Transtemporal and Transpetrous Approaches to the Cranial Base
Michael J. McKenna
Advances in surgical technology and technique, intraoperative cranial nerve monitoring, anesthesia, intraoperative stereotactic guidance systems, and stereotactic radiation therapy have made possible the successful management of skull base lesions that were once considered incurable or untreatable without unacceptable morbidity and mortality. During the past 30 years, the limits of resectability have been continuously redefined. These advances have given rise to an evolution of transtemporal approaches to intracranial and skull base lesions and a close collaboration between otologists and neurosurgeons. The acquisition of the necessary skills to successfully perform these procedures requires a thorough knowledge and appreciation of the three-dimensional anatomy of the temporal bone and skull base, hundreds of hours of practice in the dissection laboratory, and an extended period of mentorship and observation. To this end, there are no shortcuts.
Fundamental to the successful management of skull base tumors is the establishment of an accurate preoperative diagnosis, precise determination of the location and extension of the tumor and its proximity to critical anatomic structures, assessment of preoperative deficits, and a realistic estimation of the absolute, likely, and possible deficits associated with each surgical approach being considered. The hallmark of any good surgical approach is the achievement of adequate exposure necessary for safe and complete resection. For most transtemporal approaches, exposure is increased at the cost of function, including hearing and facial function, and the risk of potential neurologic deficits that occur with brain retraction and interruption of central venous flow. An understanding of the advantages and limitations of each approach and a thorough preoperative evaluation provide the basis for surgical planning. Ultimately, the choice of an appropriate surgical approach is determined in large part by the comfort and level of experience and expertise of both the otologic and neurologic surgeons.
PREOPERATIVE EVALUATION
The evaluation of patients who are being considered for surgical treatment of posterior fossa and skull base tumors begins with a thorough physical examination, including a complete neurologic examination, during which the function of each of the cranial nerves must be carefully assessed. Patients who are at risk for developing hearing loss should undergo complete audiometry, including both pure-tone and speech audiometry. Vestibular testing may be helpful in some cases, especially in assessing contralateral vestibular function in patients who are being considered for procedures that result in unilateral vestibular ablation.
Preoperative radiologic evaluation is an essential component of the preoperative assessment (Chapter 4). Both magnetic resonance imaging (MRI) and computed tomography (CT) provide valuable information. Magnetic resonance images are obtained with and without gadolinium contrast in the axial, coronal, and sagittal planes. Magnetic resonance imaging allows for the evaluation of the size, location, and degree of extension for most tumors. In addition, it provides valuable information that is most helpful in establishing an accurate preoperative differential diagnosis, often based on degree of enhancement; enhancement of associated structures, including the dura; signal intensity characteristics; and the location of critical vascular structures, which are seen as flow voids. The sagittal images are especially helpful in gaining an appreciation of the location of prepontine tumors with respect to the brainstem and basilar artery (1). CT scans are valuable in defining the bony anatomy of the temporal bone and skull base, including the degree of pneumatization, location of the venous sinuses, and bony destruction and invasion. These are often critical determinants of the amount of exposure that is achievable. Together, they provide the basis for assessment of the adequacy of exposure to be achieved by the specific approach or approaches under consideration. In
addition, preoperative angiography may be helpful in determining the vascularity and blood supply in appropriate cases. It may also be helpful in assessing the venous return and collateral flow through the venous sinuses, as well as the location of the vein of Labbé for procedures in which this structure may be at particular risk. Although some of this information may be obtainable from MRI, in cases where this information is absolutely critical in the decision-making process standard arterial angiography remains the gold standard. In situations where some consideration is given to possible sacrifice of the internal carotid artery, preoperative test occlusion and balloon occlusion may be necessary.
addition, preoperative angiography may be helpful in determining the vascularity and blood supply in appropriate cases. It may also be helpful in assessing the venous return and collateral flow through the venous sinuses, as well as the location of the vein of Labbé for procedures in which this structure may be at particular risk. Although some of this information may be obtainable from MRI, in cases where this information is absolutely critical in the decision-making process standard arterial angiography remains the gold standard. In situations where some consideration is given to possible sacrifice of the internal carotid artery, preoperative test occlusion and balloon occlusion may be necessary.
Preoperative review in a multidisciplinary setting with otologists, neurosurgeons, radiologists, and radiotherapists has proven helpful in establishing the most appropriate and advantageous approach. In this setting the geometry of each approach can be reviewed and questions or concerns of each subspecialist discussed. It is particularly helpful in patients who are likely to require postoperative radiation therapy, especially in determining what component of a specific tumor must be removed to provide a critical margin of safety and efficacy for postoperative radiation therapy.
The evolution, development, and modifications of transtemporal surgery were in large part driven by efforts to achieve improved exposure for the removal of posterior fossa tumors, which are not optimally exposed through the suboccipital approach. Although the suboccipital approach is highly versatile, provides a panoramic view of the cerebellopontine angle, and is relatively easy and rapid to perform, it does not allow for complete visualization and exposure of tumors that extend anteriorly into the prepontine space and petroclival junction (Figs. 12.1 and 12.2). Access to these tumors through the suboccipital approach is often blocked by the bridging of cranial nerves V to XI. Also, tumors that extend deep within the cerebellopontine angle and pontomedullary junction are obscured by the cerebellum, which must be either forcefully retracted or partially resected to provide adequate exposure. By approaching the posterior fossa through the temporal bone, a more anterior exposure can be accomplished and the depth of the cerebellopontine angle can be visualized without significant cerebellar retraction. These more lateral and direct approaches result in a shallower surgical field and allow for the use of shorter instruments and improved surgical precision. The degree of required exposure, and hence the size and location of the posterior fossa tumor, and individual variations in pneumatization and location of the venous sinuses determine the approach.
TRANSLABYRINTHINE APPROACH
Indications
The translabyrinthine approach provides exposure to the cerebellopontine angle and internal auditory canal. It has been used extensively for the removal of acoustic neuromas of all sizes when hearing preservation is not a goal. It is a highly versatile approach that has been used for a variety of lesions, including meningiomas and neuromas of the trigeminal and lower cranial nerves, as well as selective gliomas, chondrosarcomas and epidermoid tumors. It offers the distinct advantage over the suboccipital approach in obviating the need for cerebellar retraction (Figs. 12.3 and 12.4). In the past it has been highly criticized for providing inadequate exposure for the removal of large tumors. However, this criticism has been muted over the last two decades as it has gained wide acceptance in numerous centers throughout the world, with excellent results for tumors of all sizes, including even the largest acoustic neuromas. Its successful use for large tumors is absolutely dependent on a complete and thorough removal of bone over the posterior fossa and middle fossa dura and around the internal auditory canal. In cases with poor pneumatization, an extremely anteriorly located sigmoid sinus, or high jugular bulb, exposure may be difficult to accomplish and may be suboptimal for the removal of larger tumors. Under these circumstances, a retrosigmoid approach affords better and safer exposure. The location of the sigmoid sinus and jugular bulb can be assessed with an axial MRI scan. If the MRI scan raises questions regarding the adequacy of the exposure, a CT scan will provide definitive radiographic information. Even under optimal circumstances, the translabyrinthine approach does not provide adequate exposure of the inferior posterior fossa, the view of which is obstructed by the jugular bulb. The jugular bulb also obstructs the view of the neural compartment of the jugular foramen.
Surgical Technique
The translabyrinthine approach is accomplished with the patient in the supine position with the head turned. Some surgeons have advocated the use of a soft headrest so that the head position can be changed intraoperatively to facilitate exposure. Others choose a fixed positioning device, which allows for the use of attached intraoperative retractors. The operation begins with a curved incision approximately 4 cm posterior to the postauricular crease. Inferiorly, the incision is carried down to the bone. Superiorly, the incision is carried down to the level of the temporalis muscle, which is then incised down to bone along the temporal line. The soft tissues overlying the mastoid cortex are elevated with a large periosteal elevator to the posterior aspect of the external auditory canal. Once self-retaining retractors are placed, a large cutting bur and suction irrigation are used to remove the bone of the mastoid cortex. Bone overlying the sigmoid sinus is removed using a combination of both cutting and diamond burs. Some degree of retrosigmoid posterior fossa dural exposure is also necessary, although the degree is dependent on the location of the sinus and the degree of exposure necessary for the task at hand. Mastoid emissary veins are carefully isolated using fine diamond burs and then controlled with bipolar cautery. Avulsion of an emissary vein or inadvertent laceration of the sigmoid sinus is best controlled with extra luminal hemostatic packing such as Surgicel. A canal wall-up or canal wall-down (Chapter 11) mastoidectomy is performed with skeletonization without exposure of the descending segment of the facial nerve from the second genu to the stylomastoid foramen. Using diamond burs, bone is removed from the tegmental plate to expose the middle fossa dura, which can later be easily elevated to improve exposure. A labyrinthectomy is then performed and the vestibule entered. The ampulla of the superior semicircular canal is removed last and is an important landmark because it lies in close proximity to the upper tympanic and labyrinthine segments of the facial nerve. Extensive drilling beyond the superior ampulla puts the facial nerve at risk of injury. With completion of the labyrinthectomy, the bone is removed inferiorly to first expose and then skeletonize the jugular bulb. The bony removal is then continued medially to the level of the internal auditory canal. Once the internal auditory canal is identified, bone inferior to the canal and superior to the jugular bulb is removed anteriorly along the posterior fossa bony plate. It is important that bone be removed medial and inferior to the jugular bulb to provide necessary exposure to the anterior inferior aspect of the cerebellopontine angle. Among the most critical aspects of the surgical exposure through the translabyrinthine approach is complete and extensive bone removal around the internal auditory canal. The bone should be removed for approximately 280 degrees around the internal auditory canal and anteriorly along the posterior fossa plate both inferior and superior to the internal auditory canal for several millimeters. Bone is carefully removed from the sinodural angle over the superior petrosal sinus. When completed, there should be no bony restriction to movement of the sigmoid sinus, posterior fossa, and middle fossa dura, all of which should be easily compressible. The last bone to be removed is that which circumferentially surrounds the lateral aspect of the internal auditory canal. This is carefully accomplished until both the transverse and vertical crests are identified and the take-off of the labyrinthine segment of the facial nerve is clearly visualized. Incomplete bone removal at this point in the operation may compromise the early identification of the facial nerve within the fundus of the internal auditory canal. Before the dura is opened, it is essential that the bone removal be complete, because later attempts to remove additional bone with the dura open and the facial nerve exposed significantly increase the risk of neural injury and unnecessarily spills bone dust into the posterior fossa.
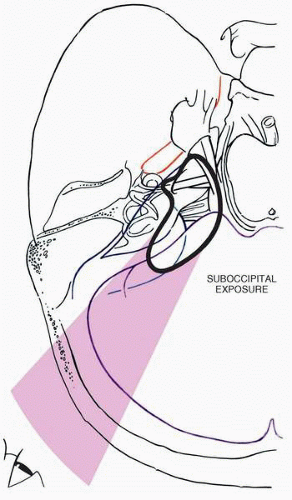 FIG. 12.1 The suboccipital approach is highly versatile and can be used for resection of both large and small tumors. Exposure of the prepontine space is limited by the angle of approach. The pontomedullary junction may be obscured by the cerebellum, requiring cerebellar resection or forceful retraction. Exposure of the entire internal auditory canal cannot be accomplished without transecting the posterior semicircular canal and sacrificing hearing. |
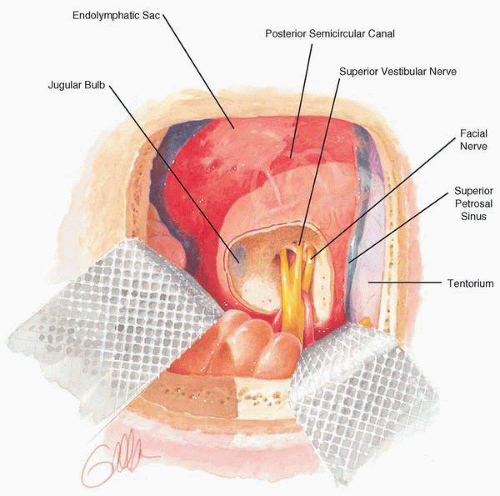 FIG. 12.2 Exposure of the posterior fossa and internal auditory canal by the retrosigmoid or suboccipital approach. A high jugular bulb may interfere with exposure of the entire internal auditory canal. |
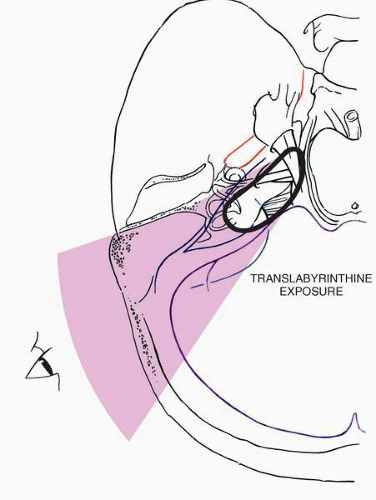 FIG. 12.3 The translabyrinthine approach can be used for tumors of all sizes. It provides excellent exposure of the pontomedullary junction. The lower cranial nerves (IX, X, and XI) may not be well visualized when obscured by a high jugular bulb. A small mastoid cavity may limit its utility for larger tumors. |
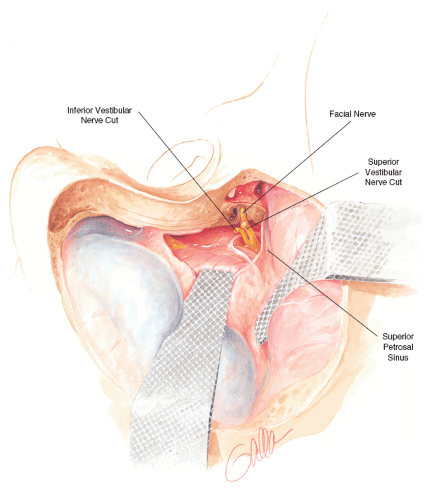 FIG. 12.4 Posterior fossa exposure by the translabyrinthine approach makes use of a presigmoid dural opening. With proper bone removal, it provides excellent exposure for safe removal of large tumors when lower cranial nerve involvement is not a concern. |
The dura over the internal auditory canal is open lengthwise and slightly inferior to the midline to be absolutely certain that the facial nerve is not inadvertently injured. Using a sharp hook or a sharp angled knife, the dura is transected at its bony junction at the fundus of the internal auditory canal. A second curved incision is made in the dura at the level of the porus acousticus and extended anteriorly to the limits of the bone removal. A final T-shaped dural incision is made that extends just anteriorly along the length of the sigmoid sinus with a limb, which extends between the sinus and the opening of the porus. Once reflected, additional exposure can be achieved as needed, depending on the size of the tumor and requirements for exposure.
In cases of large tumors the flow of cerebrospinal fluid (CSF) into the wound may be obstructed and the tumor may begin to protrude into the cavity. At this point, it is essential that CSF decompression be accomplished in order to achieve relaxation of the tumor and cerebellum into the posterior fossa. This can occur by elevating the inferior aspect of the cerebellum and exposing the arachnoid overlying the cisterna magna. The opening the arachnoid in this region with a sharp hook usually results in an immediate flow of CSF and relaxation of both the tumor and cerebellum.
The tumor dissection is begun in the fundus of the internal auditory canal with sharp transection of the superior vestibular nerve and exposure of the facial nerve. With the facial nerve clearly visualized, the tumor and remaining structures of the internal auditory canal are dissected from lateral to medial. The technique for tumor removal is similar to that for other approaches. The capsule of the tumor is incised, an extensive intracapsular debulking is accomplished, and eventually the neural and vascular structures of the posterior fossa are dissected from the capsule using a combination of blunt and sharp dissection with bipolar cautery when necessary. The use of a fenestrated suction irrigator with a constant flow of irrigation is very helpful in dispersing and removing blood and maintaining a clear visual field.
Once the tumor has been completely removed and hemostasis achieved, the craniotomy is obliterated with strips of abdominal fat, which are packed through the craniotomy in layers until eventually a mass of fat is dumbelling through the craniotomy into the posterior fossa. Although it is sometimes possible to narrow the dural defect by partial suture repair, it is rare that a watertight closure can be accomplished. Prevention of egress of spinal fluid is achieved predominantly through fat packing. Additionally, the aditus may be blocked with temporalis fascia or bone wax. Others have advocated opening the facial recess with removal of the incus and packing of the eustachian tube orifice with either fascia or hemostatic packing. Over the past several years, we have nearly eliminated the problem with postoperative CSF otorhinorrhea after translabyrinthine surgery by transection and closure of the external auditory canal with removal of the canal skin and eardrum, removal of the posterior bony canal wall, wide exposure of the eustachian tube orifice, and bone wax packing of eustachian tube as far anteriorly as can be safely accomplished. This maneuver, which requires an additional 30 to 45 minutes of work, has reduced the incidence of CSF leak following this approach from approximately 12% to less than 1%.
Advantages
The translabyrinthine approach offers two distinctive advantages over the retrosigmoid or suboccipital approach. The first advantage is a reduced requirement for cerebellar retraction,
especially in cases of larger tumors. However, with a well-performed suboccipital/retrosigmoid craniotomy in which the anterior margin of the craniotomy abuts the posterior aspect of the sigmoid sinus, it is possible to minimize the amount of cerebellar retraction necessary. It is not uncommon for patients to experience some transient postoperative cerebellar dysfunction, especially in the first few weeks following suboccipital surgery. Although this may delay recovery in the immediate postoperative phase, the majority of patients have normal cerebellar function at 1 month following surgery. It is interesting that many of these patients with normal cerebellar function do have evidence of cerebellar encephalomalasia on follow-up MRI scans. It is unclear what effect, if any, this has on long-term cerebellar function as these patients grow older.
especially in cases of larger tumors. However, with a well-performed suboccipital/retrosigmoid craniotomy in which the anterior margin of the craniotomy abuts the posterior aspect of the sigmoid sinus, it is possible to minimize the amount of cerebellar retraction necessary. It is not uncommon for patients to experience some transient postoperative cerebellar dysfunction, especially in the first few weeks following suboccipital surgery. Although this may delay recovery in the immediate postoperative phase, the majority of patients have normal cerebellar function at 1 month following surgery. It is interesting that many of these patients with normal cerebellar function do have evidence of cerebellar encephalomalasia on follow-up MRI scans. It is unclear what effect, if any, this has on long-term cerebellar function as these patients grow older.
The second distinct advantage of the translabyrinthine approach over the suboccipital approach is a significantly reduced incidence of postoperative headache. Although headache can occur following the translabyrinthine approach, the incidence and the occurrence of severe, incapacitating postoperative headache is significantly less than that which occurs with the suboccipital or retrosigmoid approach (2). Several factors have been identified that may contribute to the development of the headache, including injury to the suboccipital musculature and the dispersion of bone dust into the subarachnoid space, which occurs with drilling of the internal auditory canal (3). Over the past several years there have been multiple reports on technical modifications (4,5) to minimize postoperative headache, including modifications of the suboccipital incision, cranioplasty, and packing of the posterior fossa with Gelfoam prior to drilling in an effort to contain bone dust that is liberated from drilling of the internal auditory canal. Although it seems that each of these has resulted in a modest improvement in the postoperative headache problem, it has not been eliminated entirely, and it remains a disabling problem in approximately 5% of patients.
With our modification of the translabyrinthine approach with the canal wall-down obliteration of the eustachian tube and transection and closure of the external auditory canal, the problem of postoperative CSF leak has been nearly eliminated, making this a significant advantage over the retrosigmoid approach, where postoperative spinal fluid leakage still occurs in approximately 10% to 15% of cases. Even in the standard translabyrinthine approach with a canal wall-up technique, the incidence of CSF leakage seems to be less than in the suboccipital approach, which may possibly be attributable to the ability to block the egress of spinal fluid through the attic and at the eustachian tube orifice.
Another potential advantage of the translabyrinthine approach over the retrosigmoid approach is in the event of injury to the facial nerve, which requires repair or grafting. Under these circumstances the labyrinthine and tympanic segments can be mobilized and a proximal stump of the facial nerve made more easily available for anastomosis with a cable graft. It is also possible to mobilize the facial nerve from the stylomastoid foramen to labyrinthine segment, providing 10 to 15 mm of length and thus obviating the need for a cable graft, making possible a primary repair with a single anastomosis (Chapter 36).
Advocates of the translabyrinthine approach have often described an improved ability to identify and dissect the facial nerve beginning at the meatal foramen when it is not possible through the retrosigmoid approach. Our experience with the suboccipital and retrosigmoid approach has proven this not to be a significant issue as long as the internal auditory canal is opened completely, under which circumstances the anatomic relationships of the fundus of the canal are quite similar between the two approaches.
Disadvantages
The primary disadvantage of the translabyrinthine approach over the suboccipital approach is limitation of exposure, especially in the inferior aspects of the posterior fossa. Although this is not a significant problem with acoustic neuromas, which are usually not adherent to the lower cranial nerves and can be delivered from the inferior depths of the posterior fossa, it makes the translabyrinthine approach inadequate or dangerous for other more adherent or invasive tumors, such as meningiomas. Because the inferior aspect of the cerebellopontine angle is not directly visualized, bleeding in this area can be difficult to control and represents a significant potential problem. Occasionally, bleeding can occur from the stump of the petrosal vein, which may be avulsed when it becomes adherent to the superior pole of the tumor capsule and the capsule is delivered from the superior aspect of the cerebellopontine angle. This bleeding, which may be profuse, can be significantly reduced by ligating the superior petrosal sinus.
Another disadvantage of the translabyrinthine approach is the obvious requirement to sacrifice hearing in the operated ear. For large acoustic neuromas, this is not a significant issue, because hearing is not usually preserved with any approach once the size of the tumor exceeds 2.5 cm (6). However, for other lesions, such as meningiomas and epidermoids, this may prove to be a relative disadvantage over the retrosigmoid approach. Unilateral hearing loss is weighted against other potential deficits, which can be avoided by the improved exposure offered by the translabyrinthine approach.
RETROLABYRINTHINE APPROACH
Indications
The retrolabyrinthine approach is a presigmoid approach accomplished by performing a canal wall-up mastoidectomy with skeletonization of the descending segment of the facial nerve, semicircular canals, and jugular bulb. It allows for a relatively small (keyhole) craniotomy, which is well suited for vestibular neurectomy, microvascular decompression, and biopsy procedures (Figs. 12.5 and 12.6). It is generally inadequate for tumor resection because of the limited exposure achieved. Because the otic capsule is not violated in this approach, the limits of exposure are confined to the region of the root entry zone and proximal course of the fifth, seventh, and eighth cranial nerves. The eighth nerve complex cannot be visualized at the porus acusticus, and the internal auditory canal cannot be accessed through this approach.
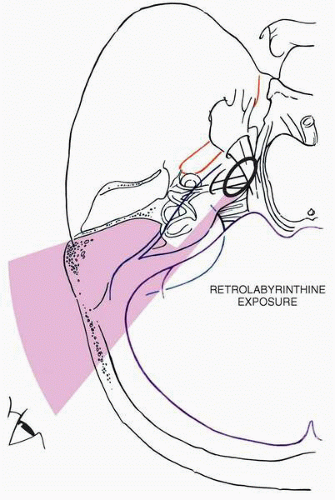 FIG. 12.5 The retrolabyrinthine approach provides limited access to the posterior fossa. Although this may be sufficient for selective vestibular neurectomy, some cases of microvascular decompression, and tumor biopsy, it is inadequate for resection of most tumors. Note: the surgeon’s view of the eighth nerve complex is proximal to the porus acusticus and the anatomic separation of the vestibular and cochlear nerves. |
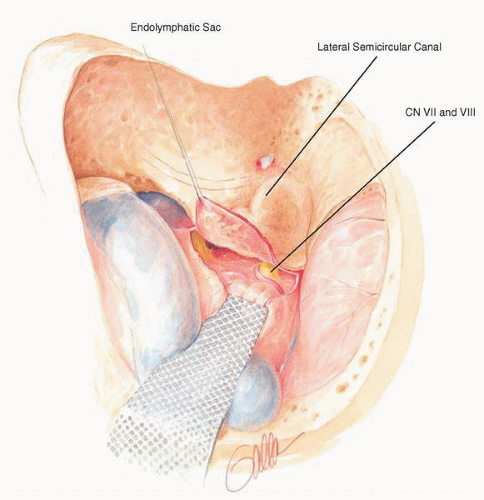 FIG. 12.6 In the retrolabyrinthine approach, the presigmoid dural opening is limited anteriorly by the posterior semicircular canal. Although well suited for selective vestibular neurectomy, the limited posterior fossa exposure makes it inadequate for resection of most tumors. CN, cranial nerves. |
Although the retrolabyrinthine approach has been used in the past for microvascular decompression in cases of trigeminal neuralgia, its predominant use at present is for selective vestibular neurectomy in patients with Meniere’s disease or other peripheral vestibulopathies. Although it has been used extensively for this indication, we have abandoned it for this use because of the difficulty in being able to clearly identify or separate the vestibular nerve fibers from the auditory nerve fibers in the part of the eighth nerve complex that is proximal to the porus acusticus. Even at the porus acusticus, which cannot be visualized through the retrolabyrinthine approach, the cleavage plane between the vestibular fibers and auditory fibers is not always clear.
Surgical Technique
The retrolabyrinthine craniotomy is performed with the patient in the supine position with the head turned. A curved incision is made in the postauricular area, approximately 3 to 4 cm posterior to the postauricular crease. As with the translabyrinthine approach, the incision inferiorly is carried down to the bone. Superiorly, the incision is carried down to the temporalis muscle, which is incised at the level of the temporal line. Soft tissues over the mastoid cortex are elevated to the level of the posterior aspect of the external canal. Self-retaining retractors are placed, and a canal wall-up mastoidectomy is performed. The sigmoid sinus is skeletonized, as is 1 to 2 cm of posterior fossa dura posterior to the sigmoid sinus. The descending segment of the facial nerve is skeletonized, with the bone left intact. The dome of the jugular bulb is identified, and bone is removed up to the jugular bulb. Superiorly the posterior semicircular canal is skeletonized. Bone is removed from the posterior fossa dura anterior and posterior to the sigmoid sinus from the jugular bulb inferiorly to the superior petrosal sinus superiorly. The sigmoid sinus is retracted posteriorly, and a curved incision is made in the presigmoid dura from the region of the jugular bulb up to the superior petrosal sinus. This dural flap should contain the endolymphatic sac, and efforts should be made not to transect the endolymphatic sac in the incision. Complete exposure of the root entry zones of the seventh and eighth nerves may require gentle retraction of the cerebellum posteriorly.
Upon completion of the intended surgical procedure, the craniotomy defect is packed with fat similar to that which is done for the translabyrinthine approach. In some cases it may be possible to achieve a watertight closure of the durotomy, although this is often technically difficult to accomplish.
Advantages
The retrolabyrinthine approach, which is now used predominantly for selective vestibular neurectomy, offers an advantage over the retrosigmoid or suboccipital approach in that patients have a significantly lower incidence of postoperative headache. When the retrolabyrinthine approach is done for selective vestibular neurectomy in Meniere’s disease, a simultaneous endolymphatic sac decompression can be accomplished with some potential for additional benefit.
Disadvantages
The primary disadvantage of the retrolabyrinthine approach is its inadequate exposure of the posterior fossa. In our experience, this even applies to selective vestibular neurectomy. Only the proximal two thirds of the eighth nerve complex can be well visualized through the retrolabyrinthine approach. The most distal segment of the eighth nerve complex that can be visualized through the retrolabyrinthine approach does not have a clearly demarcated separation between auditory and vestibular fibers, making it impossible to be absolutely certain that a complete selective vestibular neurectomy has been accomplished. This problem is evidenced in our own analysis and comparison of patients who underwent selective neurectomy through the retrolabyrinthine approach and a retrosigmoid approach with opening of the internal auditory canal (7). The incidence of recurrent postoperative vertigo and presence of a postoperative ice water caloric response was higher in patients who underwent the retrolabyrinthine approach.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


