Vision Rehabilitation
Joel A. Kraut
Low vision is increasingly a problem in our society today and will continue to be so in the future.1 Low vision refers to a range of visual conditions between normal vision and blindness. Low vision indicates that the vision is not normal and the word vision implies that the person is not blind.2 These visual problems will likely increase as citizens in developed countries live longer, develop age-related changes in their eyes, or suffer trauma or illness that may create many visual problems. In addition, many low birth-weight children survive today and will comprise another growing population with visual problems, which will have an impact not only on the individual patients but also on society in general, which increasingly deals with health care on both local and national levels.
This loss of vision can result from decreased visual acuity or visual field caused by pathology of the eye or brain.3 This loss of vision can be congenital, develop early in life, be acquired secondary to trauma, or accompany systemic disease or aging. Age-related ophthalmic diseases and subsequent vision loss affect function to a varying degree among our growing older population. Many of these patients have treatable diseases and it is important to make certain that they have access to professional eye care. Although most patients with significantly decreased vision are older, vision rehabilitation may benefit children as well.
Low vision rehabilitation is an area that actively involves only a small number of eye care professionals. There is a long history of rehabilitation in the field of physical medicine with regard to trauma, stroke, as well as cardiac and orthopedic problems; it is equally important to develop an organized visual rehabilitation program.
Low vision has also been referred to as residual vision, limited vision, partial blindness, partial sight, visual handicap, reduced visual acuity, and visual limitation. It is estimated that more than 5 million people in the United States have a severe visual impairment to the degree that they are not able to read even with the help of ordinary spectacles.4 Chronic visual impairment is the most common cause of disability in the elderly after arthritis.5 Worldwide, there are estimated to be 135 million people affected by low vision and 90% of these people live in developing countries.6 Many such could benefit from a low vision evaluation and vision rehabilitation. Age-related macular degeneration is the leading cause of loss of vision in older white people in the United States and elsewhere.7,8,9 Age-related macular degeneration increases in all population-based studies and should be expected to continue to increase in the future. Maculopathy appears to be related to environmental factors such as the sun and ultraviolet radiation, to dietary factors, and to genetic factors.10,11,12 Many studies indicate a genetic correlation to macular degeneration and it is important that these studies continue as well as other studies to determine whether dietary supplements may help prevent macular degeneration.13 The clinician must stress to patients the importance of protecting the eyes from the sun and ultraviolet radiation, which is also involved in the creation of cataracts.14 The development of cataracts particularly increases as one approaches the equator where greater exposure to more sunlight exists. Any population exposed to the sun must be encouraged to protect the eyes with ultraviolet ray-blocking glasses or hats with visors or brims. Many members of this population in developing countries who develop cataracts also have poor diets. The combination of an antioxidant-deficient diet and sun appears to increase the development of cataracts. The incidence of glaucoma is higher in blacks so that this group needs access to ophthalmologic care to allow the proper diagnosis to be made and glaucoma to be treated.15,16 Diabetes mellitus is also an increasing problem as one ages and patients with diabetes now live longer and produce children who themselves have diabetes. It is well known that diabetes can be associated with the development of cataracts, glaucoma, and diabetic retinopathy so that it is important that all patients be examined for this problem and treated property for their diabetes. Blindness is 25 times more common in patients with diabetes than in those who do not have the disease.17,18
As people age, refractive change is one of the most frequent reasons for ophthalmologic examinations. Some evidence suggests that myopia is inherited; it has also been associated with increased intraocular pressure.19 It is, therefore, important, that all refractive errors be evaluated and that all patients who have increasing myopia should be examined not only for developing cataracts but also for glaucoma. Other ophthalmic diseases, which also cause significant visual loss, include uveitis, optic neuritis, and retinitis pigmentosa.
Ocular trauma is one of the leading causes of major visual problems.20 Trauma can occur at work, while playing sports, and during other activities. Eye injuries in sports can occur in soccer, ice hockey, lacrosse, rugby, cricket, football, skiing, handball, basketball, volleyball as well as tennis.21,22 Participants need to wear guards to protect their eyes as well as to be aware that ocular injuries can occur in sports. Boxing is frequently associated with ocular injuries, including traumatic cataracts and retinal detachment.
It is often difficult to define the term low vision except that it is generally applied to vision that is not adequate for what an patient would like to do with his or her eyes.23,24 This may mean the vision loss is enough to make it difficult for a patient to read the newsprint even with spectacles. Usually the term refers to patients with a best corrected acuity of 20/50 or worse in the better seeing eye or visual field of 30 degrees or less in the better eye.
People with low vision have usable sight whereas those who are blind have no light perception or no usable sight. Legal blindness is a term that should not be confused with blindness. Those who have limited vision may be designated as legally blind but this does not mean they are blind. The term legal blindness was developed by the U.S. federal government specifically for the purpose of determining eligibility for income tax benefits and federal or state assistance in the United States for those whose vision prevented them from seeing well enough to work.25 One qualifies as legally blind in the United States when one has the best corrected vision in the better eye equal to or less than 20/200 or a visual field in the better eye equal to or less than 20 degrees.
This nomenclature does not necessarily mean the legally blind person is functionally blind. Functional blindness describes fewer than 10% of people with vision loss.4 Those who are functionally blind have a severe vision loss and are unable to use vision enhancement techniques and optic devices, but instead they must use vision substitution techniques and devices such as a guide dog, Braille, or a white cane. The term partially sighted is used to describe those who have irreversible vision loss but can function with the help of enhancement techniques and devices.
There are three major divisions of visual impairment.1,26 The first is the totally blind person who cannot perceive light or light projection. The second group, which is functionally blind, is composed of those who may perceive light but have no useful vision even with vision enhancement techniques. The third group are the partially sighted, which group is subdivided into two groups; the legally blind who in the better eye have a best corrected visual acuity of 20/200 or less or a visual field of 20 degrees or less and people who are not legally blind who have a best corrected visual acuity of 20/50 or less but better than 20/200 and a visual field greater than 20 degrees in the better eye. Those who benefit from low vision evaluations are the partially sighted patients who are legally blind and those in the 20/50 to 20/200 range. It is estimated that of this total group of visually impaired patients only 9% are legally blind and have no useful vision. This means that a substantial population who could benefit from vision rehabilitation exists.
EVALUATION OF PEOPLE WITH LOW VISION
When evaluating patients with low vision the clinician must understand not only their visual problems but their psychological problems as well. In addition many of these patients, as they age, have other medical problems, which may include loss of hearing and arthritis. All these factors must be taken into account when dealing with their visual problems.
There are many psychosocial factors in vision rehabilitation given that loss of vision changes the course of one’s life and alters relationships with many patients including family, friends, and coworkers. The ability to adapt to vision loss depends not only on the diagnosis and attendant visual problems but also on the patient’s interaction with others. The age at which this vision loss occurs is crucial. If a loss of vision occurs when the patient is young and working it may mean a drastic change in the ability to carry on a career. If this loss occurs when the patient is older and retired, however, it affects relationships with spouses, children, and friends and often contributes to a loss of self-esteem. People with vision loss often experience a period of great sadness before adjustment occurs.
This grief process has been described as being divisible into six stages and is often compared with that of grieving a terminal illness.27 Past life must be left behind and the afflicted person must learn to grasp a new physical reality emotionally and intellectually. At first when patients learn what their problem is they are shocked and upset. This stage is then followed by denial, an unconscious response, which normally occurs to deal with the intense anxiety that ensues. Many patients at this stage may deny the seriousness of their conditions and also be noncompliant in caring for themselves. It is often difficult for the ophthalmologist to inform patients that their vision will not improve. In a study performed at the Massachusetts Eye and Ear Infirmary Vision Rehabilitation Center, 25% of all interviewed patients examined denied that they knew what was the matter with their eyes, claiming that no one told them,3 even though their cases had been discussed many times with them by their eye care specialists and low vision evaluators. Unless affected patients recognize their problem, it is impossible to achieve vision rehabilitation successfully. The ophthalmologist must not offer any hope for a cure for the problem but explain to the patient that she or he must learn now to use any residual vision. The next stage many encounter is that of guilt, that in some way they caused their vision loss. It is important to inform these patients about the problem, acknowledge their grief, and provide them with honest answers to their questions. The third stage is often one of bargaining in which patients may believe they may derive some benefit if the perform certain tasks, such as eating special foods and diets, taking vitamins, or contributing to charity as if this may somehow reverse the diagnosis. The fourth stage is anger, because such patients are often angry about why this problem should happen to them and why many others of their age do not have this problem. Many patients may be angry at their ophthalmologist for “creating” this problem. Many blame their ophthalmologist for shining a bright light in their eyes and then claiming that they could not see after that dilated retinal examination. At this stage, the clinician must explain to the patient as well as to family members that this vision loss is something that occurred and that they must learn to use their residual vision. The fifth stage is depression, which may be temporary or long term. This stage usually occurs when patients understand that their vision loss is permanent and major adjustments are necessary. Such afflicted patients should be counseled, supported, and encouraged to learn new skills and adaptive techniques. Many such patients may even become suicidal; it is important to be aware of this and make certain that this does not occur. The sixth and final stage is one of adaptation and hopefully this stage continues for a long time. During this phase, patients discuss their visual problems with increasing ease and develop realistic short and long-term plans. It is important to let them try to do whatever they would like to do with their eyes and work together with them and encourage use of the eyes.
Families should accompany patients during the examination so the family members can be part of the grieving and resolution of the various phases the patients are going through. Many family members also pass through these stages of grief experienced by those experiencing vision loss.
Vision rehabilitation can be performed in an office by an ophthalmologist, an optometrist, or with the aid of ophthalmic technicians.28 This is an area where ophthalmologists can work together with optometrists in a harmonious relationship. A more complex approach to a low vision evaluation, such as evaluating multiple vision aids, can be performed at a major center or at a large practice. This can be a facility for the visually impaired or at a medical center.29 Most patients would find it more convenient having their vision rehabilitation evaluation performed close to home but sometimes this is impossible.
If a practitioner intends to perform vision rehabilitation in the office, it is important to have some vision testing materials for distance and near. There could include a trial frame, lenses for refraction, an Amsler grid, and contrast sensitivity function tests and glare testing. It is often helpful to have a trial set of basic low vision optic aids along with some reading lamps and writing material. It is important when performing a vision rehabilitation evaluation to inquire what the patient would like to be able to accomplish visually. Most patients examined for vision rehabilitation wish to be able to read, including newspapers and magazines. Because many patients were not necessarily born in the United States, it is helpful to have reading materials in the patient’s native language. This may include various foreign language newspapers or magazines (Fig. 1). It is often helpful to ask patients to bring in their own magazines or newspapers and test the vision with their own reading material. It is also helpful to have a reading stand and other samples of typical reading material such as the comics, crossword puzzles, obituaries, and the stock market page as well as playing cards and sewing materials.
 Fig. 1. Patients who are visually disabled often need strong magnifying spectacles with short focal lengths; they must be encouraged to hold their reading material close to their eyes. These patients should be advised to bring personally selected reading material to the examination. |
THE EVALUATION
A visual rehabilitation examination should be considered only the first step in a process for those with irreversible vision loss. The objective of this evaluation is to enable patients with vision problems to maximize their residual vision through the use of adaptive devices and techniques.
The first stage in every evaluation is one of history taking. As the first stage in the taking of the history, it is important to ask patients why they have come for the evaluation. Many patients who have this type of evaluation often reply that they don’t know. It is then important to educate the patient and family members why the examination is taking place. Most patients who are having this type of evaluation wish to be able to read and this is where vision rehabilitation is most helpful. After the primary visual motive is determined, it is important to ask the patient about other visual tasks and whether they are presenting any problems. It is important to inquire whether the patient can get around in a familiar or unfamiliar area. The familiar area can be inside the home or in a shopping mall. Many patients wish to maintain their financial independence and it is important to inquire whether they can write a check or a letter. Most patients wish to be able to read and it is important to find out what they would like to be able to read. Many patients wish to read television listings and unfortunately the print in most such material is very small and difficult for many of our patients to use. Most US patients like to watch television and it is important to inquire whether they have any difficulties in this area. Moreover, the clinician should encourage patients to sit as close as they would like to the television screen because the magnification of nearness is of great help to these patients. At the same time, the clinician should ask whether the patient likes to go to the movies and if so, does this present any problems. Many would like to be able to but have difficulty in the theater; so again, it is helpful to encourage these patients to sit in the front of the theater rather than in the back. The patient must be assured that sitting close to the television screen or the movie screen will not damage or injure their eyes in any way. Most restaurant menus usually have black print on a white background, which is the easiest contrast print for our patients to read. Unfortunately, a small percentage of restaurants may have menus with colors that offer poor contrast, such as black print on a red background, and for most this is very difficult to read. Many restaurants have dim illumination that makes it even more difficult for those with impaired vision to read menus. Some patients listen to whatever someone else is ordering and inform the waiter or waitress that they “will have the same thing.” Family members and friends should be encouraged to help visually impaired patients with their menu selections and, of course, the waiter or waitress can also describe many of the foods presented. When in a restaurant, family members may be helpful in orienting food on the plate and, in fact, some patients may need help in cutting meat into bite-sized portions. Patients should be asked whether they have any problem pouring liquids either at home or in the restaurant. Many patients at home have hot tea or coffee in the morning and it is important to instruct them in how to do this safely to prevent burning themselves or missing the cup. Some patients have hobbies, many collect coins or stamps, and it is important to encourage them to continue with whatever hobby they enjoy with the help of optic or nonoptic approaches.
ASSESSMENT OF VISION
Both near and distance visual acuity of all patients who have vision problems must be measured and evaluated accurately. For many patients, it is not possible to test at the usual distance of 20 ft. Testing of visual acuity can also be accomplished at a shorter distance. It is important to record the visual data as measured for near and far. These numbers can be converted to 20-ft Snellen designation by multiplying both the numerator and denominator of the visual acuity by the number that converts that numerator to 20. For example, the patient who reads the 20/40 line at 10 ft viewing the Snellen type can be recorded as having 10/40 or 20/80 (10/40 × 2/2 = 20/80) vision. This conversion to the 20-ft designation can be helpful when reports regarding these patients are sent to outside agencies. Outside agencies may not understand 10/40 and what this means but they will understand 20/80. It is also important to not only measure each patient’s eye individually but with binocular vision. Quite often, binocularity improves the vision a sufficient amount that the patient can function well with conventional lenses rather than with special low vision devices.
Various charts are available that can be very helpful for vision testing. These include the BaileyLovie, the Bausch and Lomb, the Sloan letter chart, and the Early Treatment Diabetic Retinopathy Study (ETDRS) charts (Fig. 2). These charts are recommended because they are simple, accurate, and reproducible. Standard Snellen charts usually underestimate the acuity of patients who have vision between 20/80 and 20/200. The other advantage of testing patients closer to the charts than 20 ft is that the patient feels a sense of accomplishment knowing he or she is able to read several lines on a chart that may be 10 or 5 ft away. It is important to congratulate and encourage these patients during the examination as they read the lines.
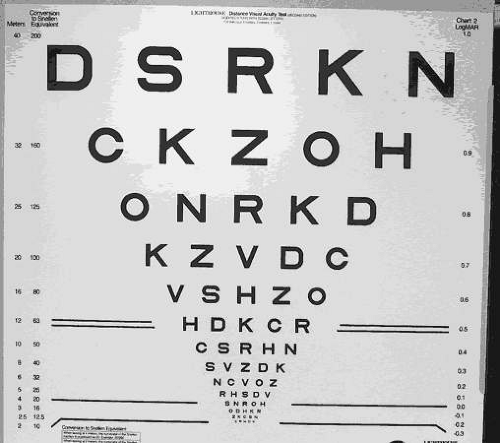 Fig. 2. Early Treatment Diabetic Retinopathy Study-modified distance acuity chart can be used to test distance vision at 2 to 3 m from the patient. |
Near visual acuity can be measured in several ways. There are some special reading charts with single letters modeled on the ETDRS distance chart, such as the Lighthouse Near Test card and quite often it is helpful to measure patients with whatever reading material they would like to be able to read (Fig. 3). This can be the patient’s own magazines or newspapers and this makes much more sense to patients who wish to be able to read these very materials. The reading visual acuity score then can be recorded by measuring the size of the type on the page. Of course, these measurements should be conducted with the patient’s own reading glasses or bifocals or with a correction recommended by the examiner.
 Fig. 3. Many patients do not read English and it is helpful to have newspapers or magazines printed in the language they usually read. |
Many low vision acuity charts differ from regular charts in several ways. Each line of optotype is an equal factor smaller than the previous line and each line contains optotypes with similar resolution difficulty. There is also a proportional decrease in spacing that is equal to letter width in each particular line. Of course, the ability to resolve optotypes visually does not directly correlate with the ability to read text, and that is why it is important for patients to be tested on their preferred reading material.
Some patients are not able to read letters because of unfamiliar language, illiteracy, or other types of cognitive impairment. For these patients, it is important to use number charts, symbol cards, or testing cards for the illiterate, which are available (Fig. 4). Even though some patients may be illiterate in reading letters, most can read numbers so that this is an important way of testing vision for near and far.
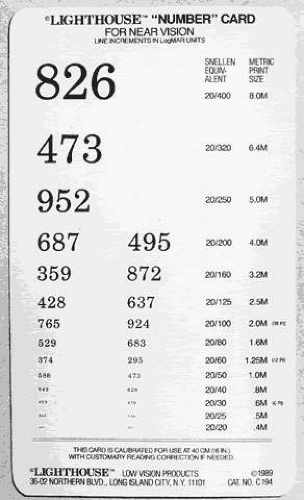 Fig. 4. The Lighthouse number card for near vision is helpful for the young, old, literate, illiterate, and for patients whose native language is not English. |
Another test that may be important to a visually impaired patient is the visual field.30,31 The clinician must know the location, density, size and the shape of central and peripheral visual field deficits to place reading material in an area where there is no visual field loss. Many patients with dense central scotomas, particularly those with macular degeneration, have difficulty with straight ahead vision and it is important to position the reading material to the right or left of fixation. Often the combination of performing a visual field test and vision rehabilitation examination on the same day may be too fatiguing for many elderly patients. Confrontation fields should be attempted because they are often very helpful. By knowing the area of the visual field loss, the low vision evaluator can best explain to the patient and family where to position materials to achieve the best possible vision. This also holds for distant vision but most patients quickly discover the head and eye position that provides maximum vision. This is very helpful for the patients who would like to walk around the neighborhood, watch television, and use their eyes for near, intermediate, and distance visual tasks.
Besides confrontation testing, several others means exist to measure visual field tests from the tangent screen to the Goldmann perimeter to the automatic visual field machines. The scanning laser ophthalmoscope (SLO) can also be used to plot the scotomas present and also find the preferred retinal locus for the best vision.32 In any case, whichever modality is chosen, best approach should include a relatively shorter time visual field test that is much easier for elderly patients to use.
Another possible visual measurement that may be important is that of color vision. Measuring color visual defects can be useful to many patients with loss of vision. For patients with severe vision loss, the Farnsworth D-15 color vision test can be used. This relatively inexpensive test can quickly be administered and can detect red, green, yellow, and blue perceptual defects.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


