Jugular Foramen Tumors
CHAPTER 83
The overwhelming majority of jugular foramen tumors are benign. Only 6% of the tumors are malignant. Paragangliomas, neurogenic tumors, and meningiomas account for more than 80% of lesions of the jugular foramen (Table 83-1). In spite of the benign histologic characteristics of these tumors, all are locally destructive. These tumors are clinically silent until they eventually cause embarrassment of the vital neurovascular structures that traverse, or are in close proximity to, the jugular foramen (Table 83-1). The lower cranial nerves, the facial nerve, and audiologic and vestibular function are all potentially compromised by the slow progression of jugular foramen tumors.
The clinician’s ability to detect these lesions has been greatly enhanced with the advent and widespread availability of advanced imaging technology such as computed tomography (CT) and magnetic resonance imaging (MRI). Paragangliomas, schwannomas, and meningiomas are all known to be radioresistant. Surgery is the treatment of choice and provides the only chance of cure. With the current lateral otologic approaches of the skull base (Fig 83–1), tumor control is excellent. Surgical morbidity is minimal but is still directly related to tumor size. For this reason, prompt diagnosis and treatment of jugular foramen tumors ensure an optimal outcome for the patient.
| Tumor Type | n | % |
| Paragangliomas | n = 280 | 70 |
| Temporal bone | 240 | |
| Glomus vagale | 40 | |
| Schwannomas | n = 41 | 10 |
| IX, X | 36 | |
| XI | 1 | |
| XII | 2 | |
| Sympathetic trunk | 2 | |
| Others | n = 79 | 20 |
| Chordoma | 18 | |
| Meningioma | 10 | |
| Infralabyrinthine cholesteatoma | 10 | |
| Papillary adenoma | 8 | |
| Various malignant tumors | 24 | |
| Various benign tumors | 9 | |
| _____ | _____ | |
| Total | 400 | 100 |
Anatomy of the Jugular Foramen
The normal jugular foramen averages 15 mm in length and 10 mm in width, and the smaller pars nervosa averages 5 mm in width.1 There is a marked range in the dimensions and degree of asymmetry of the jugular foramen, due mainly to the pars vascularis. The right jugular vein and foramen are usually dominant.1
The glossopharyngeal, vagus, and cranial accessory nerves emerge in a line from along the medulla oblongata and then run laterally to the jugular foramen, where they leave the posterior cranial fossa through the jugular foramen. DiChiro et al.1 describe the foramen as a canal coursing anteriorly, inferiorly, and laterally from an intracranial to an extracranial opening. A fibrous or bony septum separates the pars nervosa, containing the petrosal sinus and glossopharyngeal nerve, from the pars vascularis, containing the vagus and the accessory nerves along with the jugular vein.
The jugular foramen is anatomically significant, as it not only acts as a conduit for vital neurovascular structures, but is surrounded by vital neighboring structures. Both tumor progression and tumor resection may pose a potential threat to these structures.
| Related to the mass effect |
| Aural (hearing loss, vertigo, tinnitus, otalgia, eustachian tube dysfunction) |
| Parapharyngeal (neck mass, parapharyngeal mass, dysphagia) |
| Neurologic |
| Lower cranial neuropathies (dysphagia, dysphonia, aspiration, shoulder weakness, dysarthria, hemiatrophy of the tongue |
| Facial nerve palsy |
| Vestibulocochlear nerve dysfunction |
| Trigeminal nerve dysfunction |
| Cerebellar dysfunction |
| Brain stem compression |
| Hydrocephalus |
| Paraneoplastic |
| Hyperdynamic state |
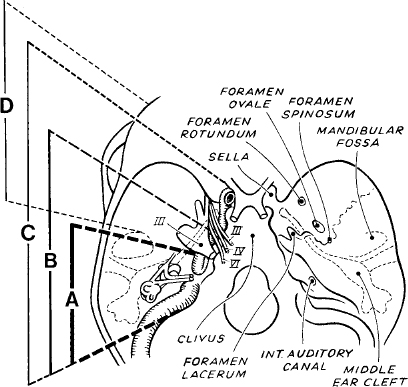
Figure 83-1 Schematic view of the lateral skull base approaches types A to D. The type A approach is the preferred access for jugular foramen tumors.
Superior to the jugular foramen lies the cerebellopontine angle, the internal auditory canal, the inferobasal otic capsule, and the middle ear. Inferiorly, the jugular foramen leads to the carotid sheath and the cervical sympathetic chain. Medially lies a partition of bone separating the jugular foramen from the hypoglossal canal. Lateral is the stylomastoid foramen and the mastoid and proximal extratemporal portion of the facial nerve. The carotid crest separates jugular foramen from the carotid foramen and artery situated more anteriorly.
Typically, there are three glomus bodies or paraganglia in each temporal bone from which paragangliomas may arise.2 The paraganglia are usually found accompanying Jacobson’s (cranial nerve IX), Arnold’s (cranial nerve X) nerve or in the adventitia of the dome of the jugular bulb. Temporal bone paragangliomas therefore more commonly originate from the jugular bulb and hypotympanum (glomus jugulare) than on the mucosa of the promontory (glomus tympanicum). Especially with large tumors, the site of origin of these tumors can often only be surmised.
Paraganglia are nonencapsulated and consist of lobules, intimately surrounded and interlaced with a rich network of capillaries. The lobules contain sustentacular cells (modified Schwann cells) and darker chief cells, arranged into groups known as Zellballen (cell balls). Derived from the neural crest, chief cells are members of the diffuse neuroendocrine system (DNES) and therefore have the capability of synthesizing catecholamines.
Schwannomas arising from the any of the lower cranial nerves will tend to expand the foramen1, 3–6 Like their vestibular counterpart, jugular foramen schwannoma arise at the transition zone between central and peripheral myelin.
With meningiomas, the jugular foramen may be the site of origin or, more frequently, may act as a conduit for the its extracranial extension. The jugular foramen and the foramen lacerum are the most common foramina, serving as pathways for the extracranial extension of a primary intracranial meningioma.
Temporal Bone Paragangliomas
Paragangliomas of the temporal bone (60%) and glomus vagale (10%) account for the vast majority of jugular foramen tumors (70%) (Table 83-1). Currently, the term paraganglioma is preferable, as it refers to the fact that these tumors arise from the paraganglia situated in perivascular locations, arising from neuroectodermal tissues. The term glomus is a misnomer and, although inaccurate, will no doubt persist.
In the head and neck, two anatomic groups of paragangliomas can be differentiated: temporal bone paragangliomas and cervical paragangliomas. Temporal bone paragangliomas can be classified as glomus tympanicum and glomus jugulare, in those cases in which the site of origin of the tumor can be determined. The term cervical paragangliomas describes glomus caroticum and glomus vagale. The jugular foramen can be affected by temporal bone paragangliomas and glomus vagale.
EPIDEMIOLOGY
Temporal bone paragangliomas are much more common than any other middle ear neoplasm. These tumors are second only to vestibular schwannoma as the most common tumor affecting the temporal bone.7 Temporal bone paragangliomas account for 15% of all neoplasms at the skull base.8 The incidence of this tumor is 1 : 1, 300, 000. The peak incidence is at 45 and 55 years of age, although this is highly variable. There is a predominant incidence in females7, 9 with a sex ratio of 4 : 1. There is no racial or ethnic predilection.
Although paragangliomas arise sporadically, a positive family history has been reported in 9.5 to 50% of patients.10–12 The mode of inheritance in the familial form is currently attributed to the genetic imprinting mode of inheritance.12
The familial form is distinct from the nonfamilial form in that there is no female preponderance, and it is associated with a higher incidence (48%) of multicentric paragangliomas.12 Multicentricity is found in about 5 to 15% of patients with the nonfamilial form. The most common second tumor is a carotid body tumor.
Pathology
Temporal bone paragangliomas are typically vascular reddish purple lobulated masses. Histologically, paragangliomas resemble paraganglia, displaying the same organoid pattern with zellballen composed of chief cell-like elements. Mitotic figures are rare. The histopathology is characterized by a rich vascularity.
Although usually histologically benign, paragangliomas of the temporal bone are characterized as locally destructive. Their growth is characteristically very slow, but rapid progression can occur and is unpredictable.13, 14 Spread occurs along the pathways of least resistance, often initially after the air cell tracts of cancellous and spongiotic temporal bone. Eventually, the tumor spreads outside the temporal bone via the jugular foramen and other neurovascular foramina.15, 16
Paragangliomas overall have an incidence of malignancy of 2 to 4%, but this is far less common with temporal bone paragangliomas than with glomus vagale tumors. There is no histologic distinction between benign and malignant lesions. Malignancy is reserved for the presence of local, regional, and distal metastases. Distal metastases occur most commonly to the lungs.
Functional activity in skull base paragangliomas is 1 to 2%.8, 17–19 In these cases, the continuous or episodic secretion of catecholamines may produce clinical symptoms mimicking a pheochromocytoma. These features include persistent or paroxysmal hypertension, tachycardia, excessive perspiration, and anxiousness. When manipulated surgically, catecholamine-secreting paragangliomomas can potentially initiate a life-threatening hypertensive crisis, constituting an anesthetic emergency.
Paragangliomas of the temporal bone are associated with other neoplasms, both benign and malignant, in 7% of patients.7 Tumors most commonly associated are pheochromocytomas, thyroid C-cell carcinoma, parathyroid adenomas, and visceral neoplasms of neural crest origin. There is also a reported association with the multiple endocrine neoplasm (MEN) syndromes.
STAGING
Fisch staging of temporal bone paragangliomas classifies these paragangliomas according to the extent of the tumor on imaging. Each of the four categories of tumor requires a different therapeutic approach. Tympanic, tympanomastoid, infralabyrinthine and intracranial tumors are described as class A, B, C, and D, respectively20–23 (Table 83-3).
CLINICAL PRESENTATION
The presentation of temporal bone paragangliomas is characterized by an insidious onset, and the slow progression of symptoms. Glomus jugulare tumors arising from the jugular foramen tend to be clinically silent until they eventually embarrass the function of the lower cranial nerves and encroach on the middle and inner ear.
At presentation, almost all patients have developed hearing loss (83%) and pulsatile tinnitus (83%).16, 24 The hearing loss is initially conductive in nature, with sensorineural hearing loss the hallmark of labyrinthine invasion. Patients may also complain of aural discharge, otalgia, and aural fullness.
| Class A: Tumor limited to the middle ear cleft Class B: Tumor limited to the tympanomastoid area without destruction of bone in the infralabyrinthine compartment Class C: Tumor extending into, and destroying, bone of the infralabyrinthine and apical compartments of the temporal bone |
| C1: Tumor erodes the carotid foramen, but does not invade the carotid artery C2: Tumor destroys the vertical carotid canal between the carotid foramen and the carotid bend C3: Tumor extends along the horizontal portion of the carotid artery but does not reach the foramen lacerum C4: Tumor grows to the foramen lacerum along the carotid artery to the cavernous sinus |
| Class D: Tumor with intracranial extension De1: Tumor with intracranial extradural extension 2 cm in diameter De2: Tumor with intracranial extradural extension 7 2 cm in diameter Di1: Tumor with intracranial intradural extension 2 cm in diameter Di2: Tumor with intracranial intradural extension 7 2 cm in diameter D3: Tumor with inoperable intracranial extension |
Symptoms related to the lower cranial neuropathies, such as dysphonia (44%), dysphagia (36%), and shoulder weakness (33%), indicate significant jugular foramen involvement.24 Because the onset of these lower cranial nerve palsies often occurs over years, excellent compensation is common at presentation.24–26 Facial nerve weakness (33 to 36%) invariably indicates neural infiltration, usually in the mastoid portion.24, 27
Physical examination consists of a complete otologic, head and neck, and cranial nerve examination. The hallmark of a temporal bone paraganglioma tumor is a red or reddish blue mass hypomesotympanic (70%) seen behind the tympanic membrane, referred to as the “sunset sign.”26 An aberrant carotid artery or a high jugular bulb may mimic this otoscopic appearance. In rare cases, a friable bleeding polyp in the external auditory canal may be the presenting sign of lateral growth of the tumor.26 The neck is examined for bruits, concurrent tumors of the carotid body, vagus, thyroid, and parathyroid. Cervical lymphandenopathy may indicate malignant paraganglioma.
INVESTIGATION
The diagnosis of temporal bone paraganglioma is made on clinical evaluation, in collaboration with imaging. Biopsy of the tumor is unwarranted, with the undue risk of hemorrhage. Audiologic function is documented with an audiogram. Screening for urine catecholamine metabolites (vanillylmandelic acid [VMA], normetanephrine, and metanephrine) is recommended only for those patients with hypertension and for those with pheochromocytoma-like symptoms.
When urinary catecholamine levels are elevated, a search should be undertaken for other functional tumors, including pheochromocytomas.28 The search to localize other catecholamine-secreting paragangliomas may require comprehensive MRI, 131-metaiodobenzylguanidine nuclear scanning, and selective catheterization for venous samples for plasma norepinephrine determination.29
CT scan provides precise evaluation of bony destruction and erosion, which is a hallmark of temporal bone paragangliomas (Table 83-4). Destruction of the infralabyrinthine compartment and the anterolateral base of the skull determines the stage of temporal bone paraganglioma.20, 30 Temporal bone CT also provides useful preoperative information about the position of the jugular bulb, and the size and presence of the contralateral sigmoid sinus. Any evidence of erosion into the basal turn of the cochlea allows the surgeon to warn the patient of the attendant high risk of sensorineural hearing loss.
Complementing the CT evaluation of bone destruction, MRI with gadolinium-DPTA enhancement offers superior soft tissue resolution and differentiation. MRI confirms the diagnosis of paraganglioma with a typical salt-and-pepper appearance. MRI is also important in determining the intracranial extension of the tumor (intra- or extradural) and extension into the cavernous sinus.
Angiography confirms the diagnosis with its characteristic rapid vascular blush. It is also important in determining the blood supply and angioarchitecture of the tumor, as well as the integrity of the internal carotid artery and the collateral circulation.
For large temporal bone paragangliomas in which the pre-operative imaging indicates encasement or invasion of the internal carotid artery, permanent preoperative balloon occlusion should be considered.22, 31, 32
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


