(1)
Narayana Hridayalaya Multispeciality, Bangalore, India
Surgical Anatomy
The oropharynx is one of the most complex anatomical sites in the head and neck region. It consists of various subsites – base of the tongue (BOT), tonsil, soft palate, and pharyngeal wall (Fig. 9.1). Tumor in each of these subsites has different biology but is grouped as one in majority of the head and neck studies. The oropharynx forms circular envelop in posterior aspect of oral cavity working as an inlet for pharynx. The base of the tongue is the most inferior structure and is in close relation to the hyoid bone inferomedially and lateral pharyngeal wall and tonsil laterally. The tonsil occupies lateral position and is connected inferiorly to BOT and superiorly to the soft palate. It is separated by the medial pterygoid muscle by a fascia, and this plane can be exposed to resect early oropharyngeal lesions. The soft palate hangs on top of the pharynx inlet and is important in speech and swallowing.
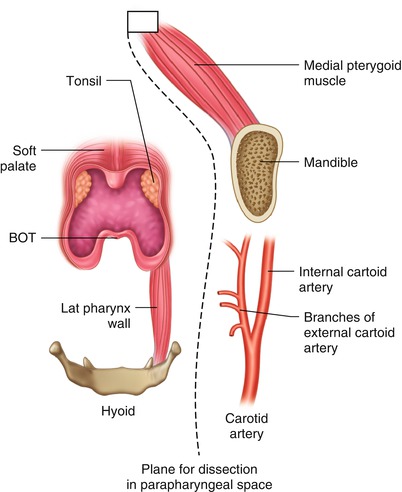
Fig. 9.1
Surgical anatomy of the oropharynx
The oropharynx is supplied by branches of the external carotid artery which traveres the parapharyngeal space. This space can be exposed to clear the lateral margin that is the deep margin for oropharynx tumors.
Surgical Pathology
The early lesions of oropharynx are generally confined to the pharyngeal wall and spread laterally to neighboring subsite. Their lateral spread is limited by the parapharyngeal space. These early lesions can be resected by entering the parapharyngeal space and mobilizing the lesion from deep to superficial. This also helps in controlling bleeding as branches of the external carotid artery are already ligated.
The advanced lesions of the oropharynx pose a difficult surgical challenge. The anatomy is multidimensional and tumor spread involves critical areas. The spread can be in two directions (Fig. 9.2). The superior and lateral spread is towards the ITF. The medial pterygoid muscle is the first one to be involved, and the tumor can spread further to high ITF. The second ie inferior spread is directed medially towards hyoid bone. The surgical resection can be planned depending upon the compartment involved. The resection includes the base of the tongue when spread is inferior and ITF when spread is superior. Both compartments need to be resected for very advanced tumors.
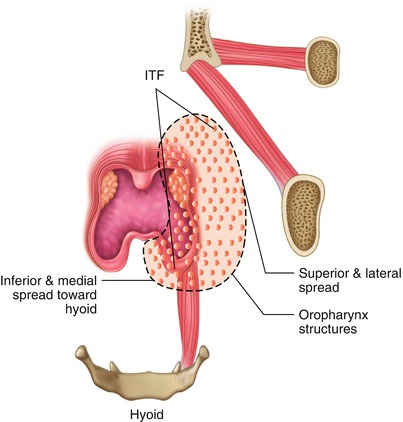
Fig. 9.2
Pattern of disease spread outside the oropharynx
Figure 9.3 demonstrates the treatment algorithm for management of oropharynx tumors. The oropharynx is essentially managed by a nonsurgical approach in current era of human papilloma virus (HPV), and surgery is generally reserved for recurrent cases. However, surgery can still be considered as one of the options in primary treatment. The newer surgical techniques in the form of robotic surgery and endoscopic laser surgery have again shifted the focus towards surgical approach. This chapter essentially focuses on the conventional open surgical approach for treatment of these tumors. The advanced tumors generally respond well to nonsurgical treatment compared to other subsites, though certain infiltrative and very advanced lesions do much better with upfront surgery.
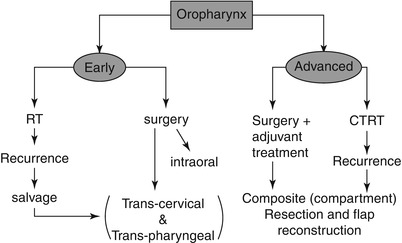
Fig. 9.3
Algorithm for treatment of oropharynx
Surgical Concepts
The lateral pharyngeal wall forms the deep margin for oropharynx tumor. This space can be exposed and cleared to achieve negative margins.
The advanced tumors have two potential ways for spread. The superior and lateral spread is towards the ITF, and this can be cleared with compartment clearance. The inferior spread is towards the hyoid bone and can be addressed by resecting the base of the tongue area.
The mandibulotomy approach has been traditionally used to address large oropharynx tumors. This is becoming less popular and these tumors can be addressed by combination of transpharyngeal and transoral approaches.
The anatomy of the parapharyngeal space is of paramount importance, and mobilization begins with clearing this area. Once the base is mobilized, the involved compartments can be addressed.
The SND is performed on the same side for lateralized lesions, while bilateral neck dissection is done for more centralized lesions.
Early Lesion
This procedure demonstrates resection of early oropharynx tumor with transcervical–transpharyngeal approach. These tumors can be addressed by open intraoral approach or by robotic assisted surgery. We come across many patients in clinical practice who come with trismus due to sub-mucus fibrosis, and these can be best addressed by the transpharyngeal approach.


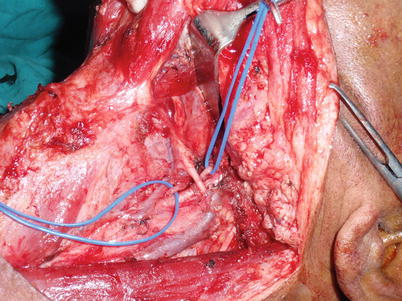
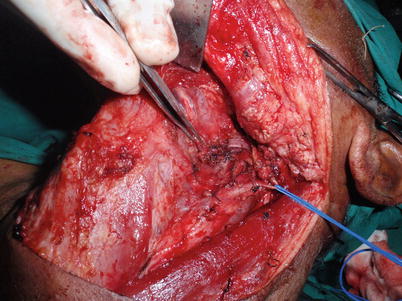
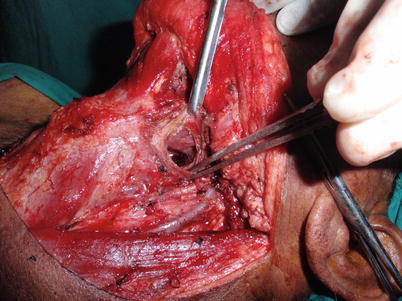
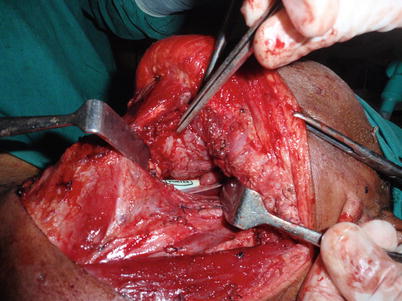




Fig. 9.4
SND level I to IV is complete
Fig. 9.5
The digastric muscle is cut
Fig. 9.6
The branches of the external carotid artery are identified and ligated. There are parapharyngeal veins coming from the IJV that needs to be secured as well
Fig. 9.7
The ligated branches of ECA are retracted laterally to expose the parapharyngeal space. The dissection can run upwards to separate the medial pterygoid muscle from tonsil and lateral pharyngeal wall. This provides complete exposure of oropharynx subsites and achieves clearance in depth
Fig. 9.8
The pharynx is opened from BOT area
Fig. 9.9
The tumor involving the BOT can be seen in this photograph. The tumor can be palpated all around, and wide excision can be performed under control. The resection for superficial lesions need not involve removal of the entire BOT muscle but selective excision of the involved area. This helps in preserving the function
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
