(1)
Narayana Hridayalaya Multispeciality, Bangalore, India
Thyroid
Surgical Anatomy and Pathology
Thyroid surgery is one of the more commonly performed head–neck surgical procedures. It is performed for a wide variety of indications ranging from benign neoplasm of thyroid to malignant tumors. Thyroidectomy is also performed by clinicians practicing in different setups with varying resources. Though it is a relatively simple procedure, it has the potential to cause life-threatening complications. Appropriate exposure, understanding of the anatomy of recurrent laryngeal nerve and parathyroid gland, and the ability to secure hemostasis in a relatively narrow space are key in obtaining a successful outcome.
Figure 3.1 demonstrates the schematic anatomy of the thyroid and parathyroid gland. The relation of the recurrent laryngeal nerve to the inferior thyroid artery and parathyroid gland forms the backbone for surgical safety. The inferior thyroid artery most of the time passes over the recurrent laryngeal nerve and divides into multiple branches. It is essential to locate the recurrent laryngeal nerve first and then ligate the terminal branches of the inferior thyroid gland close to the gland where it enters the gland. The parathyroid gland should be preserved with its blood supply.
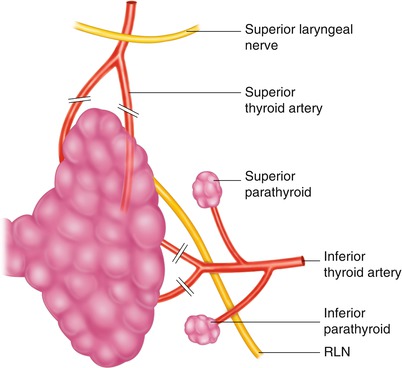
Fig. 3.1
Anatomy for thyroid surgery
Figure 3.2 demonstrates algorithm for management of thyroid diseases.
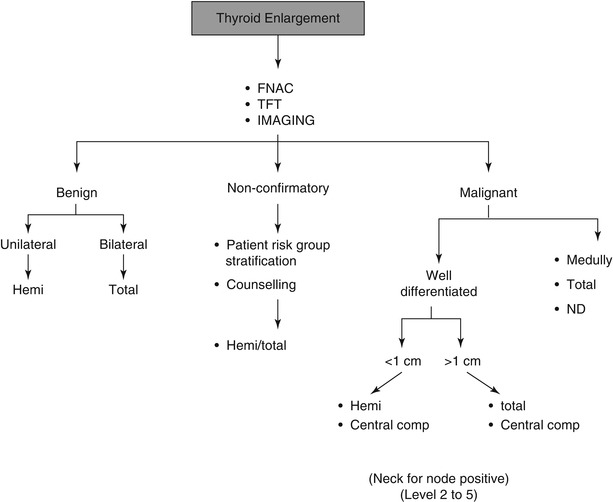
Fig. 3.2
Algorithm for management of thyroid diseases
Hemithyroidectomy
1.
Unilateral benign lesions
2.
Well-differentiated malignant thyroids less than 1 cm size
Total Thyroidectomy
1.
Bilateral large benign lesions
2.
Malignant lesions (>1 cm)
Indications for sub-total and near total thyroidectomy are rare in current day practice.
This chapter focuses on the technical aspects of performing thyroid surgeries.
A.
Thyroidectomy
B.
Thyroidectomy with tracheal resection
C.
Thyroidectomy with sternotomy for retrosternal goiter
Thyroidectomy

Fig. 3.3
Demonstrates the position of the patient for any thyroid procedure. It is essential to achieve as much neck extension as possible with the use of a shoulder bag and head ring

Fig. 3.4
Demonstrates surface marking for the incision. Transverse lower cervical incision about 2 cm above the suprasternal notch is preferred for thyroid surgeries. This gives better exposure, avoids the need for retraction of the lower flap, and provides better cosmesis. Infiltration of xylocaine–adrenaline solution 10 min before the start of the procedure helps in achieving better hemostasis while raising flaps
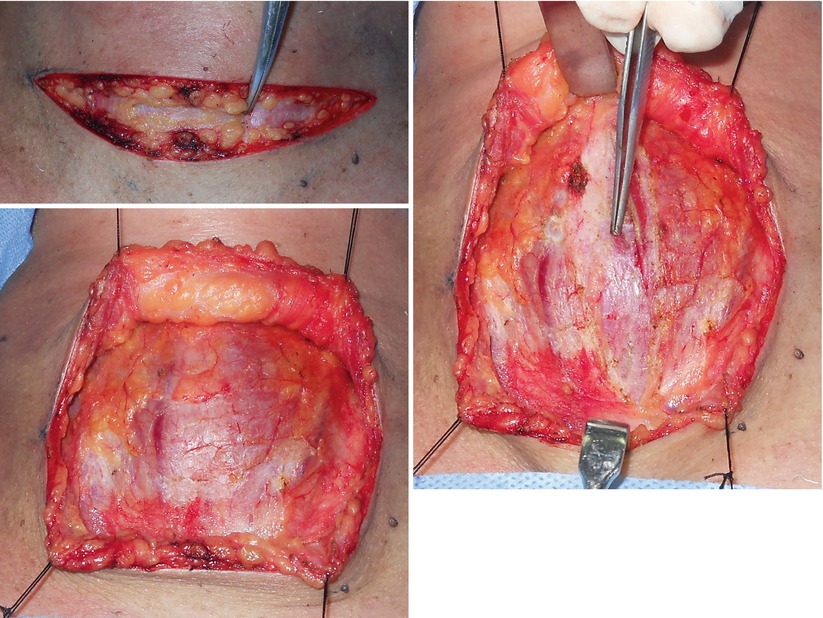
Figs. 3.5, 3.6, and 3.7
Demonstrates the anatomy of the platysma in the anterior neck. The platysma is absent in the midline in the lower neck, and it is advisable to incise the platysma on the lateral aspect to find the subplatysmal plane and raise the entire upper flap in the same plane (Fig. 3.6). Deep fascia above the strap muscle is divided in the midline to expose and separate the strap muscle from either side (Fig. 3.7)
Figs. 3.8 and 3.9
Demonstrates the division of strap muscles to expose the thyroid gland. Sectioning of the strap muscle is advisable for larger and more vascular thyroid lesions and for surgeons in training period. This approach allows better exposure for dissection of the recurrent laryngeal nerve (RLN) and parathyroid glands. Muscle should be cut as high as possible to preserve its nerve supply. Care should be taken not to damage small veins on the surface of the thyroid gland while retracting the strap muscle and exposing gland (Fig. 3.9). The middle thyroid vein is secured first while mobilizing the thyroid gland
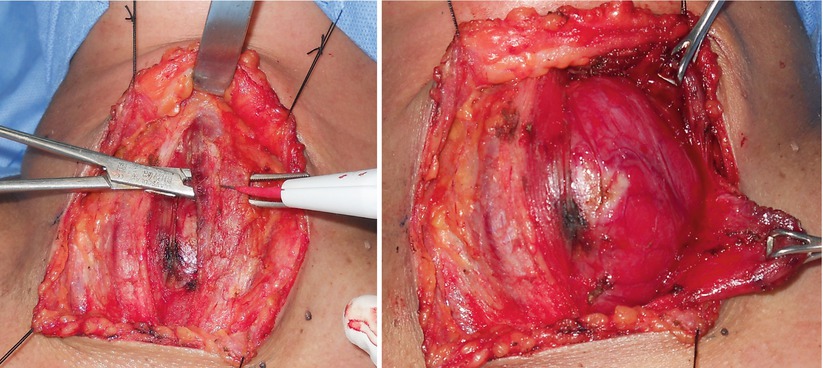
Figs. 3.10 and 3.11
Demonstrates the position of the superior thyroid pedicle in relation to the thyroid gland. This is one of the important steps for this procedure, and proper exposure to this area is essential to secure hemostasis. Two retractors are placed to expose the medial and lateral aspects of the superior thyroid pedicle. Fig. 8a shows the anterior and posterior branch of this pedicle running on the surface of the thyroid gland. The pedicle should be ligated as close to the thyroid gland as possible to avoid injury to the external laryngeal nerve. I prefer not to dissect the external laryngeal nerve and stay close to thyroid gland to avoid injuring it (Fig. 3.11)
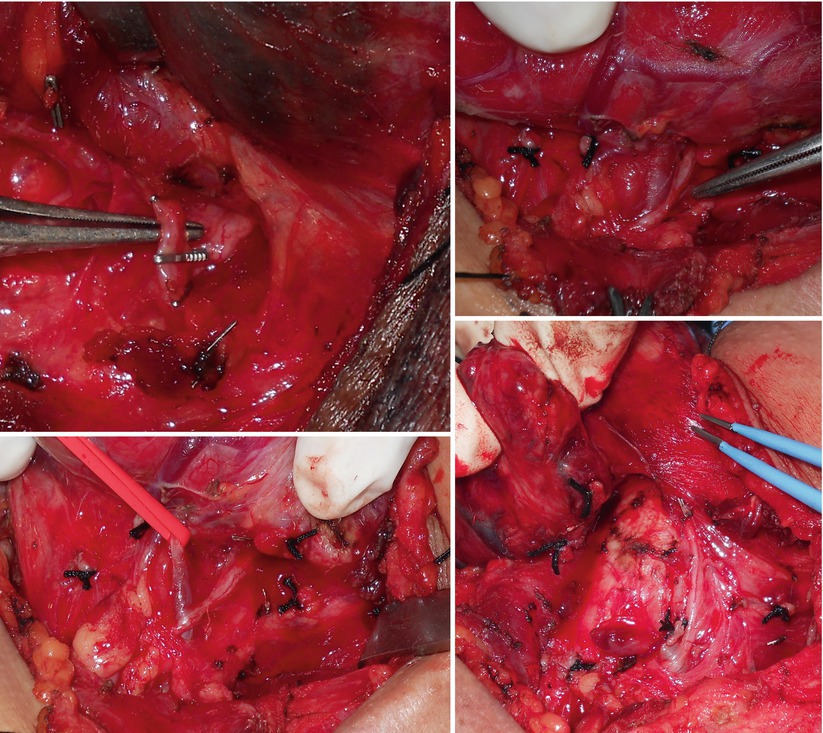
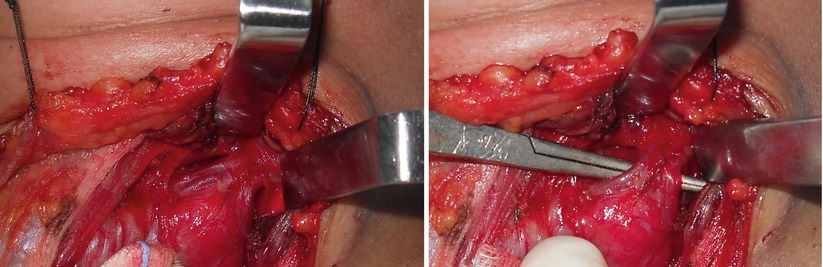
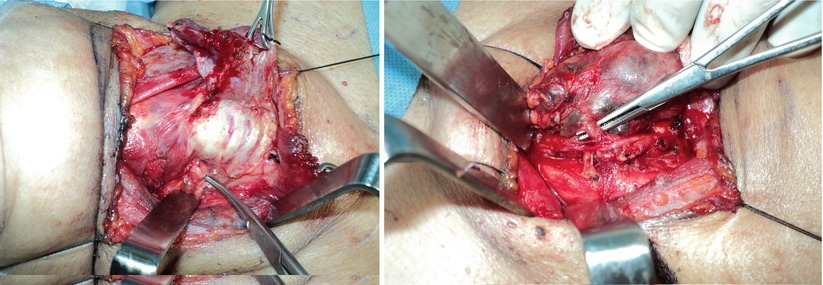
Figs. 3.12, 3.13, 3.14, and 3.15
Demonstrate the anatomy of the RLN in relation to the inferior thyroid artery and parathyroid glands. Fig. 3.12 shows the recurrent laryngeal nerve passing below the inferior thyroid artery which is the usual anatomy in this region. Fig. 3.13 shows variation of this anatomy where the RLN passes above the inferior thyroid artery. One needs to identify this relation before ligating the inferior thyroid artery. It is always advisable to ligate branches of the inferior thyroid artery after it crosses the RLN to prevent injuring the nerve. Figs. 3.14 and 3.15 show the inferior parathyroid gland with separate blood supply from the inferior thyroid artery. It is essential to preserve the parathyroid gland with its blood supply. Ligating only those branches of the inferior thyroid artery that enters the thyroid gland (near the thyroid gland) ensures preservation of functioning parathyroid gland
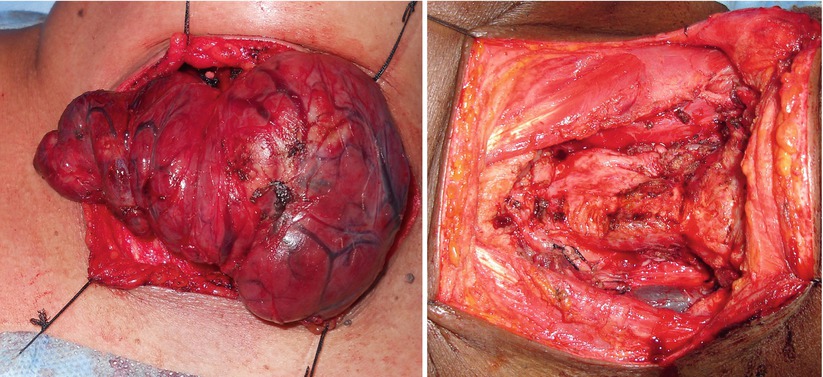
Figs. 3.16 and 3.17
Demonstrate completed total thyroidectomy. Strap muscles are sutured back to its original position. Appropriate drains are kept and closure is done. It is also advisable to remove the shoulder bag and keep neck in flexion for 10 min to check for hemostasis before starting wound closure
Thyroidectomy with Tracheal Resection
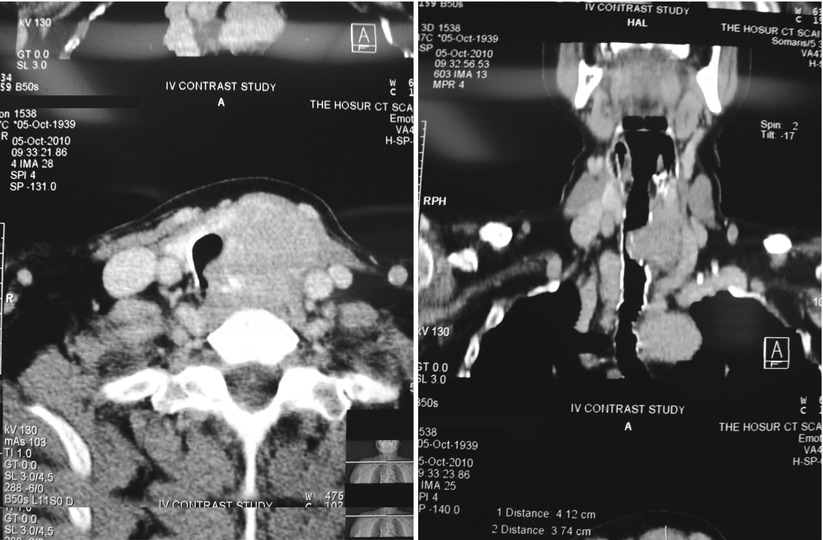
Figs. 3.18 and 3.19
Show computed tomography scan (CT scan) images of a patient of papillary carcinoma thyroid infiltrating the trachea. The left lobe of the thyroid is enlarged and has infiltrated the tracheal wall and entered into the lumen. It is very important to evaluate the level of this infiltration in relation to the cricoid cartilage. This CT scan image shows that tumor doesn’t involve the cricoid cartilage and first tracheal ring. This implies that we can have adequate margin of the trachea above and below without having to resect the cricoid cartilage. In case the cricoid cartilage is involved, total laryngectomy needs to be performed. Another important fact is the extent of tracheal involvement. Around 5–6 tracheal rings can be resected without much impact on tracheal anastomosis. Tumor infiltrating more length of the trachea needs more careful planning and may need extensive mobilization of the trachea or alternative method of reconstruction

Fig. 3.20
Shows surface marking of the thyroid and cricoid cartilage and planned incision site
Figs. 3.21 and 3.22
Shows dissection of the recurrent laryngeal nerve and inferior thyroid artery as described in the previous section of this chapter
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


