Introduction
The last three decades of the twentieth century saw an explosion of interest in the vitreous because of the development of vitreoretinal surgery. Prior to this period, large numbers of patients were blinded by inoperable vitreoretinal diseases. One goal of this chapter is to help the medical student, intern, resident, general ophthalmologist and optometrist become aware of the indications for vitreoretinal surgery, many of which are time sensitive. Many vitreoretinal conditions have implications for the family medical practitioner, internist, and emergency physician.
Vitreous Anatomy and Its Relevance to Pathology
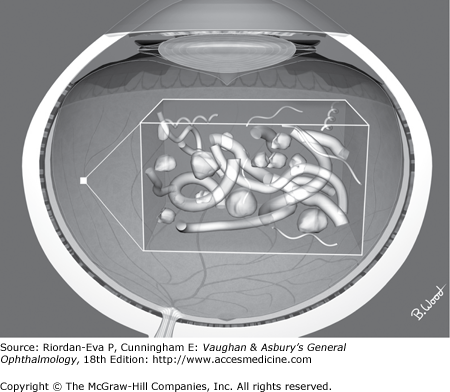
The vitreous fills the space between the lens and the retina and consists of a three-dimensional collagen fiber matrix and a hyaluronan gel (Figure 9–1). (The older term, “vitreous humor” is less commonly used today.) The outer surface of the vitreous, known as the cortex, is in contact with the lens (anterior vitreous cortex) and adherent in varying degrees to the surface of the retina (posterior vitreous cortex) (Figure 9–2).
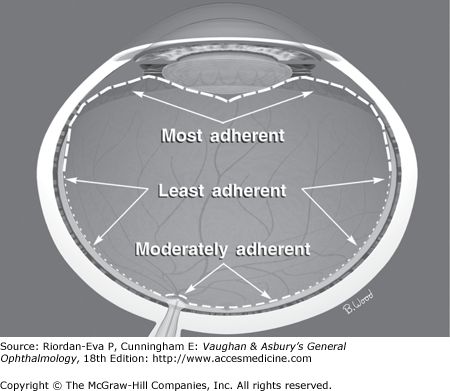
Aging, hemorrhage, inflammation, trauma, myopia, and other processes often cause hypocellular contraction of the vitreous collagen matrix. The posterior vitreous cortex then separates from areas of low adherence to the retina and may produce traction on areas of greater adherence. The vitreous base extends from the equator anteriorly and is a zone of great adherence. The vitreous virtually never detaches from the vitreous base. The vitreous is also adherent to the optic nerve and, to a lesser extent, the macula and retinal vessels. Adherence to the macular region is a significant factor in the pathogenesis of epimacular membrane, macular hole, and vitreomacular traction syndrome.
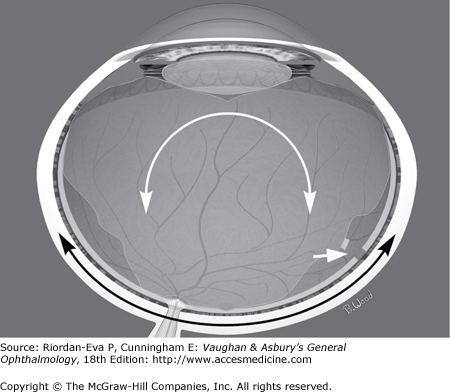
Previously it was taught that the vitreous developed cavities from a process known as syneresis, ultimately resulting in “collapse” of the vitreous. It is now believed that collagen cross-linking and selective loss of retinal adherence rather than cavity formation are the primary events. Even though the vitreous may migrate inferiorly when separated from the retina, this process causes less force at the zones of vitreoretinal adherence than the traction caused by saccadic eye motion. Saccadically induced, dynamic forces play a significant role in the development of retinal breaks (tears), damage to the retinal surface, and bleeding from torn vessels (Figure 9–3). Further contraction of the vitreous caused by invasion of retinal pigment epithelial, glial, or inflammatory cells may result in sufficient static traction to detach the retina without retinal tears.
Prior to vitreoretinal surgery, vitreous “bands” were thought to cause traction on the retina, and largely unsuccessful attempts were made to cut them with scissors. The visualization provided by vitreoretinal endoillumination systems has contributed to our knowledge of anatomy and demonstrated that these bands are contiguous with the transparent posterior vitreous cortex that is also responsible for substantial traction. Traction bands virtually only exist when penetrating trauma creates a path through the vitreous or from severe necrosis, usually due to toxocariasis. Even these bands are usually contiguous with the posterior vitreous cortex.
Examination of the Vitreous and Vitreoretinal Interface
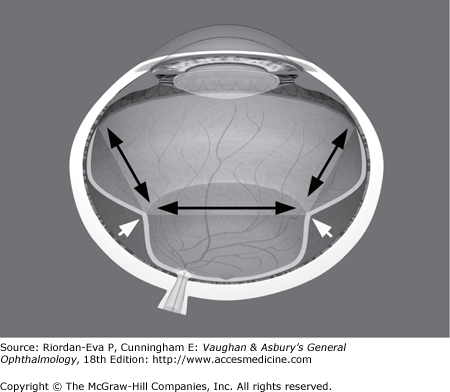
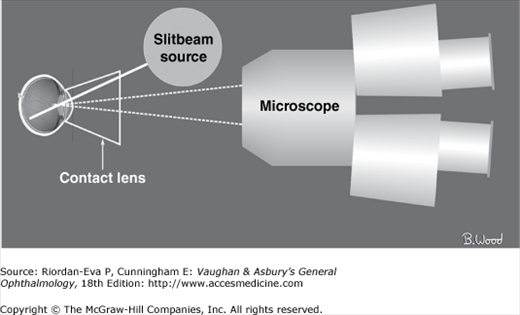
Normal vitreous is essentially transparent, yet it is capable of producing substantial force on the retina. Vitreoretinal traction can often be inferred by the configuration of the retinal surface (Figure 9–4). Transparent vitreous can best be seen by using a narrow, off-axis, slitbeam, a three-mirror contact lens, and a stereo biomicroscope (Figure 9–5). Visualization is significantly enhanced by dark adaptation of the observer. A biomicroscope with a broad, on-axis, slitbeam or a direct ophthalmoscope is usually not suitable for observing the vitreous.
Indirect ophthalmoscopes provide a large field of view, are capable of looking “around” some lenticular and vitreous opacities, and provide a stereoscopic view. Many observers only attempt to look “through” the vitreous, ignoring the opportunity to look “at” the vitreous, especially if it is abnormal. Visualization of vitreoretinal traction is enhanced rather than adversely affected by eye motion. In addition, mobility of the vitreous is an excellent gauge of the extent of vitreoretinal traction. It is often possible to see some portion of the retina in eyes with substantial vitreous hemorrhages by looking at the periphery first to establish a plane of focus, but the viewing path though semi-opaque vitreous is much less in the periphery than when attempting to visualize the optic nerve. The vitreous is often clearer superiorly. Sitting the patient up for a period of time may cause blood to migrate inferiorly, enabling a better view of the retina.
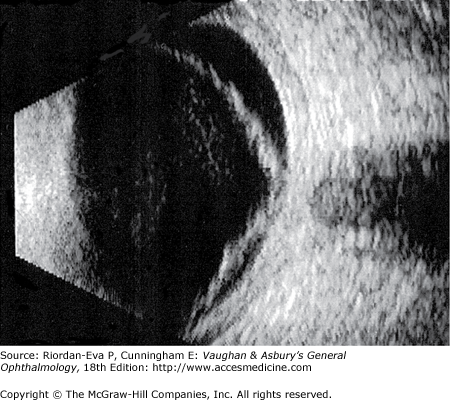
If the vitreous is too opaque to see the retina, B-scan ultrasonography should be used to determine if the retina is attached or a tumor, foreign body, dislocated lens, dislocated intraocular lens, or choroidal detachment is present (Figure 9–6).
Optical coherence tomography (OCT) utilizes light to construct a 3-D model of the macula and posterior retina from a series of optical B-scan images (see Chapter 2). Spectral domain OCT with tracking produces much better resolution than time domain OCT. The resolution is approximately 5 microns. OCT is ideal for visualization of vitreomacular traction, epimacular membranes, macular holes, macular cysts, macular edema, subretinal fluid, pigment epithelial detachments and choroidal neovascular membranes.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


