Cystic Lesions of the Petrous Apex
Richard R. Gacek
Mark R. Gacek
The subtle clinical presentations of petrous apex lesions are related to the regional anatomy of the apical segment of the temporal bone (Fig. 44.1). The usual presenting symptoms of an expanding lesion in the petrous apex are a conductive hearing loss from the serous effusion caused by eustachian tube obstruction, headache from pressure on the dural covering, diplopia related to involvement of the third and sixth cranial nerves, facial hypesthesia caused by compression of the fifth cranial nerve, and varying degrees of faintness or vertigo probably caused by changes in vascular flow (1). Various pathologies may arise within this small region of the temporal bone because of the complex anatomic composition of the petrous apex, consisting of air cells, bone marrow, cartilage, nerve bundles, and vascular structures (internal carotid artery, jugular bulb) (2). Sophisticated imaging techniques (e.g., computed tomography [CT], magnetic resonance imaging [MRI]) now permit early recognition of a petrous apex lesion. The pathologies involving the petrous apex may be divided into solid and cystic lesions (Table 44.1).
DIAGNOSIS
The clinical suspicion of a progressive lesion in the petrous apex is based on recognition of one or more of the signs and symptoms related to adjacent anatomic structures (eustachian tube, cranial nerves III through VIII, dura, and internal carotid artery). In the premodern imaging era (before CT and MRI), lesions in this area were probably underrecognized because of the difficulty in clearly demonstrating bone erosion with the conventional base of skull radiographs or polytomography. Extensive bone erosion could be detected with such studies, followed by confirmation of an extradural mass by supplementary studies such as arteriography and pneumoencephalography. Presently, thin-section (1 to 1.5 mm) CT scanning and MRI are capable of identifying such lesions in the petrous apex much earlier in their development with minimal risk (Fig. 44.2). The evaluation of a suspected lesion in the petrous apex should require CT scanning and MRI (3,4). The nature of a lesion as solid or cystic is usually revealed by the enhancement on CT and signal picture on T1 and T2 images with MRI. Arteriography may be added to define a vascular lesion or to locate displacement of the internal carotid artery.
MANAGEMENT
Solid Tumors
The management of solid tumors requires identification of the histopathology prior to definitive treatment (1). Several factors determine the approach to biopsy of solid petrous apex lesions. If the tumor has extended into an area that is easily accessible without risk to labyrinthine function, such as the infralabyrinthine and hypotympanic cell tracts, or into the sphenoid sinus, these compartments should be accessed for sampling the tumor. However, if the tumor is contained
within the petrous apex and labyrinth function is normal, a middle cranial fossa extradural approach skirting the temporal bone is the most direct approach to the tumor while preserving seventh and eighth cranial nerve function.
within the petrous apex and labyrinth function is normal, a middle cranial fossa extradural approach skirting the temporal bone is the most direct approach to the tumor while preserving seventh and eighth cranial nerve function.
TABLE 44.1 Petrous apex pathologies categorized by lesion type | ||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||
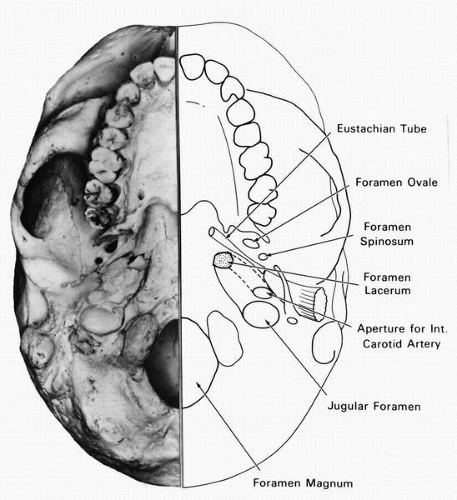 FIG. 44.1 Composite drawing and photograph showing base of skull structures adjacent to the petrous apex that influence clinical presentation. |
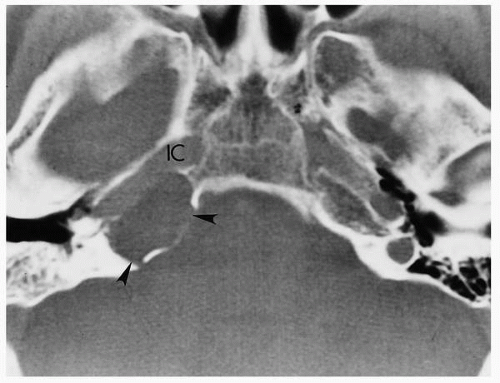 FIG. 44.2 Bone erosion from a petrous apex epidermoid (arrowheads) as seen in a CT scan. IC, internal carotid artery. |
Definitive management is guided by the histologic nature of the lesion. A benign lesion may be excised totally or subtotally depending on the progressive nature of the clinical symptoms and the patient’s age and medical status. Postoperative surveillance of the petrous apex tumor may be carried out with imaging studies to determine possible recurrence and progression. A malignant tumor will require nonsurgical management (radiation therapy, chemotherapy) because en bloc resection of this portion of the temporal bone is not feasible for cure, particularly if one considers the morbidity associated with the surgery. However, low-grade malignancy such as eosinophilic granuloma may be treated more effectively by extensive subtotal removal using curettage followed by radiation therapy.
Cystic Lesions
Cystic lesions may be vascular or nonvascular, and their management will vary from case to case. If imaging studies are not able to demonstrate the vascular nature of a lesion with certainty, then arteriography is required. The major vascular lesion of the petrous apex is an internal carotid aneurysm (Fig. 44.3). If the lesion is causing minimal nonprogressive clinical symptoms, then the aneurysm should be conservatively followed clinically and neuroradiologically. If the aneurysm becomes progressive and is responsible for significant neurologic symptoms, a team approach (neurosurgery and otolaryngology) to management of the aneurysm is necessary. Progressive preoperative occlusion followed by resection is one method of management if the patient tolerates the occlusive maneuver.
Occasionally, imaging studies are misleading. We have seen two patients presenting with episodic vertigo that revealed on T2 MRI a high-signal-intensity mass resembling a
cholesterol cyst in the petrous apex (Fig. 44.4). CT scan did not reveal bone erosion, but a compartment in the petrous apex was present (Fig. 44.5). It has been suggested that this may represent bone marrow. However, exploration of the petrous apex in these cases with severe sensorineural hearing loss in the involved ear revealed a thin-walled space with brisk venous bleeding requiring firm packing to control (Fig. 44.6). It is possible that these lesions represent venous anomalies (venous lakes). The sigmoid sinus and the jugular bulb were anatomically separated from this vascular compartment. The importance of this entity is that if it is properly recognized with the positive MRI but with no evidence of bone erosion on CT scanning, surgical exploration should be withheld and the patients only followed with clinical and radiologic methods to detect the possibility of a progressive lesion. Documentation of progression justifies surgical exploration.
cholesterol cyst in the petrous apex (Fig. 44.4). CT scan did not reveal bone erosion, but a compartment in the petrous apex was present (Fig. 44.5). It has been suggested that this may represent bone marrow. However, exploration of the petrous apex in these cases with severe sensorineural hearing loss in the involved ear revealed a thin-walled space with brisk venous bleeding requiring firm packing to control (Fig. 44.6). It is possible that these lesions represent venous anomalies (venous lakes). The sigmoid sinus and the jugular bulb were anatomically separated from this vascular compartment. The importance of this entity is that if it is properly recognized with the positive MRI but with no evidence of bone erosion on CT scanning, surgical exploration should be withheld and the patients only followed with clinical and radiologic methods to detect the possibility of a progressive lesion. Documentation of progression justifies surgical exploration.
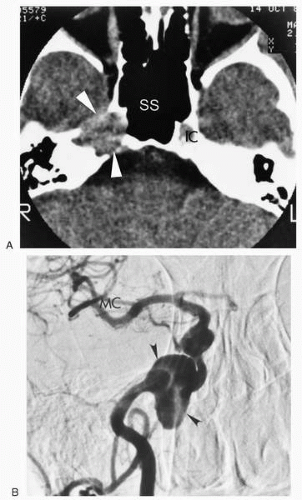 FIG. 44.3 A: CT scan of a 60-year-old woman with occasional episodes of vertigo (several hours’ duration) over a 10-year period demonstrates an erosive lesion (arrowheads) in the petrous apex. There was a normal auditory, vestibular, and neurologic examination. The bony ridge on the posterior wall of sphenoid sinus serves as a landmark for internal carotid artery (IC). SS, sphenoid sinus. B: Arteriogram in the same patient shows the internal carotid artery aneurysm (arrowheads). Neurosurgical consultation advised observation because of the lack of neurological deficits. MC, middle cerebral artery. |
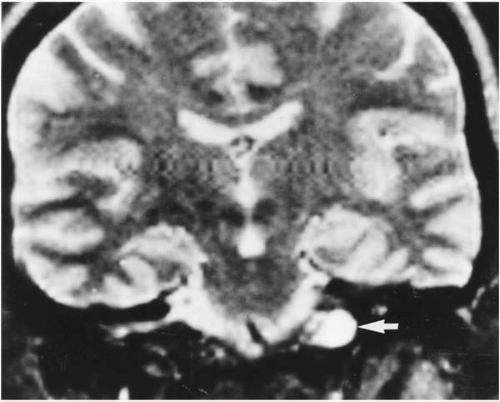 FIG. 44.4 MRI scan of a 56-year-old woman with episodic vertigo and dysequilibrium but without headache or other neurologic symptoms for 6 months. Her neurologic examination and auditory-vestibular assessment was normal. Arrow points to a high-signal collection in the petrous apex. |
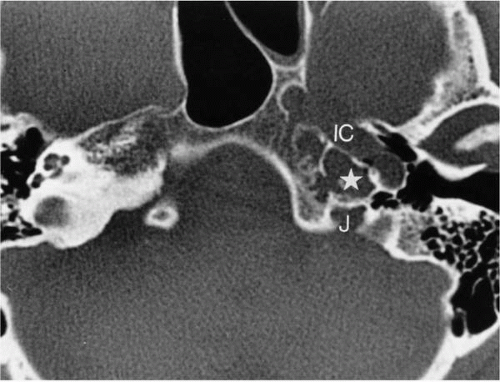 FIG. 44.5 CT scan on same patient in Fig. 44.6 shows a thin-walled compartment (star) medial to the internal carotid artery (IC) in the petrous apex but separate from the jugular bulb (J). |
Nonvascular Cystic Lesions
Petrositis
In the preantibiotic era, the most common cystic lesion of the petrous apex was infection, either chronic or acute, as a result of extension of the inflammatory process from the
middle ear and mastoid compartments. Progression of an epidural abscess in the air cell system of the petrous apex resulting in bone destruction with dural irritation and involvement of the cranial nerves adjacent to the petrous apex represents Gradenigo’s syndrome (Fig. 44.7). The advent of antibiotics and thorough mastoid surgery have virtually eliminated this complication of suppurative otitis media. Nevertheless, this complication does occasionally occur and presents a similar constellation of cranial nerve deficits and symptoms (pain) associated with signs of infection. Surgical exenteration and drainage of the epidural petrous apex abscess cavity is urgently indicated (5,6). Wide-field mastoid and middle ear exploration with identification of the cell tract leading to the apex is necessary to correctly locate and manage the abscess cavity (Fig. 44.8). Most commonly this tract will be located in the infralabyrinthine or perilabyrinthine cell groups (posteromedial, posterosuperior). The extent of bone removal required to expose the cavity
will depend on the presence or absence of function in the involved ear. If labyrinthine function is normal, exenteration of the diseased air cells should be performed with preservation of the otic capsule. Insertion of a drainage tube for the instillation of antibiotics into the abscess cavity is recommended for complete treatment of the infected cavity. Resolution of the inflammatory process results in obliteration of the defect with fibrous and osseous tissue. If labyrinthine function is significantly depressed, a transcochlear translabyrinthine approach to the petrous apex abscess is chosen (1,7).
middle ear and mastoid compartments. Progression of an epidural abscess in the air cell system of the petrous apex resulting in bone destruction with dural irritation and involvement of the cranial nerves adjacent to the petrous apex represents Gradenigo’s syndrome (Fig. 44.7). The advent of antibiotics and thorough mastoid surgery have virtually eliminated this complication of suppurative otitis media. Nevertheless, this complication does occasionally occur and presents a similar constellation of cranial nerve deficits and symptoms (pain) associated with signs of infection. Surgical exenteration and drainage of the epidural petrous apex abscess cavity is urgently indicated (5,6). Wide-field mastoid and middle ear exploration with identification of the cell tract leading to the apex is necessary to correctly locate and manage the abscess cavity (Fig. 44.8). Most commonly this tract will be located in the infralabyrinthine or perilabyrinthine cell groups (posteromedial, posterosuperior). The extent of bone removal required to expose the cavity
will depend on the presence or absence of function in the involved ear. If labyrinthine function is normal, exenteration of the diseased air cells should be performed with preservation of the otic capsule. Insertion of a drainage tube for the instillation of antibiotics into the abscess cavity is recommended for complete treatment of the infected cavity. Resolution of the inflammatory process results in obliteration of the defect with fibrous and osseous tissue. If labyrinthine function is significantly depressed, a transcochlear translabyrinthine approach to the petrous apex abscess is chosen (1,7).
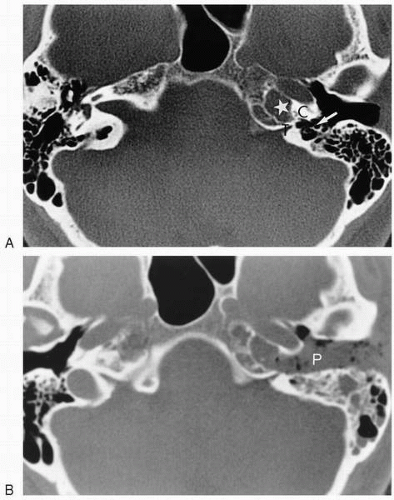 FIG. 44.6 Same patient as Fig. 44.5. A: The petrous apex compartment (star) was adjacent to the tympanomeningeal fissure (T) and the otic capsule (C). The arrow shows the infralabyrinthine cell tract. B: The compartment was exposed by a transcochlear approach and required firm packing (P) to control brisk venous hemorrhage. |
 FIG. 44.7 Photomicrograph of a petrous apex abscess cavity (PA). If the cavity cannot be reached via an existing air cell tract, the transcochlear approach is direct and offers adequate fistulization of the abscess. E, eustachian tube; C, cochlea; IC, internal carotid artery; IAC, internal auditory canal.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|