Tumors of the Facial Nerve
Michael J. McKenna
K. Paul Boyev
The facial nerve may be involved by both benign and malignant neoplasms. Although the resulting symptoms maybe similar, the management and prognosis are different. The successful management is dependent upon an accurate and early diagnosis.
The most common benign neoplasms that arise from the facial nerve are schwannoma, neurofibroma, and hemangioma. Other benign neoplasms that may affect the facial nerve include paraganglioma, meningioma, endolymphatic sac tumor, epidermoid tumor, and vestibular schwannoma. The facial nerve may also be involved by a variety of malignant processes, including squamous cell carcinoma, adenocarcinoma, sarcomas, adenoid cystic carcinoma, mucoepidermoid carcinoma, and hemangiopericytoma. The successful treatment is dependent upon establishing an accurate diagnosis, acquiring a knowledge of the natural history of the disease process, determining the extent of involvement, and determining the age and general health of the affected individual. In general, the management of malignant tumors involving the facial nerve is based upon oncologic principles of control or cure of the underlying malignancy. Early surgical intervention with sacrifice of the facial nerve is indicated when a possible cure can be accomplished. The management of benign neoplasm involving the facial nerve requires a more thoughtful consideration. Ultimately the best approach depends upon the natural history of neoplasm, the degree of symptomatology, and the patient’s own desire following a discussion of realistic expectations for recovery of function with intervention, both immediate and delayed.
DIAGNOSIS
The most common presenting symptom of both benign and malignant tumors involving the facial nerve is a gradual progressive paresis and paralysis occurring over a period of weeks to months. Approximately 5% of all lower motor neuron facial palsies are secondary to facial nerve tumors (1). The time course over which the paresis or paralysis occurs is often the most important clinical feature in differentiating a neoplastic process from the more sudden paresis characteristic of Bell’s palsy. The gradual onset of paresis is the presenting symptom in approximately 60% of patients. However, a sudden paralysis similar to Bell’s palsy may also occur in 10% to 20% of cases (2,3). In addition, some benign neoplasms may present with transient paresis. Approximately 30% of patients with facial nerve schwannomas have normal facial function at the time of diagnosis (3). An accurate and timely diagnosis is dependent upon an index of suspicion and a careful and complete clinical evaluation.
The presence of auditory or vestibular symptoms should raise the index of suspicion. A history of malignant disease, either local or distant, could indicate possible metastatic involvement of the facial nerve. This is especially true for cutaneous malignancies involving the face, head, and neck, which may readily metastasize or spread to involve the facial nerve by perineural extension.
A complete head and neck, otologic, and neurotologic evaluation is paramount in the evaluation of patients with facial paralysis. Involvement of a single branch of the facial nerve, with sparing of others, should also raise concern of an underlying neoplasm.
Audiometry may be useful in establishing the presence of an ipsilateral conductive or sensorineural hearing loss. Hearing loss of either type is present in 28.5% (4) to 49% (3) of patients with schwannomas of the facial nerve. Electroneuronography is also useful both from a diagnostic and prognostic standpoint once a diagnosis is established and surgery is being considered.
RADIOGRAPHIC EVALUATION (FIG. 43.1)
Any patient who is suspected of having a neoplasm of the facial nerve should undergo radiographic evaluation with both high-resolution temporal bone computed tomographic (CT) scan and gadolinium-contrast magnetic resonance imaging (MRI) (5). The MRI scan with gadolinium can demonstrate abnormal enhancement of the facial nerve from the brainstem to the periphery. Because patients with idiopathic facial paralysis often have abnormal enhancement of the facial nerve
centered in the geniculate area and extending both anterograde and retrograde into the tympanic cavity and internal auditory canal, it may be difficult on the MRI scan alone to differentiate this enhancement from that which is seen in cases of facial nerve schwannomas. The CT scan is often useful in evaluating for the presence of bone erosion in the region of geniculate fossa and labyrinthine segment, which may occur with a facial nerve schwannoma or geniculate hemangioma.
centered in the geniculate area and extending both anterograde and retrograde into the tympanic cavity and internal auditory canal, it may be difficult on the MRI scan alone to differentiate this enhancement from that which is seen in cases of facial nerve schwannomas. The CT scan is often useful in evaluating for the presence of bone erosion in the region of geniculate fossa and labyrinthine segment, which may occur with a facial nerve schwannoma or geniculate hemangioma.
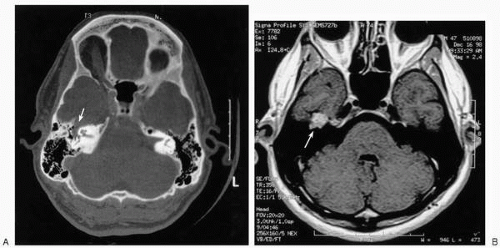 FIG. 43.1 A: Axial CT scan with bone window technique demonstrating an expansile lesion in the area of the geniculate ganglion on the left (arrow). Patient had a history of progressive facial paresis. The cause was hemangioma. B: Axial T1 gadolinium-enhanced image of the same patient shows enhancement of the lesion (arrow). |
Ultimately the diagnosis of a primary facial nerve tumor is made on the basis of clinical evaluation and radiographic studies. Although it might be tempting to biopsy a primary facial nerve tumor to establish the histologic diagnosis, this will often result in immediate facial paralysis and should be avoided if possible (6). Facial nerve tumors involving the tympanic segment of the facial nerve may present initially as a mass within the middle ear, with conductive hearing loss. Although not a common postmortem finding, Zhang et al. (7) found 12 asymptomatic tympanic segment schwannomas in a collection of 1,526 temporal bones. Often the diagnosis is difficult to establish solely on the basis of exam and radiographic studies, especially when there is no evidence of preoperative facial nerve dysfunction. An accurate diagnosis may be further clouded by a concurrent problem with chronic otitis media secondary to eustachian tube dysfunction.
DIFFERENTIAL DIAGNOSIS
The most common tumors of the facial nerve are schwannoma, followed by hemangioma. These benign lesions must be differentiated from other benign and malignant lesions of the temporal bone, such as meningioma, vestibular schwannoma, primary epidermoid tumor, paraganglioma, and metastatic lesions. To some extent, schwannomas and hemangiomas exhibit distinct proclivities for certain anatomic sites along the facial nerve (3,4,8, 9, 10) (Fig. 43.2). Characteristic radiographic features of each are often helpful in establishing a differential diagnosis (11). However, definitive diagnosis can only be established at surgical exploration.
MANAGEMENT
At present there is no role for medical management of benign neoplasms of the facial nerve. However, in the future, the use of antiangiogenetic factors may possibly play a role for vascular neoplasms affecting the facial nerve, such as paragangliomas and hemangiomas. There is no evidence at present to support the use of radiation therapy as a primary treatment modality for benign facial nerve tumors (12).
The surgical management of malignant lesions can be divided into palliative and curative procedures. The preservation of facial nerve integrity and function may be a primary goal of palliative procedures. Curative procedures for malignant lesions involving the facial nerve may require sacrifice of the facial nerve. Because many malignant lesions have a tendency for perineural invasion and spread, reconstructive efforts with cable grafting should make use of intraoperative frozen sections to be certain that both the proximal and distal segments of the nerve are free of disease. Often, extensive malignant disease precludes the use of cable grafting, and other alternative forms of facial reanimation may be
necessary. Adjunctive therapy with either chemotherapy or radiation should not be delayed even if a cable graft is used. These patients should undergo a baseline imaging study with CT, MRI, or both in the early postoperative course, which will serve as a baseline for surveillance for possible recurrence.
necessary. Adjunctive therapy with either chemotherapy or radiation should not be delayed even if a cable graft is used. These patients should undergo a baseline imaging study with CT, MRI, or both in the early postoperative course, which will serve as a baseline for surveillance for possible recurrence.
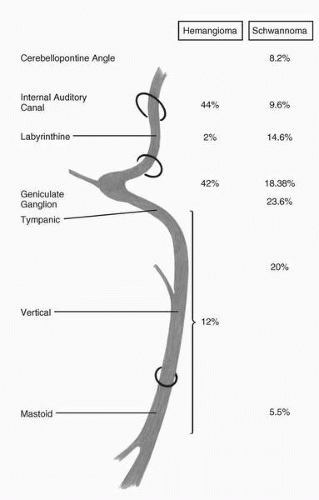 FIG. 43.2 Distribution of hemangiomas and schwannomas along the facial nerve. Approximately 90% of hemangiomas occur between the internal auditory canal and tympanic segment, whereas schwannomas tend to be more evenly distributed. |
The most critical aspect of preoperative planning for surgical management of benign facial nerve tumors surrounds the timing for intervention and should be individualized based on the degree of preoperative impairment, amount of neuronal degeneration as determined by electroneuronography, progression of auditory and vestibular dysfunction, and the patient’s own desires. Although some facial nerve hemangiomas can be resected in a manner that maintains facial nerve integrity and continuity, it is more common that a portion of the facial nerve must be resected, which necessitates a cable graft (8). The central dilemma of planning surgical intervention is timing: The operation needs to take place while conditions for maximizing postoperative cable graft function are optimal; however, during this window, the patient’s level of function is usually better than the best expected cable graft outcome. It has been our philosophy to wait until there is evidence of noticeable progression of symptoms but to recommend surgical intervention before residual facial neuronal function drops below 40% on electroneuronography. Our results and the results reported by others indicate that the best possible recovery is a House-Brackmann grade III, with most patients ending up with House-Brackmann grade IV (13). Because the final recovery is often poorer than the preoperative facial function, the patients need to have a clear understanding of the goals of the proposed surgical procedure and realistic expectations prior to surgery. Patients should undergo both still and video photography prior to surgery. We have also found it helpful for patients to view photographs and videos of other patients who have undergone similar procedures so that they can gain a realistic expectation of the degree of recovery that might be expected in their case.



