Purpose
To investigate whether the enhanced depth imaging technique (EDI) may improve the visualization of the lamina cribrosa using spectral-domain optical coherence tomography (SD-OCT).
Design
Prospective observational case series.
Methods
Images of the optic nerve were obtained in 10 normal subjects, 7 glaucoma suspects, and 18 glaucoma patients by positioning an SD-OCT in the usual fashion, as well as close enough to the eye to obtain an inverted representation of the fundus (EDI). In addition to these single line scans, approximately 65 sections were obtained within a 10 × 15-degree rectangle covering the optic nerve head using EDI. The “depth of signal” was measured as the distance from the optic cup surface and the point where the signal ended in both single line scan images.
Results
Compared to the image obtained with the SD-OCT used in the usual fashion, images obtained with EDI provided larger depth of signal (728.04 ± 124.20 vs 368.79 ± 75.15 μm, P < .001) below the optic cup surface and better image contrast from the deep optic nerve; this facilitated the discrimination of the lamina cribrosa. In the en face image, the lamina cribrosa was visualized as a highly reflective plate containing multiple pores that corresponded with the color fundus photographs.
Conclusion
Using EDI SD-OCT, the full-thickness lamina cribrosa was clearly visualized in all eyes examined. This technique should facilitate the investigation on the lamina cribrosa in glaucoma, and may provide additional insight into the pathogenesis of glaucomatous optic neuropathy.
The lamina cribrosa is considered to be the primary site of axonal injury in glaucoma. The deformation and compression of the lamina cribrosa are thought to promote optic neuropathy by a blockade of axoplasmic flow within the optic nerve fibers. It has been a challenge to evaluate the deformation of the lamina cribrosa in patients.
A number of recent reports suggest that spectral-domain optical coherence tomography (SD-OCT) imaging of the human optic nerve head can capture the lamina cribrosa. Inoue and associates measured the lamina cribrosa thickness of living glaucoma patients on the 3-dimensional (3D) images using 3D imaging software. However, 42% of their study eyes were excluded from the analysis because the lamina cribrosa could not be clearly identified, either because of poor image contrast or because of the vascular shadowing that obscured the lamina cribrosa. Strouthidis and associates compared serial optic nerve head histology with interpolated B-scans generated from a 3D SD-OCT optic nerve head volume acquired in vivo from the same normal monkey eye. Using this method, they were able to delineate the anterior lamina surface. However, the posterior surface of the lamina cribrosa was not detectable as the signal faded with increasing depth through the optic nerve.
Recently, a new imaging technique, enhanced depth imaging (EDI) OCT, has been described by Spaide and associates. This technique was originally developed to visualize the full thickness of the choroid and involves positioning the SD-OCT device close enough to the eye to obtain an inverted representation of the fundus.
The purpose of the present study was to investigate whether the EDI technique improves the visualization of the lamina cribrosa using SD-OCT.
Methods
This investigation is based on the Lamina Cribrosa Exploration Study, an ongoing prospective study of glaucoma and healthy individuals at the Glaucoma Clinic of Seoul National University Bundang Hospital. The subjects were either invited to participate in the study at the clinic visit or recruited by advertisement.
Primary open-angle glaucoma was defined as the presence of glaucomatous optic nerve damage (ie, vertical cup-to-disc ratio of 0.7 or greater, or asymmetry 0.2 or more, or the presence of focal thinning, notching, and disc hemorrhage) and associated visual field defect without ocular disease or conditions that may elevate the intraocular pressure. A glaucomatous visual field change was defined as 1) outside normal limit on glaucoma hemifield test; or 2) 3 abnormal points with P < 5% probability of being normal, 1 with P < 1% by pattern deviation; or 3) pattern standard deviation of 5% if the visual field was otherwise normal, confirmed on 2 consecutive tests. Glaucoma suspect was defined as either the ocular hypertension (intraocular pressure >21 mm Hg) or the presence of glaucomatous optic nerve head damage without visual field defect. Normal eyes were defined when they have intraocular pressure below 22 mm Hg, normal visual fields, and normal-appearing optic discs.
To be included, subjects were required to have a best-corrected visual acuity of ≥20/200, spherical refraction within ±6.0 diopters and cylinder correction within ±3.0 diopters, and clear ocular media (up to grade 3 for nuclear opalescence, nuclear color, and cortical changes (NO1-3, NC1-3, C1-3) and up to grade 2 for posterior subcapsular change (P1-2) on LOCS III (Lens Opacities Classification System III). Eyes with optic nerve diseases other than glaucoma, including optic disc drusen or anterior ischemic optic neuropathy, retinal diseases such as retinal vessel occlusion or diabetic retinopathy, and neurologic diseases such as pituitary tumor, were excluded. Eyes were also excluded if they had a history of ocular surgery other than cataract extraction or glaucoma surgery or if a good-quality image (ie, quality score >15) could not be obtained from them.
Optic Disc Scan Using OCT
The optic discs of the subjects were evaluated by Spectralis OCT (Heidelberg Engineering GmbH, Heidelberg, Germany) using both conventional method and EDI. The principle and detail of the EDI technique is described elsewhere. In brief, the device was positioned close enough to the eye to create an inverted image near the top of the display. Enough separation from the top of the display was used to avoid image ambiguity from image folding with respect to zero depth.
Subjects were imaged through undilated pupils. A single line scan was first obtained at the central optic disc. Then, a single line scan using EDI technique was obtained at the same location, which was enabled by repeat mode of Spectralis OCT. In addition, a 10 × 15-degree rectangle covering the optic disc was scanned by the EDI technique with approximately 65 sections, which were 30 to 34 μm apart (the slicing distance is determined automatically by the machine). Scanning was performed with 42 frames averaged.
A 3D volumetric image was reconstructed from the B-scan images obtained using 3D imaging software (Amira 5.2.2, Visage Imaging, Berlin, Germany). En face images were generated at the prelaminar, laminar, and retrolaminar level.
Measurement of Signal Depth
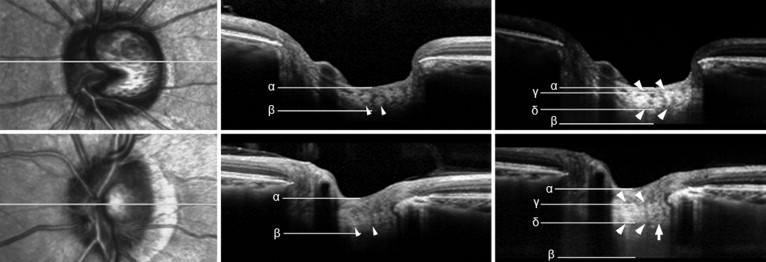
The distance from the optic cup surface to the point where the signal ended was measured in the single line scan images to determine the “depth of signal” ( Figure 1 ). Difference in the depth of signal between the 2 imaging methods was assessed using paired t test.
Measurement of Prelaminar Tissue and Lamina Cribrosa Thickness
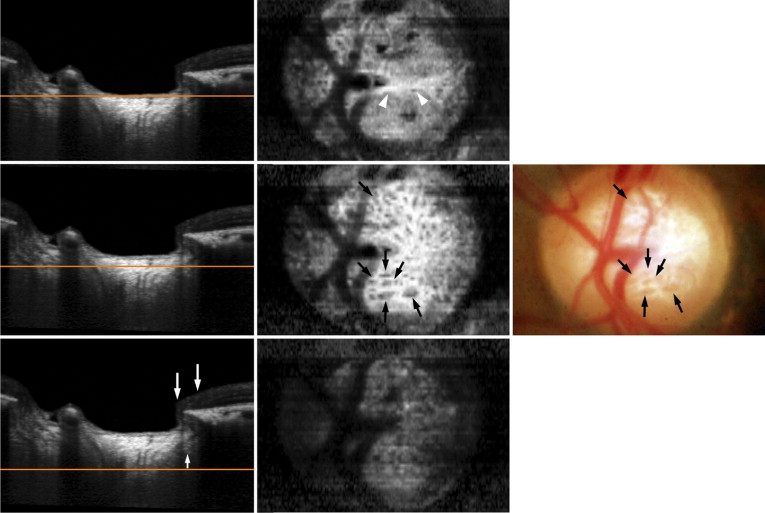
The thicknesses of the prelaminar and the laminar tissue were measured on the B-scan images obtained with EDI. The measurement points were determined as centrally on the optic nerve as possible where there is the least likelihood of vascular shadows, because thick retinal vessels cause shadows in axial images that prevent visualization of optic nerve head structures underlying the vessels. The prelaminar tissue thickness was defined as the distance between the optic cup surface and the anterior border of the highly reflective region that corresponds to the lamina cribrosa (see below). The thickness of the lamina cribrosa was defined as the distance between the anterior and the posterior borders of the highly reflective region ( Figure 1 ). When the anterior or posterior border of the lamina cribrosa was not definite on B-scan image, the borders were determined by examining the en face images ( Figure 2 ). The thicknesses were measured using a manual caliper tool of the Amira 5.2.2 software.
To evaluate the interobserver reproducibility of our measuring method, 15 randomly selected SD-OCT datasets were evaluated by 2 examiners (E.J.L. and T.W.K.) and the intraclass correlation coefficient (ICC) was calculated. According to Fleiss and associates, scores ≥0.75, between 0.40 and 0.75, and ≤0.4 are termed as excellent, moderate, and poor, respectively.
Results
This study initially involved 36 subjects. Of these, 1 subject was excluded because of poor cooperation (severe eye movement) during image acquisition. The mean age of the remaining 35 subjects was 51.8 ± 16.9 years with a range of 22 to 75 years. The mean visual acuity measured 0.8 ± 0.3 (range, 0.1 to 1.0) and the mean refractive error (spherical equivalent) was −0.67 ± 1.92 diopters (range, −6.0 to 3.75 diopters). The mean intraocular pressure was 16.2 ± 7.6 mm Hg. The mean central corneal thickness was 552.7 ± 46.1 μm and the visual field mean deviation was −2.73 ± 5.71 dB (range, −21.99 to 1.61 dB).
Compared to the image obtained with the SD-OCT used in the usual fashion, images obtained with the EDI technique provided more abundant signal and better image contrast in the deep portion of the optic nerve head ( Figure 1 ). The depth of signal was significantly larger in images obtained with the EDI technique than those obtained in the usual fashion (728.04 ± 124.20 vs 368.79 ± 75.15 μm, P < .001). On B-scan images, the lamina cribrosa was visualized as a highly reflective layer, as was demonstrated in previous studies. On the en face cross-sectional images through the lamina cribrosa, multiple low-reflectivity dots that corresponded to lamina pores shown in the color fundus photographs were visualized ( Figure 2 ).The prelaminar and retrolaminar tissue was shown to be more homogenous with less reflectivity than the lamina cribrosa ( Figure 2 ). Although the lamina was more readily recognizable below the optic nerve cup, it was also possible to delineate the lamina beneath the neuroretinal rim ( Figures 1 through 3 ). The mean thickness of the prelaminar tissue and the lamina cribrosa was 102.24 ± 31.28 μm (range, 65.0 to 196.0 μm) and 235.42 ± 66.47 μm (range, 143.0 to 420.0 μm), respectively. There was good interobserver reproducibility in measurement of thicknesses of the prelaminar neural tissue and the lamina cribrosa (intraclass correlation coefficient = 0.965 and 0.861, 95% limit of agreement = −118.1 to 46.1 μm and −65.2 to 51.5 μm, respectively).
Table 1 shows the thickness measurements in each group. The difference of the lamina cribrosa among 3 groups was statistically significant ( P = .047, 1-way analysis of variance). In the post hoc analysis, normal eyes showed significantly thicker lamina cribrosa than glaucomatous eyes (254.80 ± 69.31 μm and 215.67 ± 58.26 μm, respectively, Dunnett’s test).
| Normal Subjects (n = 10) | Glaucoma Suspects (n = 7) | Glaucoma Patients (n = 18) | P Value b | Post Hoc | |
|---|---|---|---|---|---|
| Prelaminar thickness (μm) | 111.43 ± 34.98 | 93.83 ± 18.74 | 95.70 ± 28.46 | .092 | |
| Laminar thickness (μm) | 254.80 ± 69.31 | 242.67 ± 68.02 | 215.67 ± 58.26 | .047 | Normal subjects > glaucoma patients |
a When both eyes were eligible, only 1 eye was randomly selected.
b Comparison was performed using 1-way analysis of variance.
Table 2 shows the symmetry analysis between fellow eyes for each group. There was no significant difference between right and left eyes in any group.
| Normal Subjects (n = 10) | Right Eye | Left Eye | P Value |
|---|---|---|---|
| Prelaminar thickness (μm) | 114.75 ± 29.11 | 115.67 ± 46.05 | .928 |
| Laminar thickness (μm) | 273.0 ± 81.31 | 242.58 ± 66.05 | .194 |
| Glaucoma Suspects (n = 7) | Right Eye | Left Eye | P Value |
|---|---|---|---|
| Prelaminar thickness (μm) | 82.50 ± 9.71 | 87.25 ± 8.18 | .531 |
| Laminar thickness (μm) | 233.25 ± 36.63 | 218.0 ± 44.11 | .570 |
| Glaucoma Patients (n = 18) | Eye With Higher Mean Deviation | Eye With Lower Mean Deviation | P Value |
|---|---|---|---|
| Prelaminar thickness (μm) | 93.33 ± 20.66 | 98.60 ± 33.64 | .449 |
| Laminar thickness (μm) | 219.47 ± 55.66 | 210.87 ± 62.64 | .316 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


