Reconstruction of Congenital Auricular Malformations
Roland D. Eavey
GENERAL CONSIDERATIONS
The form of the external ear is so closely associated with otorhinolaryngology that a simple line drawing of the auricle serves as a symbol of the specialty. Paradoxically, however, effective correction of malformations of the auricle has not been possible until recently. The otolaryngologist who trains to correct this malformation is in a fine position to serve the patient, because both hearing and aesthetic issues, as well as associated conditions such as facial paralysis, can be addressed. The counseling and treatment that must be provided are long term, starting shortly after birth.
Embryologic development of the ear is extremely complex (1, 2, 3, 4, 5), involving multiple types of tissue such as skin, fat, cartilage, bone, blood vessels, nerve, and mucous membrane. Ectoderm and mesoderm are involved in the development of the auricle. In addition to these basic tissue elements, the temporal bone also contains endodermal primordia. The auricle is the product of the maturation of six hillocks originating from the mandibular and hyoid arches. These hillocks coalesce by the third fetal month. The first branchial (mandibular) arch is the origin of the tragus. The second (hyoid) arch produces the other five hillocks that then generate the remainder of the auricle. The branchial groove between the two arches invaginates to produce the external auditory canal.
The range of auricular malformations is extensive. For example, the ears merely can be malpositioned or low set. Other minor malformations can occur as noted in Fig. 45.1 (6). More severe malformations of the auricle may be present that exhibit extensive cartilage deformity but preserve a meatus and canal (Fig. 45.2). In the typical microtia malformation, the external ear is severely deformed, with no canal, meatus, or tragus. The auricle is most commonly reduced in size and vertically oriented in an abnormal position. In the typical case, there is an amorphous rudimentary cartilaginous mass superiorly and a lobule-like tissue mass inferiorly (Fig. 45.3). Anotia can also occur and is generally associated with a low-lying hairline. Although unusual, stenosis or atresia of the external auditory canal may be found in the presence of a well-developed auricle (7).
Microtia occurs commonly as an isolated condition. However, specific syndromes have been associated with microtia and atresia. Treacher Collins syndrome, a result of a mutation in the gene TCOF1 (8), is associated with bilateral microtia, whereas unilateral microtia is more common in Goldenhar’s syndrome. Other syndromes less commonly associated with auricular dysmorphic features have been detailed by Konigsmark and Gorlin (9) and include the following: microtia, hypertelorism, cervical fistula and nodules, and mixed hearing loss; thickened earlobes and incudostapedial abnormalities; lacrimoauriculodentodigital syndrome; malformed low-set ears and conductive hearing loss; and lop ears, micrognathia, and deafness. An excellent monograph by Melnick and Myrianthopoulos (10) provides other listings of congenital conditions associated with malformations of the auricle. Trisomy 13-15, 18, and 22 have been reported with microtia as one of multiple anomalies (11, 12, 13). Antenatal detection of microtia by ultrasonography could alert physicians to other anomalies (14).
The incidence of microtia has been estimated to be 1 in 10,000 births according to the Center for Disease Control and Prevention data for metropolitan Atlanta (J. Cordero, personal communication). This rate includes syndromic forms of microtia. A higher incidence has been noted in other geographic populations (15, 16, 17, 18, 19, 20), as well as in infants born of diabetic mothers (21,22) and infants exposed to intrauterine varicella (23). The inheritance pattern theoretically can be calculated if microtia is part of a dominant or recessive pattern; however, even if familial, the inheritance pattern can vary (22,24, 25, 26, 27, 28). Twins do not necessarily both develop microtia, suggesting that the intrauterine environment is not solely responsible (29). Genetic animal models are being developed or exist in nature (30, 31, 32, 33). In isolated microtia, the genetic probability is not easily computed; however, there is quite possibly an increased incidence for subsequent siblings (24, 25, 26, 27, 28). I have seen microtia occur in four individuals of the same family.
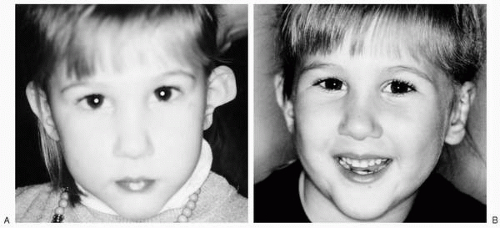 FIG. 45.1 Minor auricular malformation; the auricle is prominent with partial congenital absence of the lower helix, scapha, anthelix, conchal bowl, and lobule. A: Preoperative. B: Postoperative appearance. |
 FIG. 45.2 Despite severity of malformation, a meatus, canal, and tympanic membrane are present. |
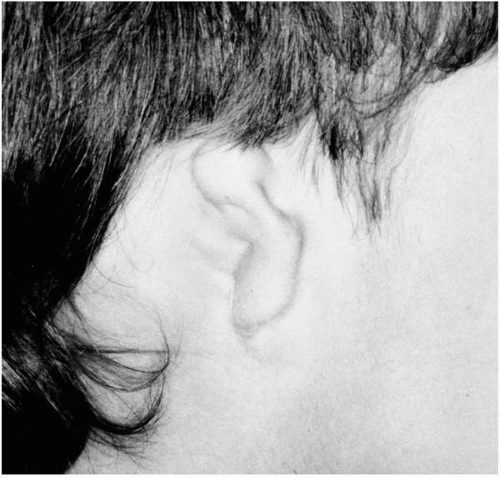 FIG. 45.3 Typical appearance of microtia. |
Animal models suggest possible embryologic mechanisms for microtia and atresia. Poswillo (34) has provided a mouse model to demonstrate a similar malformation caused by rupture of the stapedial artery during development. Unfortunately, no mechanism to confirm this hypothesis yet exists (34,35). As an alternative mechanism of abnormal development, the failure of neural crest migration has been implicated in the pathogenesis. This hypothesis has been circumstantially strengthened by the known teratogenic effect of maternal ingestion of vitamin A (36). The selectivity of vitamin A toxicity on the second branchial arch is hypothesized to be the reason that microtia due to vitamin A teratogenicity is characterized by a preserved tragus (Fig. 45.4). Animal models have shown that the second branchial arch in mice does not develop when migration of the neural crest is retarded by vitamin A (4). However, because in most cases of microtia the tragus is not preserved, this theory has not been widely applicable.
Intrauterine deformation (37) may also cause auricular malformation. As an example, from personal experience, in one patient the ipsilateral hand was deformed presumably
due to an abnormal intrauterine position in which the hand rested against the ear. Of clinical interest is the fact that this infant selected a peculiar posture for several weeks postpartum, holding the deformed hand against the deformed ear.
due to an abnormal intrauterine position in which the hand rested against the ear. Of clinical interest is the fact that this infant selected a peculiar posture for several weeks postpartum, holding the deformed hand against the deformed ear.
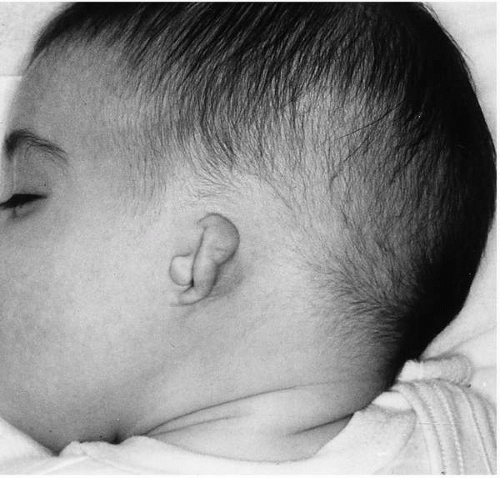 FIG. 45.4 Vitamin A teratogenicity. Note the presence of a tragus, which usually is absent in microtia. |
Classification systems have been devised to grade the degree of severity of auricular malformation; however, these subjective grading schemata of types I, II, and III or of mild, moderate, and severe malformation are of little practical use. Instead, individual analysis of the specific anatomic features is more important for decisions concerning reconstruction. Specific considerations from the physical examination follow.
The Presence of a Meatus and Canal
In cases of severe malformation, the meatus and canal are usually absent. However, their presence raises several issues. First, if the auricle is not severely malformed and if a canal exists, the potential for hearing preservation or reconstruction is enhanced (38). Second, the presence of a canal, especially if narrow, makes the patient susceptible to secondary cholesteatoma. Third, auricular reconstruction will need to accommodate to this fixed canal position yet be symmetrically located in relation to the contralateral ear. Fourth, for hearing habilitation in bilateral microtia, an air- rather than bone-conduction hearing aid may be preferred. Fifth, the otologic surgeon must not be tempted to reconstruct a canal stenosis until after the external ear has been repaired.
The Presence of a Tympanic Membrane
The presence of a tympanic membrane raises the possibility that hearing levels may be acceptable or a conductive loss more easily corrected. Additionally, the tympanic membrane allows otoscopic monitoring because the microtic ear is at risk for otitis media and extended complications (39).
The Hairless Zone Around the Auricle
Even with severe microtia, a hairless cutaneous rim persists in most cases. With anotia, on the other hand, the hairline can be extremely low. The significance of a hairless zone is apparent during the first stage of rib reconstruction because the superior portion of the cartilaginous framework of necessity will reside under hair-bearing skin. In the patient who has an adequate zone of hairless skin, fewer hair removal techniques, such as skin grafting or hair lasering, will be needed later.
The Cartilaginous Appendage
The cartilaginous appendage varies in appearance and orientation. Importantly, in less severe malformations, the superior cartilaginous portion of the auricle may have only a moderate deformity and may be reconstructed using less morbid techniques adapted from otoplasty (40). In severe microtia, the volume of cartilaginous remnant determines the degree of overlying soft tissue cover. If rib reconstruction is elected, skin coverage is critical. The greater the size of the cartilaginous remnant, the greater will be the amount of pliable soft tissue cover with which the surgeon can work. Another important point is whether the auricle remnant has a smooth covering or whether the skin convolutes to fit the contours of the auricular remnant. Should the convolutions be very deep and pitted, preservation of intact skin will be more difficult. Also, at times a rudimentary conchal bowl and tragus will exist. Auricular features that are well formed can be incorporated into the reconstruction. Conversely, an abnormally located conchal bowl and tragus may add to the challenge of removing the cartilaginous remnants during the reconstruction phase, because the location of the cartilaginous framework as it relates to the contralateral auricle is a priority in the repair of microtia.
Lobular Remnant
A lobular remnant is present in the typical case, even with severe malformation. During reconstruction, this tissue is rotated posteriorly and inferiorly to abut the costal framework at its inferior margin. The presence of lobular tissue provides for some flexibility in establishing the overall vertical height of the new auricle as it is normally transferred at a secondary stage and allows for accurate design at this point. Additionally, this lobule-like tissue hopefully will be adequate to place an earring, which some patients desire and which assists with eventual aesthetic appeal.
The Position of the Auricle
On lateral view, the microtic ear is smaller in vertical height than the contralateral, normal ear. The most cephalad portion of the normal ear lies approximately at the level of the
lateral brow, whereas the microtic ear is caudad to this level. Microtic ears also exhibit a more vertical axis of orientation than a normal auricle. In the normally oriented auricle, an imaginary line drawn from the most superior portion of the helix through the lobule is roughly parallel with the dorsum of nose. This relationship is very helpful in properly placing the cartilage framework during surgery. Another common finding is that in the frontal view, the lobule tends to be 3 to 5 mm higher on the microtic side than on the contralateral normal side and is coupled with a lack of tragal prominence.
lateral brow, whereas the microtic ear is caudad to this level. Microtic ears also exhibit a more vertical axis of orientation than a normal auricle. In the normally oriented auricle, an imaginary line drawn from the most superior portion of the helix through the lobule is roughly parallel with the dorsum of nose. This relationship is very helpful in properly placing the cartilage framework during surgery. Another common finding is that in the frontal view, the lobule tends to be 3 to 5 mm higher on the microtic side than on the contralateral normal side and is coupled with a lack of tragal prominence.
Skin Tags
Skin tags are often present. Their removal should be delayed until after placement of the reconstructed cartilaginous framework to avoid vascular compromise of the overlying skin. Occasionally, a skin tag can be used in the reconstructive effort.
The Mandible
Especially in Goldenhar’s syndrome (oculoauriculovertebral syndrome or hemifacial microsomia), the mandible may be smaller on the microtic side. This finding carries implications for the aesthetics of ear reconstruction because the mandible may be reconstructed at another time. Depending on the reconstruction technique, rib grafting may be used for mandibular augmentation, as well as for auricular repair. Should distraction osteogenesis be planned, the mandible will expand quickly and the position of the ear will appear to change rapidly. If mandibular reconstruction is not planned, the presence of an asymmetric mandible makes it necessary for the surgeon to rely upon aesthetic judgment rather than strict measurement in determining the proper location of the newly created auricle. I see patients in conjunction with an oral surgeon so that simultaneous ear and jaw reconstruction can be planned.
The Contralateral Ear
It is very important to evaluate the contralateral ear prior to the reconstruction. Good hearing is more likely in a normal-appearing ear; however, the hearing of both ears must be tested. Further, minor otologic anomalies are often present in the contralateral ear. In addition to these concerns, the normal contralateral ear serves as the model for reconstruction and associated otoplasty techniques are often necessary to enhance the overall symmetry of the repair.
EVALUATION AND CARE OF THE PATIENT PRIOR TO SURGERY
Infancy
Because auricular malformation is less common and less familiar than other congenital malformations such as cleft lip or club foot, the parents will require extensive counseling. Compounding the situation, the malformed auricle is a visible condition during the first several months or even years of life because of the lack of hair to camouflage the condition. After the initial concern about the auricular appearance, parental attention then focuses on hearing. A thorough brainstem evoked response audiometric test, not merely an auditory brainstem response (ABR) screening, should be performed as soon after birth as possible. During the first few weeks of life, brainstem evoked response audiometry can be performed under natural sleep conditions rather than under sedation. Even in cases with unilateral microtia, the hearing must be evaluated. Although the contralateral normal-appearing ear has normal hearing in most cases, this must be proven. The abnormal ear usually has a maximum conductive hearing loss of about 60 dB. However, a lesser conductive loss or associated sensorineural loss may be present (41).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


