Purpose
To describe the visual outcomes and volumetric magnetic resonance imaging (3D MRI) in children with neurofibromatosis type 1 (NF1) and orbitotemporal plexiform neurofibromas.
Design
Multicenter retrospective case series.
Methods
Two institutions with dedicated NF1 clinical research programs queried their established clinical databases for children with orbitotemporal plexiform neurofibromas. Visual acuity, refractive error, ambylopia, and treatment history were abstracted. Extent of orbitotemporal plexiform neurofibroma involvement was assessed clinically and with 3D MRI analysis. Children with optic pathway gliomas or ocular causes of decreased visual acuity (ie, cataracts, glaucoma) other than strabismus or anisometropia were excluded.
Results
Twenty-one children met inclusion criteria (median age 8 years, range 0.33-23 years). Orbitotemporal plexiform neurofibroma location was classified as isolated eyelid (n = 6), eyelid and orbit (n = 7), orbit and temporal region (n = 7), or diffuse orbit (n = 1). Three subjects had bilateral orbital involvement. Amblyopia secondary to the orbitotemporal plexiform neurofibroma was present in 13 subjects (62%) and was caused by strabismus (n = 2, 10%), occlusion from ptosis (n = 9, 43%), or anisometropia (n = 9, 43%), or a combination of factors (n = 6, 29%). MRI-derived volumes were measured in 19 subjects (median 41.8 mL, range 2.7-754 mL). All subjects with amblyopia had orbitotemporal plexiform neurofibroma volumes greater than 10 mL.
Conclusion
In our series, amblyopia occurs in more than half of NF1 children with orbitotemporal plexiform neurofibromas, most commonly because of ptosis and anisometropia. The 3D MRI analysis allowed for sensitive measurement of orbitotemporal plexiform neurofibroma size, and larger volumes were associated with development of amblyopia.
Neurofibromatosis type 1 (NF1) is a multisystem genetic disorder occurring in approximately 1:3000 births. Although optic pathway gliomas are the most common ophthalmologic condition in children with NF1, plexiform neurofibromas that infiltrate the orbit, temporal region, and/or eyelids, termed orbitotemporal neurofibromas, are less common but potentially vision threatening. Most orbitotemporal neurofibromas are believed to be congenital, grow during early childhood, and have the potential to become malignant in a small number of cases. Orbitotemporal neurofibromas can cause strabismus and proptosis, alter globe length, and obscure the visual axis secondary to infiltration and edema of the orbit and eyelids—putting young children at risk for amblyopia.
Most research on orbitotemporal neurofibromas has focused on the surgical treatment, primarily in adult cohorts, rather than visual outcomes in young children at risk for amblyopia. Long-term success of surgical resection and ptosis repair is reduced by the potential for recurrence of orbitotemporal neurofibromas, especially in young children. Recurrence of incompletely resected orbitotemporal neurofibromas is now better understood as it is likely a result of the inflammatory environment created by surgery, resulting in increased recruitment of mast cells.
We describe the visual outcomes associated with orbitotemporal neurofibromas and propose initial guidelines for the evaluation and management of orbitotemporal neurofibromas in children.
Methods
Patients
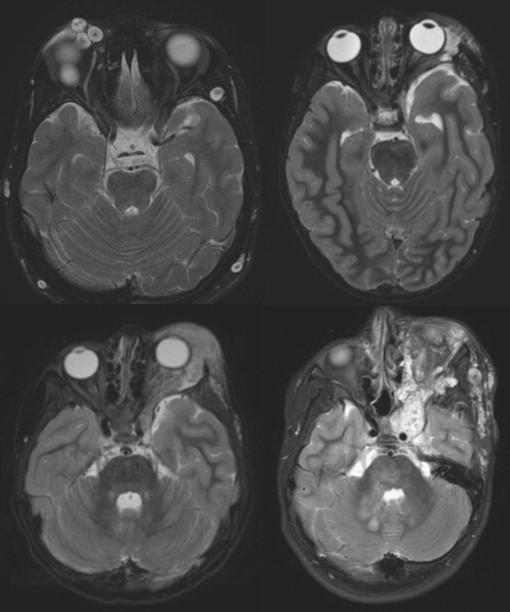
The NF1 clinical research programs at Children’s National Medical Center (Washington, DC) and the Pediatric Oncology Branch of the National Cancer Institute (Bethesda, Maryland) performed a retrospective case study by querying their established NF1 clinical databases for children who met the following criteria: confirmed orbitotemporal neurofibromas by neuroimaging (magnetic resonance imaging [MRI]/computed tomography) and ophthalmologic records. Children with optic pathway gliomas or ocular causes of decreased visual acuity (ie, cataracts, glaucoma) other than strabismus or anisometropia were excluded. Those subjects meeting inclusion criteria had the following data abstracted from their first visit’s clinical chart onto a standardized data form: visual acuity (VA), refractive error, presence of amblyopia, and treatment (medical or surgical) history for their orbitotemporal neurofibromas. Amblyopia was defined as a greater than or equal to a 0.2 logarithm of the minimal angle of resolution (logMAR) difference in the age-based VA and attributed to strabismus, occlusion from ptosis, and/or anisometropia, defined as greater than 1.5 diopters (D) myopia, 2.5 D hyperopia, or 1.5 D astigmatism. Amblyopia treatment was defined as any intervention aimed at improving VA or alignment such as patching, atropine drops, or surgical repair of strabismus. Orbitotemporal neurofibroma location was classified as isolated eyelid, eyelid and orbit, orbit and temporal region, or diffuse orbit ( Figure 1 ). Treatment indications included amblyopia, cosmetic appearance, exposure keratopathy, or a combination of factors.
The Institutional Review Boards from both institutions approved the clinical databases used in the study. All subjects provided written consent to allow their protected health information to be included in the database. No identifying information was exchanged between institutions.
Volumetric Magnetic Resonance Imaging Analysis
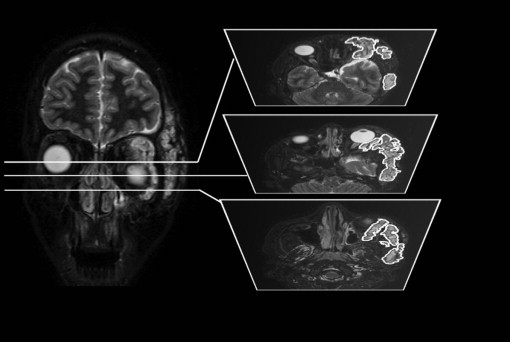
Extent of orbitotemporal neurofibromas was assessed clinically and with MRI, including volumetric MRI (3D MRI) analysis, if feasible; 3D MRI analysis was performed as previously described using MEDx (Medical Numerics Inc, Germantown, Maryland). For each MRI image, the tumor is roughly outlined manually, including a rim of low-signal-intensity normal tissue, followed by automated histogram analysis of signal intensity pixel by pixel, definition of threshold that distinguishes high-signal-intensity tumor from normal tissue, and determination of tumor contours ( Figure 2 ).
Statistical Analysis
Demographic and clinical characteristics were summarized by descriptive summaries (eg, means and standard deviations for continuous variables such as age and percentages for categorical variables such as sex). Wilcoxon rank sum was used to compare variables between eyes affected by orbitotemporal neurofibromas and unaffected eyes. Spearman rank correlation determined the relationship between orbitotemporal neurofibroma volumes and magnitude of amblyopia (logMAR).
Results
Twenty-eight children with NF1 and orbitotemporal neurofibromas were identified (median age 8 years at first evaluation, range 0.33-23 years). Seven subjects were excluded for coexistent optic pathway glioma (n = 6) or glaucoma (n = 1), resulting in 21 evaluable subjects. Ten of 21 subjects (48%) were female; 2 subjects were African American, 1 subject was of multiple races, and 18 were white. Discovery of orbitotemporal neurofibromas occurred between birth and 5 years of age, with most being diagnosed within the first 2 years of life. Thirteen subjects experienced amblyopia (mean = 0.5 logMAR difference, range 0.2-1.5 logMAR). Fifteen subjects received corrective eyewear, of which 14 of 15 (93%) were for myopia. The amount of spherical refractive error was greater for the orbitotemporal neurofibroma eyes (median −2.63 D, range −10.00 to +1.50) compared with the unaffected eye (median = −0.125 D, range −7.25 to +1.50; P = .025). The amount of astigmatism affected by orbitotemporal neurofibromas (median = 0.875 D, range 0.00 to 6.00) was slightly greater but not statistically different than the unaffected eyes (median = 0.25 D, range 0.00 to 1.25; P = .063).
Table 1 lists the location of orbitotemporal neurofibromas, etiology of amblyopia, type, and indication for treatment. The locations of orbitotemporal neurofibromas were fairly well distributed, although diffuse orbital infiltration occurred in 1 of 21 cases (5%). The etiology of amblyopia occurred most commonly from ptosis (9/21; 43%) or anisometropia (9/21; 43%), although a combination of multiple factors (6/21; 29%) frequently contributed. Treatment of orbitotemporal neurofibromas most commonly occurred because of amblyopia (7/21; 33%), followed by cosmetic appearance (4/21; 19%).
| Subjects (N = 21) | |
|---|---|
| Location of OTPN, no. (%) | |
| Isolated eyelid | 6 (29) |
| Eyelid and orbit a | 7 (33) |
| Orbit and temporal region | 7 (33) |
| Diffuse orbit | 1 (5) |
| Etiology of ambylopia, no. (%) | 13 (62) |
| Strabismus | 2 (10) |
| Occlusion from ptosis | 9 (43) |
| Anisometropia | 9 (43) |
| Multiple etiologies | 6 (29) |
| Treatment for OTPN, no. (%) | 9 (43) |
| Ptosis surgery | 2 (22) |
| OTPN removal from eyelid | 3 (33) |
| Enucleation | 2 (22) |
| Medication b | 4 (44) |
| Reasons for treatment, no. (%) c | 9 (43) |
| Amblyopia | 7 (33) |
| Cosmetic appearance | 4 (19) |
| Exposure keratopathy | 1 (5) |
a Three subjects had bilateral involvement.
b Some attempted medication in combination with surgery.
MRI-derived orbitotemporal neurofibroma volumes were measured in 19 subjects (median 39.9 mL, range 2.7-754 mL), with 1 subject contributing volumes from bilateral orbitotemporal neurofibromas ( Table 2 ). Subjects with amblyopia had a greater orbitotemporal neurofibroma volume (median 41.8 mL, range 12.8-754.0) compared with those without vision loss (median 9 mL, range 2.7-66.7), although this did not reach statistical significance ( P = .074). All 13 subjects with amblyopia had orbitotemporal neurofibroma volumes greater than 10 mL, compared with 3 of 7 subjects without amblyopia ( Figure 3 ). Despite the differences in groups, the correlation between orbitotemporal neurofibroma volume and amount of vision loss (logMAR difference from normal) did not reach statistical significance (r = 0.259, P > .2).
| Subject | Age (y) | Right Eye Refraction (D) a | Left Eye Refraction (D) a | logMAR Difference b | Affected Eye c | MRI Volume (mL) |
|---|---|---|---|---|---|---|
| 1 | 8 | 0.75 + 0.75 | −1.00 + 1.00 | 0.4 | Left | 18.9 |
| 2 | 1 | −0.25 + 0.00 | −3.00 + 0.50 | 0.2 | Left | 19.4 |
| 3 | 2 | −0.75 + 1.00 | −1.50 + 1.25 | 0.0 | Left | 8.1 |
| 4 | 0.3 | 1.50 + 0.00 | 1.50 + 0.00 | 0.0 | Left | — d |
| 5 | 11 | −1.00 + 1.50 | 0.00 + 0.75 | 0.3 | Right | 17.4 |
| 6 | 2 | −2.25 + 1.00 | −2.25 + 1.00 | 0.0 | Left | 48.0 |
| 7 | 8 | 0.50 + 0.00 | 0.50 + 0.00 | 0.0 | Left | 55.2 |
| 8 | 7 | — | 0.50 + 0.00 | 1.5 | Right | 53.2 |
| 9 | 13 | 0.00 + 0.00 | −6.00 + 0.50 | 0.2 | Left | 315 |
| 10 | 17 | 0.00 + 0.00 | −10.00 + 0.00 | 1.4 | Left | 81.2 |
| 11 | 18 | −3.25 + 0.00 | −5.00 + 0.50 | 0.2 | Left | 754.0 |
| 12 | 11 | −6.50 + 1.25 | −6.25 + 0.25 | 0.2 | Left | 299.0 |
| 13 | 12 | −0.50 + 0.50 | −2.25 + 3.50 | 0.2 | Left | 400.0 |
| 14 | 23 | 0.00 + 0.00 | 0.00 + 0.00 | 0.0 | Right/left | 7.4/2.7 |
| 15 | 18 | −7.00 + 1.00 | −7.25 + 0.75 | 0.0 | Right | 9.0 |
| 16 | 5 | 1.50 + 0.00 | 1.50 + 0.00 | 0.5 | Left | 14.2 |
| 17 | 18 | −0.75 + 1.25 | −0.50 + 0.50 | 0.0 | Left | — d |
| 18 | 9 | 0.00 + 0.00 | 0.00 + 0.00 | 0.2 | Left | 41.8 |
| 19 | 1 | −1.00 + 0.75 | 1.25 + 0.00 | 0.1 | Right | 66.7 |
| 20 | 3 | 0.00 + 0.00 | −3.00 + 6.00 | 0.6 | Left | 36.6 |
| 21 | 2 | 2.25 + 0.00 | −2.50 + 7.25 | 0.8 | Left | 33.8 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


