Vestibular and Balance Laboratory Studies
Neil T. Shepard
Kristen L. Janky
Jaynee A. Handelsman
This chapter is one of the clinical companions to the preceding chapter on the vestibular function and anatomy. A clear understanding of those concepts and principles is vital to the appreciation of the information presented herein. The anatomy and physiology of the vestibular and balance systems form the basis against which interpretations of patients’ presenting history, signs, symptoms and laboratory test results are developed. The nomenclature used in this chapter will follow that suggested for the International Classification of Vestibular Disorders (1). Therefore, the following are the definitions of the terms used to describe symptoms for patients reporting with vertigo, dizziness, or unsteadiness:
Vertigo—sensation of self (internal) or environmental (external) movement when such movement is not occurring, for example, spinning, rocking, swaying, tilting, bobbing, sliding, or bouncing.
Dizziness—sensation of disturbed or impaired spatial orientation without a sensation of self or environment movement.
Unsteadiness—sensation of being unstable—independent of position without a directional preference.
In considering the evaluation of the patient with complaints of vertigo, unsteadiness, and dizziness or combinations of these descriptors, one must look beyond just the peripheral and central vestibular system with its oculomotor connections. The various pathways involved in postural control, only part of which have direct or indirect vestibular inputs, should be kept in mind during an evaluation. Additionally, significant variations in symptoms and test findings can be generated by migraine disorders (2) and/or anxiety disorders (3), yet these are diagnosed primarily by case history and require a specific line of questioning, not by the use of laboratory testing per se; however, the test helps to set up a profile.
Evaluation of the dizzy patient should be guided by the information required to make initial and subsequent management decisions. In the acute patient, the primary aim is to rule out significant cardiovascular and neurological disorders, quiet symptoms, and determine a working diagnosis. Extensive laboratory testing is generally unnecessary in the acute patient since the presenting symptoms and office examination will primarily guide initial management decisions (see chapter 165 by Joel Goebel on the clinical evaluation of the patient with vertigo in this text). In the chronic patient (defined as having symptoms that are intermittent or persistent for greater than 2 months), addressing the question of why natural central compensation has not taken place in a significant manner to reduce symptoms and establish a refined diagnosis and treatment program would be the goal. While aspects of the laboratory testing, especially caloric testing, can be of use in the acute patient, it is the exception that these would be used acutely. Therefore, for the purposes of this chapter, discussion is limited to the evaluation of the chronic patient.
For the chronic patient, a detailed neurotologic history together with a comprehensive direct vestibular office examination is as important as in the acute patient. In the chronic patient, a detailed pre-evaluation patient questionnaire combined with a focused history obtained at the start of laboratory testing can facilitate selection of appropriate laboratory tests and guide the examiner regarding what tests beyond a basic core series of evaluations are needed for any given patient. This use of a staged testing protocol effectively allows laboratory information to be collected prior to the clinician’s direct office interview and examination so that all of the information can then be collectively analyzed in the context of the history and presenting symptoms (4).
Defining the role of the laboratory testing becomes an important aspect of the understanding of the benefit of the studies that are currently available.
Determination of extent and site of lesion within the peripheral and central vestibular system
Determination of the functional limitations in static and dynamic postural control (these may be related directly to gait abnormalities) and functional performance of the vestibuloocular reflex (VOR)
Assessment of the status of the compensation process
Along with symptom presentation, to aid in the prognosis and design of vestibular and balance rehabilitation
The collective use of the information is most often in the confirmation of the suspected site of lesion and diagnosis, both derived from the patient’s history and direct office vestibular evaluation with audiometric evaluation. This does not imply a prioritized order to the testing versus the office visit, as with chronic dizzy patients it can be very useful to triage them to laboratory evaluations prior to the office visit.
A common misconception is that the studies will render a specific diagnosis or at a minimum drive the remainder of the investigation and help determine levels of disability. However, when the various tests listed below are reviewed and correlated with high-level activities of daily living, virtually no significant relationships exist for the chronic dizzy patient (5, 6). Conversely, patient complaints cannot be used to predict the outcomes of these tests. In a limited manner, more functionally oriented evaluation tools such as computerized dynamic posturography (7) and dynamic visual acuity (DVA) testing (8) provide for correlation between test results, patient symptoms, and functional limitations (9, 10). It is hypothesized that the reason for this dichotomy in test results versus functional disability and symptom complaints is the inability of the tests to adequately characterize the status of the central vestibular compensation process (9, 11, 12). Thus, vestibular laboratory testing is never a replacement for a detailed neurotologic history and physical examination, but needs to be interpreted in context of the history and physical examination.
LABORATORY STUDIES
The discussion to follow provides a brief description of the various laboratory studies that are available for the investigation of the patient with vertigo, dizziness, or unsteadiness. In each case, the purpose for the study, general information about administration of the test, and its general interpretations are provided. A detailed presentation of each of the studies is beyond the scope of this chapter and text. Interested readers are referred to other sources for further information (13, 14, 15). For organizational ease, the tests are divided into those in more routine use and those found only in dedicated tertiary balance centers.
Common Procedures
Electronystagmography/Videonystagmography
Electronystagmography (ENG) and videonystagmography (VNG) utilize complete computer-based systems for performing eye movement testing. During ENG testing, horizontal and vertical eye movements are recorded indirectly using electrodes via the corneoretinal potential (dipole). Electrodes are typically placed at each lateral canthus and above and below at least one eye with a common electrode on the forehead. During VNG testing, on the other hand, eye movements are recorded directly using infrared video cameras and digital video image technology. Specifically, for binocular recording, a reflected image of the eye is captured by cameras mounted above, in front of each eye or adjacent to the lateral canthi (Fig. 144.1) (16). For monocular recordings, a camera may be positioned directly in front of one eye (Fig. 144.1). Monocular recording has the disadvantage of failure to recognize and capture disconjugate eye movements. For both ENG and VNG, recording is typically limited to horizontal and vertical eye movements (three-dimensional systems are available adding the torsional movements but far from common use) and the data are recorded, digitally stored, and analyzed by the software in much the same way.
The ENG/VNG battery typically consists of a series of subtests designed to assess the function of the vestibular end organs, the central vestibuloocular pathways, and oculomotor processes, independent of vestibular input. ENG/VNG testing is useful for all patients of all ages with ongoing balance system disorders.
Oculomotor Evaluations
The availability of computerized ENG/VNG systems resulted in a transformation in the formal assessment of oculomotor function because of the ability to directly compare the timing and accuracy aspects of the eye movements with the target stimuli. The clinical utility of these tests is improved by exploiting their redundancy, such as when the results from multiple subtests point to the same site of lesion. Because oculomotor function changes with age, it is important to compare results with norms in order to minimize the number of false-positive results.
Gaze Stability Testing. The patient is typically asked to fixate on a stationary target that is positioned at eye level at a distance of 1 to 1.5 m, and the eyes are observed for the presence of nystagmus or other abnormal movements. Both horizontal and vertical eye movements are recorded. Eccentric gaze is also evaluated by moving the target from center to horizontally and vertically eccentric positions. Individuals without any peripheral or central involvement may demonstrate transient nystagmus when the eyes are at the extreme eccentric positions (referred to as end-point nystagmus, usually dies away within 5 seconds); persistent nystagmus that occurs when the targets are positioned appropriately is always considered to be abnormal.
Gaze-evoked nystagmus can originate from either the peripheral or the central vestibular system with differences in clinical presentation between the two. Nystagmus that is peripheral in origin will generally be direction fixed and
enhance with fixation removed. Nystagmus is considered to be of central origin if it changes direction with change in gaze direction, if it evidences rebound, where the fast component of the nystagmus changes with the direction of the last eye movement, it enhances or does not change in intensity with fixation. In rare instances, eye movements can be consistent with both peripheral and central origin (e.g., Bruin nystagmus seen in Cerebellar-Pontine Angle mass lesions). A variety of other abnormalities may be evidenced during gaze testing such as congenital nystagmus and a variety of saccadic intrusions (special grouping of involuntary saccadic eye movements when visual fixation target is present), suggesting central vestibular system involvement (17).
enhance with fixation removed. Nystagmus is considered to be of central origin if it changes direction with change in gaze direction, if it evidences rebound, where the fast component of the nystagmus changes with the direction of the last eye movement, it enhances or does not change in intensity with fixation. In rare instances, eye movements can be consistent with both peripheral and central origin (e.g., Bruin nystagmus seen in Cerebellar-Pontine Angle mass lesions). A variety of other abnormalities may be evidenced during gaze testing such as congenital nystagmus and a variety of saccadic intrusions (special grouping of involuntary saccadic eye movements when visual fixation target is present), suggesting central vestibular system involvement (17).
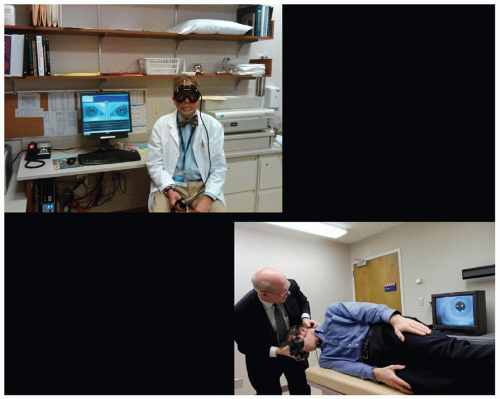 Figure 144.1 Shown are photographs that illustrate two eye movement recording techniques using VOG. The top picture shows a system with cameras mounted above reflecting see-through lenses and the display of the binocular recordings on the computer. The lower figure shows the use of monocular camera system affixed on the goggles directly in front of the right eye and the image seen on the monitor behind the subject. |
Saccade Evaluation. As is the case in gaze testing, the patient is asked in saccade testing to follow a computercontrolled visual target. Random saccade testing is the paradigm that is most often included in the ENG/VNG battery. The patient’s eye movements are compared by the computer to the target stimuli and the analysis typically yields measurements of saccade accuracy, latency, and velocity. Saccade accuracy generally refers to the amplitude of the eye movement relative to the target, latency refers to the delay between the onset of target movement and the initiation of eye movement, and velocity refers to the maximum sampled velocity of the saccade once it has been initiated.
The interpretation of saccade data must take into account patient variables such as age (although age-related normative data is not required), cognitive status, attention to task, visual acuity, sedation, sleep deprivation, comprehension level, and medications. Symmetrically inaccurate or slow saccades are often attributable to one or more of those variables. On the other hand, characteristic saccade abnormalities can suggest relatively specific sites of lesion and can provide for differentiating between brainstem and posterior cerebellar vermis involvement. For example, internuclear ophthalmoplegia (INO) results from a lesion in the medial longitudinal fasciculus (MLF) that causes a reduction of the neural signal to the ipsilateral medial rectus muscle (adduction) and preserved lateralrectus-mediated movements (abduction). The resulting
saccades in INO demonstrate slow velocity of adducting eye movements and overshoot for abducting eye movements. Details of the suggested lesion sites based on various combinations of abnormalities of latency, velocity, and accuracy are beyond the scope of this chapter but are available elsewhere (17).
saccades in INO demonstrate slow velocity of adducting eye movements and overshoot for abducting eye movements. Details of the suggested lesion sites based on various combinations of abnormalities of latency, velocity, and accuracy are beyond the scope of this chapter but are available elsewhere (17).
Smooth Pursuit Tracking. Testing of smooth pursuit ability is conducted by having a patient follow a computer-controlled visual target, typically moving in a sinusoidal pattern that varies in frequency over time. Patient eye movements are evaluated qualitatively by looking for smooth eye movements. As is true with saccade testing, patient variables can negatively impact performance and interfere with interpretation. Use of age-appropriate norms is essential, as pursuit performance tends to degrade with age. The main outcome parameter is gain, which is calculated by dividing eye velocity by target velocity. Of all the oculomotor subtests, pursuit tracking has been demonstrated to be the most sensitive to central vestibular system abnormalities; however, it does not provide the same site-of-lesion localization as the remaining oculomotor subtests (17). Abnormalities with pursuit are typically taken as an indication of possible vestibulocerebellar region involvement but lesions in a variety of other areas can produce abnormalities of pursuit especially when pursuit is disrupted for both eyes moving to the right or left. Asymmetrically impaired pursuit is a more specific finding and suggests a unilateral cerebellar hemispheric or asymmetrical posterior fossa lesion (13).
Optokinetic Nystagmus. In order to truly assess the optokinetic system, use of a full-field visual stimulus and a phenomenon called “optokinetic afternystagmus” is required (13). The production of true optokinetic nystagmus involves a combination of the neurological substrate involved with smooth pursuit tracking together with areas that respond to moving visual stimuli in a full-field format but do not respond to head movement, the so-called optokinetic areas. Further, when viewing a full-field (90% or more of the visual field filled with the repeated moving targets) stimulus, the initiation of the nystagmus is dominantly a result of smooth pursuit tracking with the OKN component added as the stimulus is continued requiring seconds to fully develop. The response then continues as a combination of both smooth pursuit tracking and optokinetics. Therefore, to evaluate OKN function in isolation from smooth pursuit, one must take advantage of a perseveration of nystagmus caused by stimulation of the optokinetic system when the person is suddenly put into the dark after a minimum of 30 seconds worth of stimulation (called optokinetic after nystagmus [OKAN]). As soon as the target has been extinguished for 1 second, the smooth pursuit system no longer has any influence and the OKAN is a direct result of the activity of the optokinetic system reflected through the area of the brainstem referred to as the velocity storage system. In order to produce the OKN stimulation through retinal input and signals transmitted via the accessory optic track, the stimulus needs to fill a minimum of 90% of the visual field and be capable of producing a circularvection effect (the illusion of circular motion when not moving).
Therefore, optokinetic nystagmus testing as a part of an ENG/VNG battery using a laser target or a traditional light bar is not a true optokinetic test but is a test dominated by smooth pursuit. Abnormal optokinetic nystagmus has a localizing value that is similar to smooth pursuit, although the sensitivity is poorer. For that reason, the cost-benefit ratio of inclusion of this test in the battery is poor.
Spontaneous Nystagmus
This test is performed with the patient sitting upright with the head straight. Eye movements are recorded while the patient is gazing straight ahead (not imagining a target) with visual fixation removed. Jerk nystagmus is the principal abnormality and is typically classified by the direction of the fast component of the nystagmus but measured by the velocity of the slow component. Clinically significant, direction-fixed nystagmus is interpreted to indicate pathology within the peripheral vestibular system if the oculomotor evaluation is normal and the nystagmus is significantly suppressed with visual fixation.
Hyperventilation Testing
The purpose of the hyperventilation test is to help diagnose, or unmask, disorders of the peripheral vestibular system and/or VIII cranial nerve (18, 19, 20, 21, 22). Secondly, the test can suggest possible anxiety disorder via premature symptoms without nystagmus (23). The hyperventilation test is completed by first removing fixation, either by Frenzel lenses or infrared goggles, and then having the patient take one breath per second for 30 to 90 seconds. Nystagmus induced by hyperventilation is considered significant if it persists greater than 5 seconds and if the peak slow-phase velocity is greater than 3 to 4 degrees per second, subtracting out any preexisting spontaneous nystagmus. If no nystagmus is provoked but the patient becomes symptomatic within the first 20 to 30 seconds, then anxiety issues are suspected.
Hyperventilation-induced nystagmus can beat ipsilesionally (with the fast-phase beating toward the side involved) or contralesionally (with the fast-phase beating away from the side involved). As a general rule of thumb, hyperventilation-induced nystagmus more often beats contralesionally in peripheral vestibular system lesions and ipsilesionally in VIII nerve or retrocochlear lesions: however, this relationship is not mutually exclusive.
Headshake
The headshake test also helps uncover asymmetries in peripheral and central vestibular system function and serves as an indication of dynamic central compensation. The headshake test is completed by removing fixation. The patient’s head is shaken back and forth in the
horizontal plane at approximately 2 to 4 Hz for 10 to 15 seconds. Post headshake nystagmus is considered clinically significant if at least three to five consecutive beats of nystagmus are present directly following the headshake and if the nystagmus peak slow-phase velocity is greater than 3 to 4 degrees per second after subtracting out any preexisting spontaneous nystagmus (20, 24, 25, 26). Both vertical and horizontal headshaking can also be completed. The headshake test has relatively low sensitivity (30% to 35%) but high specificity (90% to 95%) in peripheral vestibular disorders, with the incidence of postheadshake nystagmus increasing as the severity of caloric paresis increases. Postheadshake nystagmus has also been documented in as many as 50% of normal controls (27



horizontal plane at approximately 2 to 4 Hz for 10 to 15 seconds. Post headshake nystagmus is considered clinically significant if at least three to five consecutive beats of nystagmus are present directly following the headshake and if the nystagmus peak slow-phase velocity is greater than 3 to 4 degrees per second after subtracting out any preexisting spontaneous nystagmus (20, 24, 25, 26). Both vertical and horizontal headshaking can also be completed. The headshake test has relatively low sensitivity (30% to 35%) but high specificity (90% to 95%) in peripheral vestibular disorders, with the incidence of postheadshake nystagmus increasing as the severity of caloric paresis increases. Postheadshake nystagmus has also been documented in as many as 50% of normal controls (27
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
