Purpose
To determine the natural course of lamellar macular holes (MHs) in highly myopic eyes.
Design
Prospective and observational case series.
Methods
Twenty-four eyes of 21 consecutive patients with a lamellar MH and high myopia (myopic refractive error >8 diopters or axial length ≥26.5 mm) were followed for ≥12 months. The changes of the optical coherence tomography (OCT) findings and the best-corrected visual acuity (BCVA) were analyzed. The progression of the lamellar MH to a full-thickness MH and the change of the BCVA were analyzed.
Results
At the initial examination, an epiretinal membrane was identified by OCT in 17 of the 24 eyes (70.8%) and 7 eyes (29.2%) had macular retinoschisis. Twenty-three of 24 eyes (95.8%) did not show any changes of the lamellar MH in the OCT images during a mean follow-up of 19.2 ± 10.2 months. However, the remaining eye progressed to a full-thickness MH and pars plana vitrectomy was required to close the MH. Except for this 1 eye, the BCVA was maintained (within 0.2 logMAR change) during the follow-up period of at least 1 year.
Conclusions
A lamellar MH in highly myopic eyes is a relatively stable condition.
Lamellar macular holes (lamellar MHS) were first described by Gass in 1976 to be a complication of chronic cystoid macular edema that developed after cataract extraction. The differentiation of a lamellar MH from pseudo MHs or full-thickness MHs has been greatly enhanced by the findings of optical coherence tomography (OCT). The OCT criteria of lamellar MHs are a break of the inner layers of the fovea, an intraretinal split, an irregular foveal contour, and a thin and irregular fovea. A lamellar MH most likely develops from an aborted formation of a full-thickness MH, although tomographic studies of the natural history of lamellar MHs are limited. Theodossiadis and associates examined the natural course of 41 patients with a lamellar MH (mean refractive error; −0.45 diopter [D]) and reported that the best-corrected visual acuity (BCVA) was stable in 78% and decreased in 22% of patients with a mean follow-up of 37.1 months. However, the foveal thickness decreased and the diameter of the lamellar MH increased slightly. Takahashi and Kishi reported 2 patients with a lamellar MH that progressed to full-thickness MH, and they suggested that lamellar MHs form when the inner wall of a superficial split or cyst in the neurosensory retina at the fovea is avulsed by vitreous traction.
It is difficult to follow the natural course of a lamellar MH in highly myopic eyes because it is difficult to identify a lamellar MH by ophthalmoscopy and because of the intense red reflex of the thin retina and coexisting myopic fundus lesions, for example, macular chorioretinal atrophy or choroidal neovascularization. Studies on lamellar MHs in highly myopic eyes are limited, and these studies have been mainly related to macular retinoschisis (MRS). Thus, Panozzo and associates reviewed the medical records and OCT findings of 218 highly myopic eyes in 121 consecutive patients and reported that a lamellar MH was observed in only 6 eyes (4.8%) by OCT.
Detailed characteristics and natural history of lamellar MHs in highly myopic eyes have not been published. Because it has been reported that a full-thickness MH is difficult to close in highly myopic eyes, it is important to know the natural history of lamellar MHs and the incidence of lamellar MHs that progress to full-thickness MHs in highly myopic patients.
Thus, the purpose of this study was to prospectively investigate the natural history of lamellar MHs in highly myopic eyes. We followed 24 highly myopic eyes of 21 patients for at least 1 year without any intervention, and we shall show that 95.8% of the eyes did not show any progression in the lamellar MH in the OCT images. In addition, the BCVA did not decrease significantly over this 1-year period. Thus, a lamellar MH in highly myopic eyes is relatively stable and surgery should be undertaken only if other findings indicate a course different from the natural course.
Patients and Methods
Twenty-one consecutive highly myopic patients (24 eyes) with a lamellar MH who visited the High Myopia Clinic at Tokyo Medical and Dental University from September 2006 through May 2009 were enrolled.
The inclusion criteria were: 1) myopic refractive error (spherical equivalent) ≥8.0 D or axial length ≥26.5 mm; 2) presence of a lamellar MH by OCT; and 3) minimum follow-up period of 1 year. Patients with a history of intraocular surgery in the study eye were excluded. Patients received a comprehensive ocular examination, including measurements of the BCVA, refractive error (spherical equivalent), axial length, dilated ophthalmoscopy with macular examinations with a contact lens or a 90-diopter lens, color fundus photography, and OCT. The BCVA was determined by a Landolt C chart, and the decimal BCVAs were converted to the logarithm of minimal angle of resolution (logMAR) units for statistical analyses. OCT examinations were performed through a dilated pupil using the Cirrus OCT (Carl Zeiss Meditec, Jena, Germany) with a scan length of about 8 mm. These examinations were performed every 3 months, even if there were no changes in the BCVA and visual symptoms.
A lamellar MH was diagnosed based on the OCT findings and was based on the criteria of Witkin and associates: 1) irregular foveal contour, 2) break in the inner fovea, 3) separation of the inner from the outer foveal retinal layers leading to an intraretinal split, and 4) absence of a full-thickness foveal defect with intact photoreceptors posterior to the area of the foveal dehiscence.
For statistical analyses, the significance of the differences was determined by the Mann-Whitney U tests. A P value <.05 was considered statistically significant.
Results
There were 3 men and 18 women who met the inclusion criteria. None of the patients dropped out during the follow-up period. The mean age of the patients at entry was 59.0 ± 11.0 years (range, 38 to 79 years). The mean refractive error was −15.5 ± 4.5 D (range, −9.0 to −26.0 D) and the mean axial length was 30.2 ± 1.5 mm (range, 26.8 to 32.9 mm). The mean follow-up period was 19.2 ± 10.2 months with a range of 12 to 44 months. All of the eyes had a posterior staphyloma. The Weiss ring was not observed in any of the 24 eyes ophthalmoscopically. The OCT images showed that all of the eyes met the criteria for a lamellar MH as reported by Witkin and associates. An epiretinal membrane was identified by OCT in 17 of the 24 eyes (70.8%). Seven of the 24 eyes (29.2%) had macular retinoschisis; however, a foveal retinal detachment or vitreomacular traction was not identified in any of the eyes in the OCT images.
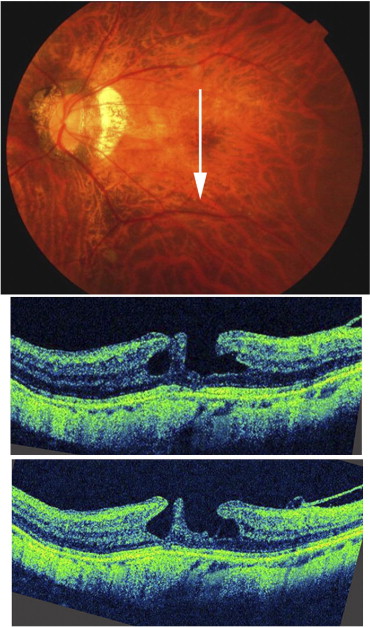
Twenty-three of 24 eyes (95.8%) did not show any changes of the lamellar MHs by OCT during the follow-up period ( Figure 1 ). However, the remaining eye progressed to a full-thickness MH and had decreased vision at 17 months after the initial examination ( Figure 2 ). This patient did not develop an MRS during the follow-up. Pars plana vitrectomy with gas tamponade was performed on this patient and the MH was closed. Except for this 1 eye that developed a full-thickness MH, the BCVA in the other 23 eyes remained at the baseline level during the follow-up ( Figure 3 ). The BCVA was 0.12 ± 0.16 logMAR units (range, −0.18 to 0.40 logMAR units) at the initial visit and was 0.12 ± 0.17 logMAR units (range, −0.18 to 0.52 logMAR units) at the final visit. This difference between initial and final BCVA was not significant (paired t test, P = .695).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


