(1)
Narayana Hridayalaya Multispeciality, Bangalore, India
Surgical Anatomy and Pathology
The larynx is one of most critical organ in the human body responsible for voice production. The larynx is subdivided into supraglottis, glottis, and subglottis. The tumor from each subsite has different biological behavior and has different pattern of spread. The supraglottic tumor has higher tendency to have lymphatic spread compared to glottic tumor. Treatment algorithm for laryngeal cancer has changed significantly with majority of tumors being treated by nonsurgical organ preservation approach. Early laryngeal lesions are managed either by radiotherapy or by endoscopic laser surgery. The minimally invasive surgery is beyond the scope of this book. The moderately advanced tumors are managed by concurrent chemoradiotherapy in majority of cases. The conventional total laryngectomy (TL) can be offered to this group in select cases. The very advanced tumors require TL and voice rehabilitation with tracheoesophageal prosthesis (TEP). Open conservative laryngeal procedures have become almost obsolete with the advent of endoscopic laser procedures and concurrent chemoradiotherapy regimens. Near total laryngectomy (NTL) is almost like total laryngectomy but voice quality is inferior to TEP and majority of clinicians prefer TL with TEP over NTL.
The management of hypopharynx tumor is almost similar to laryngeal tumor with majority of lesions treated with chemoradiotherapy. The hypopharynx tumors have poor biology with the tendency for distant metastasis. These tumors are known for their submucosal spread and skip lesions in adjacent areas. These factors should be kept in mind while performing the surgery. Total laryngectomy with partial pharyngectomy is the standard operation for the majority of pyriform fossa tumors. The advanced post-cricoid tumors require total laryngopharyngectomy with or without esophagectomy depending upon the lower extent of tumor spread.
There are many issues to discuss in the treatment of the larynx and hypopharynx cancer, but the focus of this book is on surgical approach, and the following procedures will be discussed in this chapter:
1.
Total laryngectomy
2.
Total laryngopharyngectomy
3.
Repair of pharyngeal fistula
Total Laryngectomy
This section deals with TL procedure for a case of advanced cancer of the larynx.

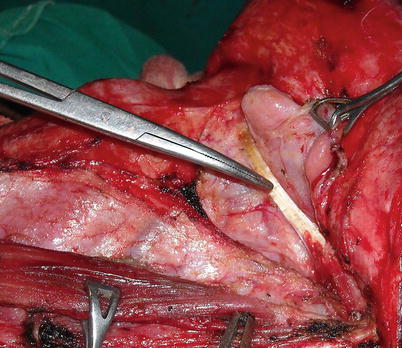
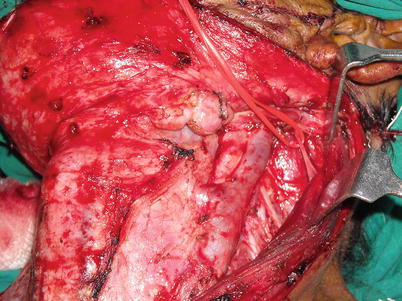
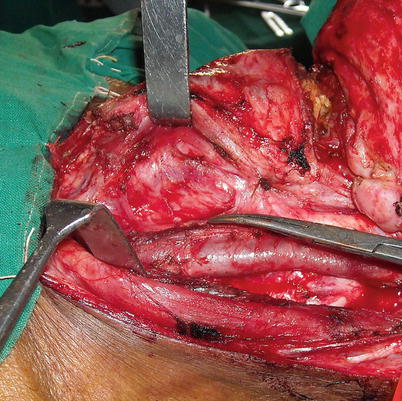
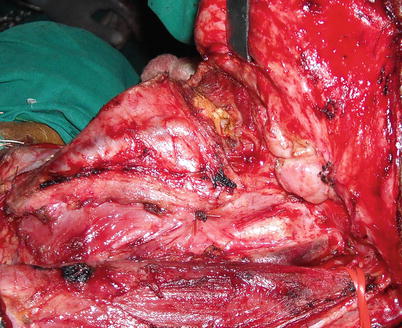
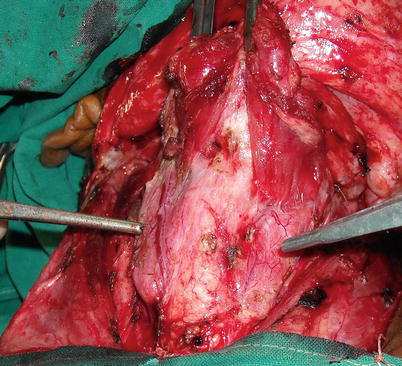
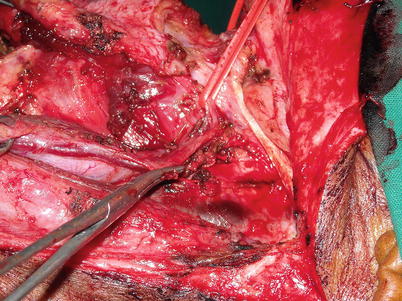
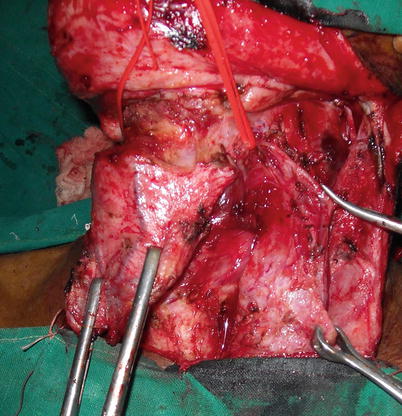
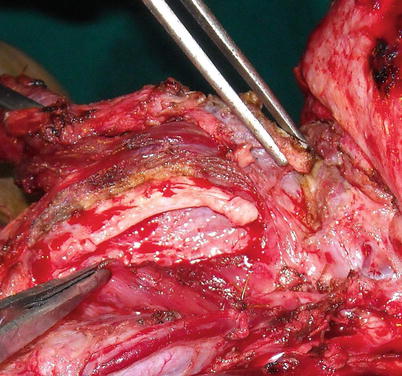

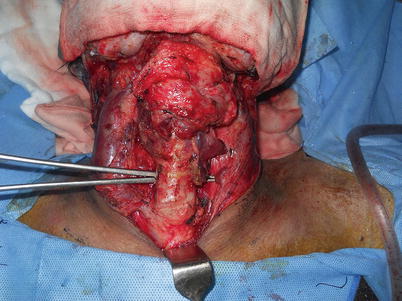
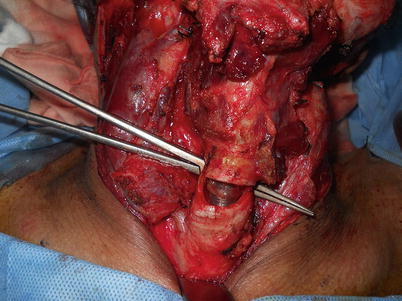
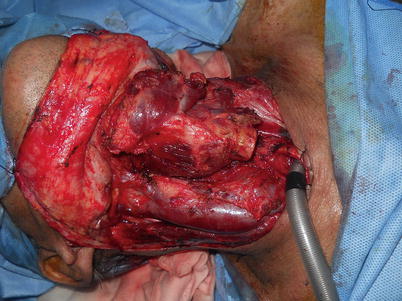




Fig. 10.1
The U-shape incision for TL. Alternatively one can use transverse incision
Fig. 10.2
The flap is raised till the digastric muscle is exposed in its entire length
Fig. 10.3
The SND level II to IV is performed
Fig. 10.4
The carotid artery is separated from the thyroid gland and cartilage
Fig. 10.5
The hyoid bone is exposed
Fig. 10.6
The strap muscle is divided above the trachea and the thyroid gland is exposed. It is a standard practice to save the thyroid gland on the contralateral side. When both lobes of the gland are involved in the tumor, efforts are made to save the parathyroid glands on either side
Fig. 10.7
Pedicle of the superior thyroid is dissected. Branch supplying strap muscle is clipped
Fig. 10.8
The gland is lateralized away from thyroid cartilage with intact vascular pedicle
Fig. 10.9
The lateral border of thyroid cartilage is dissected and pyriform fossa mucosa is exposed. This maneuver is done on the side where the disease is not there we can preserve pharyngeal mucosa on non-disease side this way. The pharynx cavity is entered from normal side
Fig. 10.10
The lower end of trachea is exposed to perform end tracheostomy
Fig. 10.11
Proposed site for tracheostomy. In cases where subglottis has significant disease extension, this site can be much lower and care should be taken to have a secure lower end of the trachea
Fig. 10.12
The anesthetic tube should be de-cuffed and withdrawn before cutting the trachea. Try and have cut curving upwards in the posterior wall for easy suturing of stoma
Fig. 10.13
The lower end of the trachea is sutured to the chest wall, and an endotracheal tube is shifted to this end. The sterile endotracheal tube should be ready before transecting the trachea
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
