 Vascular Tumors of the Eyelids
Vascular Tumors of the EyelidsEyelid Congenital Capillary Hemangioma (Strawberry Hemangioma)
General Considerations
Congenital cutaneous capillary hemangioma (infantile hemangioma, benign hemangioendothelioma, strawberry nevus) is a benign vascular tumor that is either apparent at birth or develops a few weeks after birth. It is one of the most common tumors of infancy (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36). It can be located superficially, deep, or both. There is a tendency for this lesion to occur in siblings and affected triplets have been described (7). Rarely, cutaneous capillary hemangioma can be associated with extensive hemangiomatosis that can involve the viscera and other organs. These large tumors trap platelets within their vascular channels, leading to thrombocytopenia and secondary coagulopathy. This condition, called the Kasabach-Merritt syndrome, is sometimes fatal (3).
Clinical Features
The superficial eyelid and periocular capillary hemangioma (strawberry hemangioma) appears initially as a red vascular macule that progressively enlarges and becomes more elevated for 3 to 6 months after diagnosis. It usually becomes stable by age 12 to 18 months and then slowly involutes. It has been estimated that about 30% of cutaneous capillary hemangiomas regress completely by age 3 years and 75% to 90% by age 7 years (4). Almost complete regression usually occurs by age 5 years. Although it may have a very bothersome cosmetic appearance early in its course, the eventual regression is often dramatic, leaving little cosmetic defect.
In contrast to the superficial form, the deep capillary hemangioma lies in the subcutaneous tissues with little or no involvement of the epidermis. It is blue-gray in color, soft to palpation, and becomes more prominent with crying or straining. A tumor that extends deeper in the orbit can produce proptosis and displacement of the globe, and is important in the differential diagnosis of infantile orbital tumors. A typical overlying hemangioma in the skin should suggest that the deeper orbital tumor is also a capillary hemangioma. Its natural course is similar to the superficial variant, with fairly rapid growth followed by regression. This deep capillary hemangioma is covered in the atlas of orbital tumors.
Complications
The main complications of periocular capillary hemangioma are strabismus and amblyopia. The strabismus is either secondary to tumor impingement on the rectus muscles or secondary to amblyopia. The amblyopia can be a result of the tumor obstructing the pupil or a result of the anisometropia induced by the compression of the globe by the tumor. The refractive error often persists even after the hemangioma has regressed (5).
Differential Diagnosis
When the eyelid skin is involved by the typical red lesion, the diagnosis is generally quite evident. The differential diagnosis of deeper capillary hemangioma includes several other childhood anterior orbital neoplasms, including lymphangioma, rhabdomyosarcoma, and myeloid sarcoma (leukemia). These are discussed further in the Atlas of orbital Tumors.
Pathology
Histopathologically, capillary hemangioma consists of lobules of capillaries that are separated by fibrous tissue septa. The proliferating endothelial cells may obliterate the capillaries (6). As a capillary hemangioma undergoes regression, it becomes less cellular and less vascular, and is replaced by fibrous tissue.
Pathogenesis
The pathogenesis of cutaneous capillary hemangioma, previously unknown, has been the subject of recent interest. It has been recognized that placenta and cutaneous capillary hemangiomas share unique immunohistochemical similarities. This has led to speculation that infantile hemangiomas could be of placental origin. Two theories have been proposed to explain this hemangioma-placental connection. First, angioblasts may proliferate toward placental tissue in the site where the hemangioma develops. A second intriguing theory is that cells of placental origin could embolize to the target areas and proliferate into the tumor (“metastatic placenta”) (8,9).
Management
Because most infantile capillary hemangiomas regress spontaneously, it is generally appropriate to follow the tumor with observation rather than surgical resection. However, it is important to check visual acuity and do a refraction. Any amblyopia or potential amblyopia should be treated with patching the opposite eye. Most authorities also use local or systemic corticosteroids to hasten resolution.
There has been considerable enthusiasm for the use of systemic corticosteroids or intralesional injection of cortico-steroids to hasten regression of capillary hemangioma of the ocular region that have amblyopic potential (10,11,12,13,14,15,16,17,18,19,20,21,22,23,24). Most patients treated in that manner have had a good response without complications. However, occasional complications of intralesional corticosteroids include central retinal artery obstruction (16,17), linear perilymphatic subcutaneous fat atrophy (18,19), eyelid depigmentation (20), eyelid necrosis (21), and adrenal gland suppression (22,23,24). As an alternative, topical corticosteroids have been occasionally used (25,26). Intralesional interferon a-2a and -2b have also been used for capillary hemangioma that is unresponsive to corticosteroids (27,28,29). Laser therapy has been advocated for some cutaneous hemangiomas (30,31,32).
Finally, although surgical removal has historically been discouraged, there is a valid argument to manage selected periorbital capillary hemangiomas by surgical resection (33,34,35,36). An indication for surgical resection may be a circumscribed subcutaneous hemangioma that is enlarging in a very young infant. Such a tumor is destined to become very large
before it regresses and early complete surgical removal can avoid more difficult management of a larger tumor and worse amblyopia. An eyelid crease incision, with removal of the mass intact if possible, and closure of the skin with fine absorbable sutures can achieve a very satisfactory outcome (35). However, surgical resection should generally be avoided for larger superficial lesions that have extensive involvement of the epidermis. Such tumors may show satisfactory spontaneous regression.
before it regresses and early complete surgical removal can avoid more difficult management of a larger tumor and worse amblyopia. An eyelid crease incision, with removal of the mass intact if possible, and closure of the skin with fine absorbable sutures can achieve a very satisfactory outcome (35). However, surgical resection should generally be avoided for larger superficial lesions that have extensive involvement of the epidermis. Such tumors may show satisfactory spontaneous regression.
Selected References
1. Haik BG, Carroll GS, Kilmer SL. Periocular hemangiomas. In: Mannis MJ, Macsai MS, Huntley AC, eds. Eye and Skin Disease. Philadelphia: Lippincott Raven; 1996:439-447.
2. Haik BG, Jakobiec FA, Ellsworth RM, et al. Capillary hemangioma of the lids and orbit: an analysis of the clinical features and therapeutic results in 101 cases. Ophthalmology 1979;86:760-789.
3. Haik BG, Karcioglu ZA, Gordon RA, et al. Capillary hemangioma (infantile periocular hemangioma). Surv Ophthalmol 1994;38:399-426.
4. Margileth AM, Museles M. Current concepts in diagnosis and management of congenital cutaneous hemangiomas. Pediatrics 1965;36:410-416.
5. Robb RM. Refractive errors associated with hemangiomas of the eyelids and orbit in infancy. Am J Ophthalmol 1977;83:52-58.
6. Font RL. Eyelids and lacrimal drainage system. In: Spencer WH, ed. Ophthalmic Pathology. An Atlas and Textbook. 4th ed. Philadelphia: WB Saunders; 1996:2322-2325.
7. Shields CL, Shields JA, Minzter R, et al. Cutaneous capillary hemangiomas of the eyelid, scalp, and digits in premature triplets. Am J Ophthalmol 2000;129:528-531.
8. North PE, Waner M, Mizeracki A, et al. A unique microvascular phenotype shared by juvenile hemangiomas and human placenta. Arch Dermatol 2001;137:559-570.
9. North PE, Waner M, Brodsky MC. Are infantile hemangiomas of placental origin?Ophthalmology 2002;109:633-634.
10. Hiles DA, Pilchard WA. Corticosteroid control of neonatal hemangiomas of the orbit and ocular adnexa. Am J Ophthalmol 1971;71:1003-1008.
11. Brown BZ, Huffaker G. Local injection of steroids for juvenile hemangiomas which disturb the visual axis. Ophthalmic Surg 1982;13:630-633.
12. Zak TA, Morin JD. Early local steroid therapy of infantile eyelid hemangiomas. J Pediatr Ophthalmol Strabismus 1981;18:25-27.
13. Kushner BJ. Intralesional corticosteroid injection for infantile adnexal hemangioma. Am J Ophthalmol 1982;93:496-506.
14. Motwani MV, Simon JW, Pickering JD, et al. Steroid injection versus conservative treatment of anisometropia amblyopia in juvenile adnexal hemangioma. J Pediatr Ophthalmol Strabismus 1995;32:26-28.
15. O’Keefe M, Lanigan B, Byrne SA. Capillary haemangioma of the eyelids and orbit: a clinical review of the safety and efficacy of intralesional steroid. Acta Ophthalmol Scand 2003;81:294-298.
16. Ruttum MS, Abrams GW, Harris GJ, et al. Bilateral retinal embolization associated with intralesional corticosteroid injection for capillary hemangioma of infancy. J Pediatr Ophthalmol Strabismus 1993;30:4-7.
17. Egbert JE, Schwartz GS, Walsh AW. Diagnosis and treatment of an ophthalmic artery occlusion during an intralesional injection of corticosteroid into an eyelid capillary hemangioma. Am J Ophthalmol 1996;121:638-642.
18. Droste PJ, Ellis FD, Sondhi N, et al. Linear subcutaneous fat atrophy after corticosteroid injection of periocular hemangiomas. Am J Ophthalmol 1988;105:65-69.
19. Ford MD, Codere F. Perilymphatic subcutaneous atrophy in adnexal hemangioma: a complication of intralesional corticosteroid injection. Ophthalmic Surg 1990;21:215-217.
20. Cogen MS, Elsas FJ. Eyelid depigmentation following corticosteroid injection for infantile ocular adnexal hemangioma. J Pediatr Ophthalmol Strabismus 1989;26:35-38.
21. Sutula FC, Glover AT. Eyelid necrosis following intralesional corticosteroid injection for capillary hemangioma. Ophthalmic Surg 1987;18:103-105.
22. Weiss AH. Adrenal suppression after corticosteroid injection of periocular hemangiomas. Am J Ophthalmol 1989;107:518-522.
23. Glatt HJ, Putterman AM, Van Aalst JJ, et al. Adrenal suppression and growth retardation after injection of periocular capillary hemangioma with corticosteroids. Ophthalmic Surg 1991;22:95-97.
24. Goyal R, Watts P, Lane CM, et al. Adrenal suppression and failure to thrive after steroid injections for periocular hemangioma. Ophthalmology 2004; 111:389-395.
25. Elsas JF, Lewis AR. Topical treatment of periocular capillary hemangioma. J Pediatr Ophthalmol Strabismus 1994;31:153-156.
26. Cruz OA, Zarnegar SR, Myers SE. Treatment of periocular capillary hemangioma with topical clobetasol propionate. Ophthalmology 1995;102: 2012-2015.
27. Rosenthal G, Snir M, Biedner B. Corticosteroid resistant orbital hemangioma with proptosis treated with interferon alfa-2-a and partial tarsorrhaphy. J Pediatr Ophthalmol Strabismus 1995;32:50-51.
28. Hastings MM, Milot J, Barsoum-Homsy M, et al. Recombinant interferon alfa-2b in the treatment of vision-threatening capillary hemangiomas in childhood. J AAPOS. 1997;1:226-230.
29. Fledelius HC, Illum N, Jensen H, et al. Interferon-alfa treatment of facial infantile haemangiomas: with emphasis on the sight-threatening varieties. A clinical series. Acta Ophthalmol Scand 2001;79:370-372.
30. Gladstone GJ, Beckman H. Argon laser treatment of an eyelid margin capillary hemangioma. Ophthalmic Surg 1983;14:944-946.
31. Chopdar A. Carbon-dioxide laser treatment of eyelid lesions. Trans Ophthalmol Soc UK 1985;104:176-180.
32. Shorr N, Goldberg RA, David LM. Laser treatment of juvenile hemangioma. Ophthalmic Plast Reconstr Surg 1988;4:131-141.
33. Deans RM, Harris GJ, Kivlin JD. Surgical dissection of capillary hemangiomas. An alternative to intralesional corticosteroids. Arch Ophthalmol 1992;110:1743-1747.
34. Plager DA, Snyder SK. Resolution of astigmatism after surgical resection of capillary hemangiomas in infants. Ophthalmology 1997;104:1102-1106.
35. Aldave AJ, Shields CL, Shields JA. Surgical excision of selected amblyogenic periorbital capillary hemangiomas. Ophthalmic Surg Lasers 1999;30: 754-757.
36. Slaughter K, Sullivan T, Boulton J, et al. Early surgical intervention as definitive treatment for ocular adnexal capillary haemangioma. Clin Exp Ophthalmol 2003;31:418-423.
Eyelid Congenital Capillary Hemangioma: Superficial Type
The superficial type of capillary hemangioma (strawberry hemangioma) has typical clinical features and can show dramatic spontaneous regression.
 Figure 8.1. Superficial capillary hemangioma on right lower eyelid. |
 Figure 8.2. Superficial capillary hemangioma on right upper eyelid. |
 Figure 8.3. Superficial capillary hemangioma on medial aspect of upper eyelid. |
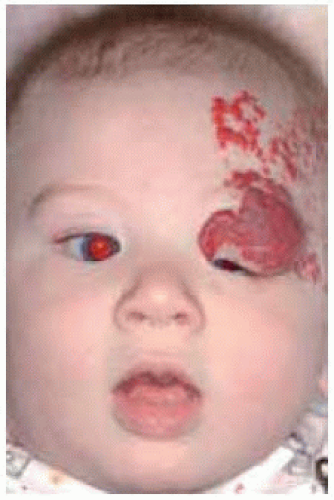 Figure 8.4. Extensive multifocal capillary hemangioma involving upper eyelid, forehead, and temporal scalp. |
 Figure 8.5. Side view of patient shown in Figure 8.4 demonstrating multifocal capillary hemangioma of face, scalp, and neck. |
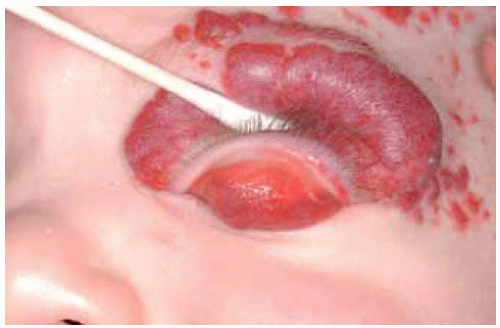 Figure 8.6. Eyelid capillary hemangioma with conjunctival involvement. The upper eyelid is being everted showing diffuse involvement of involved tarsal conjunctiva. It is necessary to evert the eyelid in such cases to determine the full extent of the lesion. |
Eyelid Congenital Capillary Hemangioma: Deep Type
The deep type of capillary hemangioma does not affect the epidermis and appears as a soft blue or pink subcutaneous mass.
 Figure 8.7. Deep capillary hemangioma of upper eyelid with overlying prominent blood vessels. |
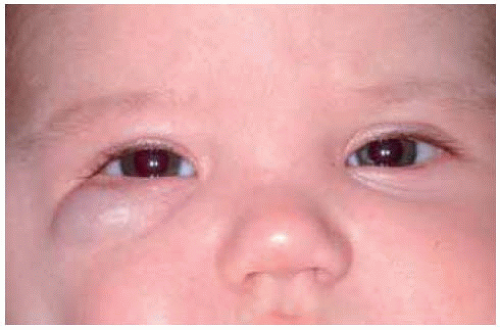 Figure 8.8. Deep capillary hemangioma beneath right lower eyelid imparting blue color to skin. |
 Figure 8.9. Deep capillary hemangioma in left lower eyelid. |
 Figure 8.10. Deep capillary hemangioma on side of nose near left medial canthus. |
 Figure 8.11. Deep capillary hemangioma beneath medial aspect of left upper eyelid. |
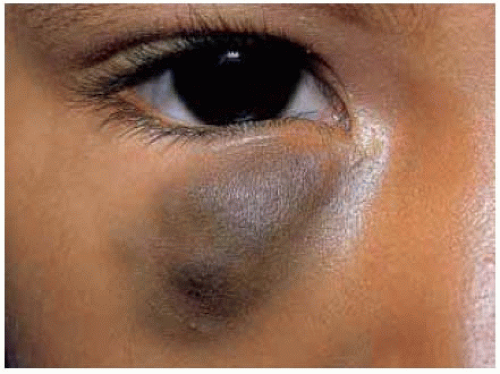 Figure 8.12. Blue-colored deep capillary hemangioma of lower eyelid. This can look similar to hemorrhage into a lymphangioma, but the lesion had slowly progressed and had no acute bleeding episodes. |
Eyelid Congenital Capillary Hemangioma: Regression of Superficial Type
 Figure 8.13. Combined superficial and deep capillary hemangioma in 3-month-old child. The child was treated with oral corticosteroids. |
 Figure 8.14. Same child 10 months later showing regression of tumor, less blepharoptosis, and more exposure of pupil. |
 Figure 8.15. Premature triplets, each of whom had multiple cutaneous capillary hemangiomas. The triplet on left shows forehead involvement, the middle one showed involvement of left upper eyelid, and the right one has finger hemangiomas that are not seen. |
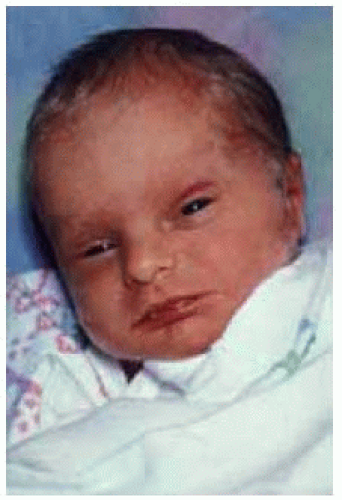 Figure 8.16. One of triplets at birth had a subtle capillary hemangioma of left upper eyelid. |
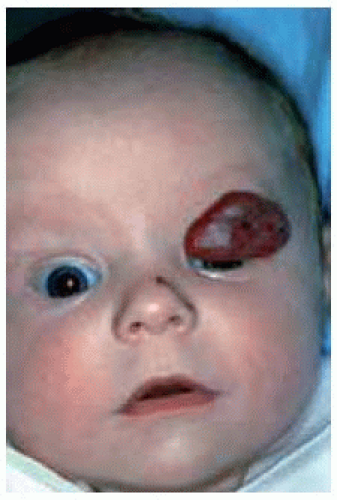 Figure 8.17. Same child shown in Figure 8.16, two months later showing larger capillary hemangioma that rapidly developed on left upper eyelid. The child was treated with oral corticosteroids. |
 Figure 8.18. Same child at age 3 years, showing complete resolution of the lesion. The resolution was rapid after the oral corticosteroids were initiated. |
Eyelid Congenital Capillary Hemangioma: Regression of Deep Type
 Figure 8.19. Deep capillary hemangioma in lower eyelid of infant. Observation was advised. |
 Figure 8.20. Same lesion showing tumor regression 2 years later. |
 Figure 8.21. Deep capillary hemangioma in lower eyelid of infant. |
 Figure 8.22. Same patient 13 months later. The lesion has almost completely resolved. |
 Figure 8.23. Deep capillary hemangioma in medial canthal and eyebrow area of an infant. Such a lesion can simulate an ethmoidal encephalocele. |
 Figure 8.24. Seven months later, the lesion has partly resolved. |
Eyelid Congenital Capillary Hemangioma: Surgical Removal
Sometimes a capillary hemangioma can be resected entirely with a good result without waiting for it to grow to a large size.
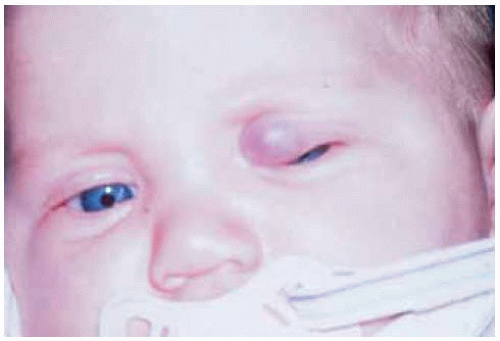 Figure 8.25. Capillary hemangioma involving deep aspect of upper eyelid nasally in an infant. The lesion was removed intact by eyelid crease incision. |
 Figure 8.26. Facial appearance of child after surgery, showing good cosmetic result. |
 Figure 8.27. Large deep upper eyelid capillary hemangioma in an infant showing complete blepharoptosis. |
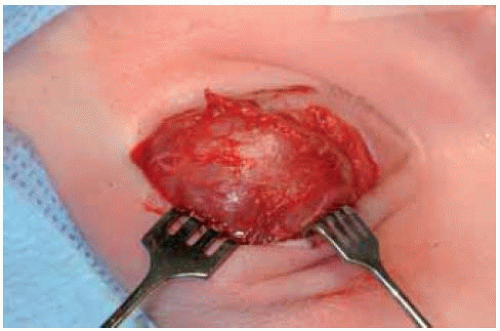 Figure 8.28. Surgical resection of tumor in patient shown in Figure 8.27 using an eyelid crease approach. |
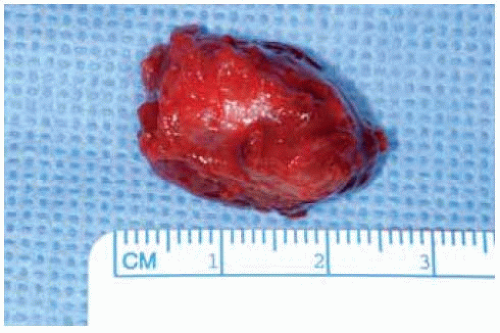 Figure 8.29. Gross specimen removed intact. |
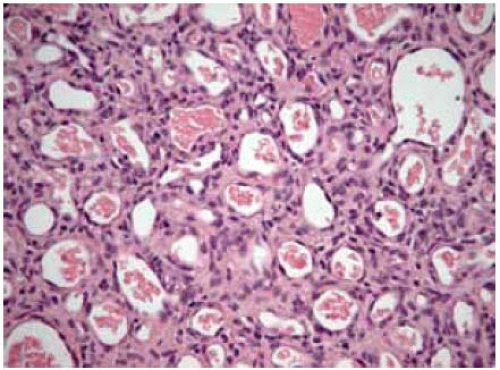 Figure 8.30. Histopathology of eyelid capillary hemangioma shown in Figure 8.29, showing fine vascular channels and proliferating endothelial cells. (Hematoxylin-eosin 75.) |
Eyelid Acquired Hemangioma (Cherry Hemangioma)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


