collagen vascular disease (including rheumatoid arthritis), Crohn’s disease (regional enteritis; see later in this chapter), ulcerative colitis, and Whipple’s disease (see Chapter 12); and atopy. C. A history of cigarette smoking is a significant risk factor. I. Viral infections such as herpes simplex and zoster, Epstein–Barr virus (EBV), SSPE, rubella (see Chapter 2), and rubeola may cause an endogenous nonsuppurative, chronic nongranulomatous uveitis. A. Herpes simplex virus (HSV; Fig. 3.6) 1. HSV consists of a linear, double-stranded DNA packaged in an icosahedral capsid and covered by a lipid-containing membrane. 2. Neonatal HSV most commonly causes a nonfollicular conjunctivitis followed by keratitis. 3. Acquired HSV in children and adults is similar to that in neonates. a. A mucocutaneous eruption is common. c. The most common ocular manifestation is keratitis (see Chapter 8). 4. Histologically, the infected area reveals both acute and chronic nongranulomatous inflammation. a. Intranuclear inclusions (Cowdry type A) may be seen. b.
Nongranulomatous Inflammation
Uveitis, Endophthalmitis, Panophthalmitis, and Sequelae
Classification
Terminology
Suppurative Endophthalmitis and Panophthalmitis
Clinical Features
Classification
Histology
Examples
Nonsuppurative, Chronic Nongranulomatous Uveitis and Endophthalmitis
Clinical Features
Classification
Examples
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Nongranulomatous Inflammation
3
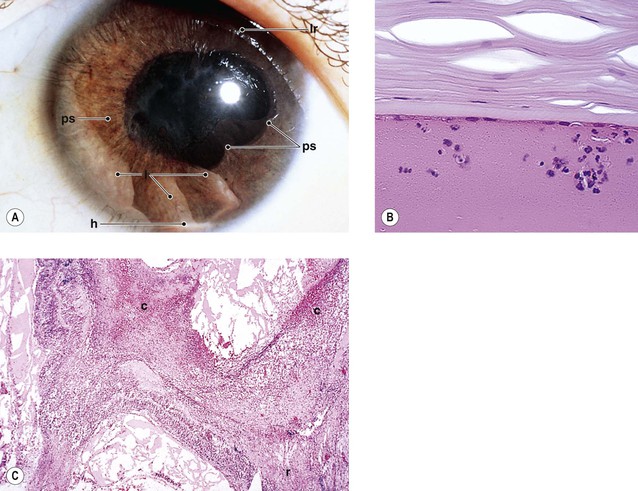
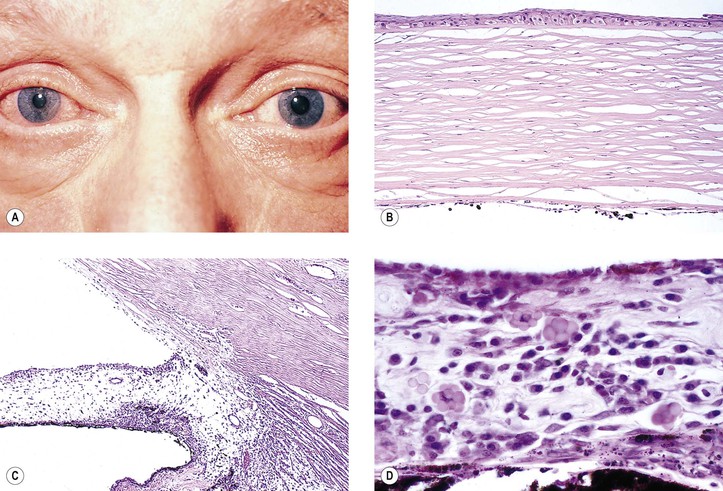
Fig. 3.4 Suppurative endophthalmitis (see also Fig. 3.1). A, Suppurative inflammation present in area of perforating corneal ulcer and in hypopyon in anterior chamber. Iris contains chronic nongranulomatous inflammatory infiltrate of lymphocytes and plasma cells. B, Polymorphonuclear leukocytes (PMNs) in hypopyon shown with increased magnification. C, Edge of corneal ulcer shown in A demonstrates corneal necrosis, PMNs seen as a lining-up of nuclear particles along stromal lamellae, and “smudgy” areas that represent bacterial colonies (seen as gram-positive cocci with special stain in D).