Purpose
To evaluate the 1-year efficacy and safety of photodynamic therapy (PDT) combined with intravitreal injections of ranibizumab for polypoidal choroidal vasculopathy (PCV).
Design
Retrospective chart review.
Methods
We retrospectively reviewed the medical records of 63 consecutive patients (66 eyes) with subfoveal PCV who were treated with PDT combined with intravitreal injections of ranibizumab. Of the 66 eyes, 29 had no history of treatment for PCV, 10 had been treated previously with only intravitreal injections of anti–vascular endothelial growth factor agents, and 27 had been treated previously with PDT. All eyes had a minimal follow-up of 12 months.
Results
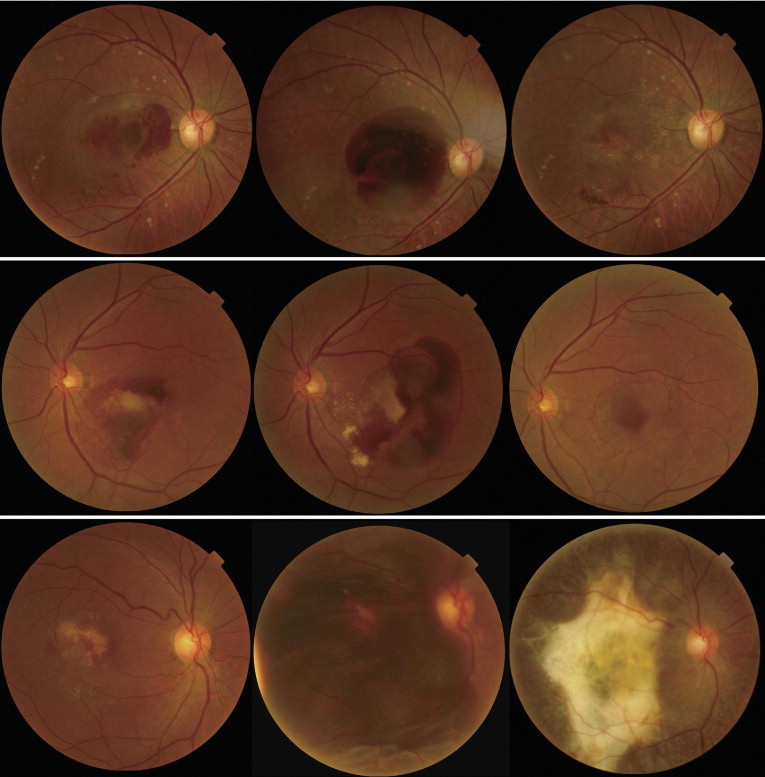
The combined therapy reduced substantially the exudative change immediately after initiation of treatment. In treatment-naïve eyes, mean VA before treatment (0.47 ± 0.37 logarithm of the minimal angle of resolution [logMAR]) improved to 0.32 ± 0.30 ( P < .01) at 3 months and to 0.29 ± 0.29 (P < .01) at 12 months. Polypoidal lesions were reduced in all eyes and disappeared completely in 79.1% of cases. In eyes treated previously with only anti–vascular endothelial growth factor therapy, some visual improvement was achieved, but in eyes treated previously with PDT, mean visual acuity (0.61 ± 0.45) deteriorated to 0.68 ± 0.52 at 12 months. Of all 66 eyes, 5 showed extensive postoperative subretinal hemorrhage, in 2 of which a vitreous hemorrhage developed, necessitating pars plana vitrectomy.
Conclusions
PDT combined with ranibizumab led to significant visual recovery in treatment-naïve eyes with PCV, but not in eyes with PCV that had demonstrated recurrence after previous PDT. PDT in combination with ranibizumab still has a risk of the postoperative hemorrhagic complications.
Today, intravitreal injections of anti–vascular endothelial growth factor (VEGF) agents are a standard treatment for exudative age-related macular degeneration (AMD). As a unique form of choroidal neovascularization (CNV), polypoidal choroidal vasculopathy (PCV) is characterized by a branching vascular network that terminates in polypoidal lesions. Similar to AMD, recent findings of high concentrations of VEGF in aqueous humor and high expression of VEGF in histologic specimens of PCV have suggested that VFGF is involved also in the pathogenesis of PCV. In contrast to AMD, however, it has been reported that the treatment effects of anti-VEGF agents on the vascular lesions associated with PCV are limited. In a recent report of PCV by Hikichi and associates, although exudative changes regressed with 3 monthly injections of ranibizumab, with concomitant improvement of visual acuity (VA), complete disappearance of the polypoidal lesions was achieved in only 26% of eyes.
A number of studies have shown encouraging results of photodynamic therapy (PDT) on PCV. In a report by Chan and associates, PDT led to complete regression of the polypoidal lesion in 95% of eyes with PCV and resulted in stable or improved VA 1 year after treatment. Unfortunately, 1 or more years after successful treatment with PDT, some eyes have a recurrence of the PCV lesions and, consequently, a decrease in VA. Akaza and associates reported that 64% of eyes with PCV that had been treated successfully with PDT showed a recurrence of the polypoidal lesions during a follow-up of 24 months. These recurrent polypoidal lesions often are accompanied by an exudative change, which results in a poor visual prognosis despite retreatment using PDT.
Several investigators have reported promising short-term results of PDT combined with bevacizumab for the treatment of PCV. Recently, Ruamviboonsuk and associates reported 1-year results of 12 eyes with PCV that were treated with PDT combined with ranibizumab. To date, however, the efficacy and safety of this combined therapy has not been evaluated sufficiently. In addition, most reports have involved PCV that had no previous treatments. In the clinical setting, physicians often need to treat eyes in which PCV has recurred after initial treatment with PDT or eyes with chronic PCV that is refractory to anti-VEGF agents, but, again, little information is available on the efficacy of combined therapy in such cases. Accordingly, the study described herein was designed to study the safety and efficacy of PDT combined with ranibizumab for the treatment of symptomatic PCV, depending on the history of previous treatment(s).
Methods
For this case series, we studied retrospectively the medical records of 66 consecutive eyes (63 patients) with subfoveal PCV that were treated with PDT combined with intravitreal injections of ranibizumab (Lucentis; Novartis, Bülach, Switzerland) at Kyoto University Hospital between the beginning of May 2009 and the end of February 2011. Inclusion criteria of the study were (1) symptomatic subfoveal PCV, (2) presence of exudative or hemorrhagic features involving the macula, (3) VA of 0.7 or less on a Landolt chart before treatment, and (4) a minimum follow-up of 12 months after the initial treatment. The diagnosis of PCV was based on indocyanine green angiography, which shows a branching vascular network that terminates in polypoidal swelling. In the current study, all eyes showed polypoidal lesions, a branching vascular network, or type 2 CNV beneath the foveal center. Eyes with other macular abnormalities (i.e., AMD, pathologic myopia, idiopathic CNV, presumed ocular histoplasmosis, angioid streaks, and other secondary CNV) were excluded from the study. However, pseudophakic eyes were included, but eyes with a history of vitrectomy were excluded.
At the initial visit, each patient underwent a comprehensive ophthalmologic examination, including measurement of best-corrected VA with a Landolt chart, determination of intraocular pressure, indirect ophthalmoscopy, slit-lamp biomicroscopy with a contact lens, spectral-domain optical coherence tomography ([OCT], Spectralis HRA+OCT; Heidelberg Engineering, Heidelberg, Germany), and fluorescein and indocyanine green angiography (HRA-2; Heidelberg Engineering). Patients who had a visual disturbance resulting from PCV were offered PDT combined with an intravitreal injection of 0.5 mg ranibizumab. Injections of ranibizumab were performed in a sterile manner and prophylactic topical antibiotics were applied for 1 week after the injection. At 3 to 4 days after the intravitreal injection of ranibizumab, normal-fluence PDT was performed using a 689-nm diode laser unit (Visulas PDT system 690S; Carl Zeiss, Dublin, California, USA) after an injection of verteporfin (Visudyne; Novartis), according to PDT guidelines for AMD. The greatest linear dimension chosen was based on fluorescein and indocyanine green angiograms, as previously described. All polypoidal lesions and the entire branching vascular network detected with indocyanine green angiography and type 2 CNV detected with fluorescein angiography were included. Serous pigment epithelial detachment was not included in the lesion area when the absence of underlying CNV was confirmed.
After the initial treatment, each patient was scheduled for an examination at 3 months, at which time they again underwent a comprehensive ophthalmologic examination. When indocyanine green angiography showed recurrent or residual polypoidal lesions and when an exudative change was seen on OCT, additional combination therapy was given. When residual polypoidal lesions were detected on indocyanine green angiography, but no exudative change was seen on OCT, no additional treatment was given and the patient was re-evaluated at the next visit. When only recurrent or residual exudative changes resulting from PCV were seen by OCT examination, but neither polypoidal lesions nor type 2 CNV were seen on angiography, an additional injection of ranibizumab was administered. After the additional injection of ranibizumab, the patient was scheduled to visit our clinic after 1 month, at which time they again underwent a comprehensive ophthalmologic examination.
In the current study, we examined 66 eyes with subfoveal PCV that were treated with PDT combined with intravitreal injections of ranibizumab. Of these 66 eyes, 29 had no history of treatment for PCV (treatment-naïve group). Ten eyes had been treated previously with only intravitreal injections of anti-VEGF agents, including ranibizumab, pegaptanib (Macugen; Pfizer, New York, New York, USA), or bevacizumab (Avastin; Genentech, South San Francisco, California, USA); these eyes had no history of PDT treatment (anti-VEGF group). Twenty-seven eyes had been treated previously with PDT for PCV (PDT group). Of the 27 eyes in the PDT group, 18 also had been treated previously with intravitreal injections of anti-VEGF agents.
All values are presented as mean ± standard deviation. For statistical analysis, best-corrected VA as measured with a Landolt chart was converted to a logarithm of the minimal angle of resolution (logMAR). VA was considered to be improved or deteriorated when the logMAR change was more than 0.3. On OCT sections, foveal thickness was defined as the distance between the inner surface of the neurosensory retina and the retinal pigment epithelium beneath the fovea. In each group, VA or foveal thickness after the combined therapy was analyzed by 1-way repeated-measures analysis of variance with the Dunnett method. At each time point, the change in VA or in foveal thickness was analyzed using the least-significant difference procedure. Software (StatMate III; ATMS, Tokyo, Japan) was used for the statistical analyses. A P value < .05 was considered to be statistically significant.
Results
In the study described herein, 66 eyes of 63 patients (44 men and 19 women), ranging in age from 57 to 85 years (mean ± standard deviation, 72.1 ± 8.0 years), underwent PDT combined with intravitreal injections of ranibizumab for the treatment of PCV. All patients were Japanese, and all were of Asian ancestry. Of these 66 eyes, 29 had no history of treatment for PCV (treatment-naïve group). Ten eyes previously had been treated only with intravitreal injections of anti-VEGF agents (anti-VEGF group); the mean number of previous anti-VEGF treatment was 4.30 ± 2.83 (range, 1 to 9). Twenty-seven eyes had been treated previously for the PCV with PDT (PDT group); the mean number of previous PDT and anti-VEGF treatments was 1.63 ± 0.74 (range, 1 to 3) and 1.67 ± 1.03 (range, 0 to 4), respectively. In the study period over 12 months, the mean number of combined treatments was 1.38 ± 0.63 (range, 1 to 4) ( Table 1 ) .
| Total | Treatment-Naïve Group | Anti-VEGF Group | PDT Group | |
|---|---|---|---|---|
| No. of eyes | 66 | 29 | 10 | 27 |
| Age (years) | 72.1 ± 8.0 | 70.7 ± 9.9 | 72.3 ± 5.5 | 73.5 ± 6.3 |
| Gender (women/men) | 20/46 | 11/18 | 2/8 | 7/20 |
| No. of previous anti-VEGF treatments | — | — | 4.3 ± 2.8 | 1.7 ± 1.0 |
| No. of previous PDT treatments | — | — | — | 1.6 ± 0.7 |
| Initial visual acuity (logMAR) | 0.53 ± 0.40 | 0.47 ± 0.37 | 0.51 ± 0.36 | 0.61 ± 0.45 |
| Initial total foveal thickness (μm) | 401.0 ± 188.9 | 390.3 ± 143.2 | 434.8 ± 243.2 | 399.3 ± 211.8 |
| Cystoid macular edema | 20 | 9 | 3 | 6 |
| Serous retinal detachment | 57 | 27 | 8 | 22 |
| Subretinal hemorrhage | 42 | 22 | 6 | 14 |
| Pigment epithelial detachment | 30 | 12 | 7 | 11 |
| Greatest linear dimension | 4530 ± 1339 | 4147 ± 1171 | 4968 ± 1704 | 4780 ± 1301 |
| Additional anti-VEGF therapy | 10 | 7 | 1 | 2 |
| No. of additional anti-VEGF treatments | 0.39 ± 1.20 | 0.69 ± 1.65 | 0.30 ± 0.95 | 0.11 ± 0.42 |
| Range | 1 to 7 | 1 to 7 | 1 to 3 | 1 to 2 |
| Additional combined therapy | 21 | 9 | 4 | 8 |
| No. of additional combined therapy | 0.38 ± 0.63 | 0.31 ± 0.47 | 0.50 ± 0.71 | 0.41 ± 0.75 |
| Range | 1 to 3 | 1 | 1 to 2 | 1 to 3 |
In the treatment-naïve group, all eyes showed an exudative change resulting from the PCV; cystoid macula edema was seen in 9 eyes (31.0%), serous retinal detachment was seen in 27 (93.1%), and serosanguineous pigment epithelial detachment was seen in 12 (41.4%). Initial combined therapy substantially reduced the exudative change. At 3 months, reduced size of the cystoid space and a serous retinal detachment was seen in only 5 eyes and 6 eyes, respectively. Of the 12 eyes with a serosanguineous pigment epithelial detachment, 10 (83.3%) showed a reduction of its size and 5 (41.7%) showed complete resolution at 3 months. Of 24 eyes examined at 3 months with indocyanine green angiography, the polypoidal lesion was reduced in all eyes and had disappeared completely in 19 eyes (79.1%; Figures 1 and 2 ) . However, a branching vascular network remained in all eyes.
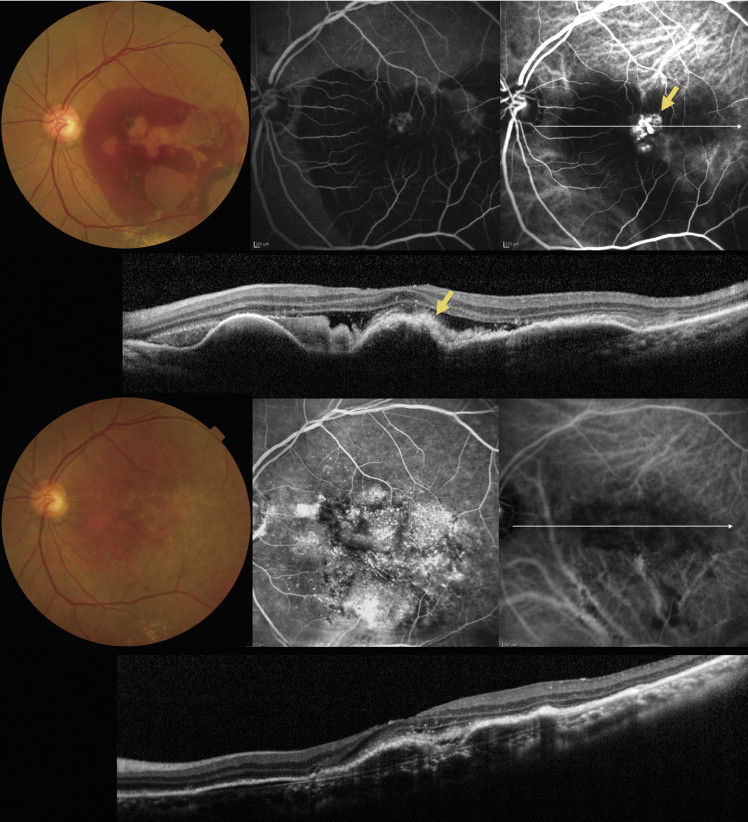
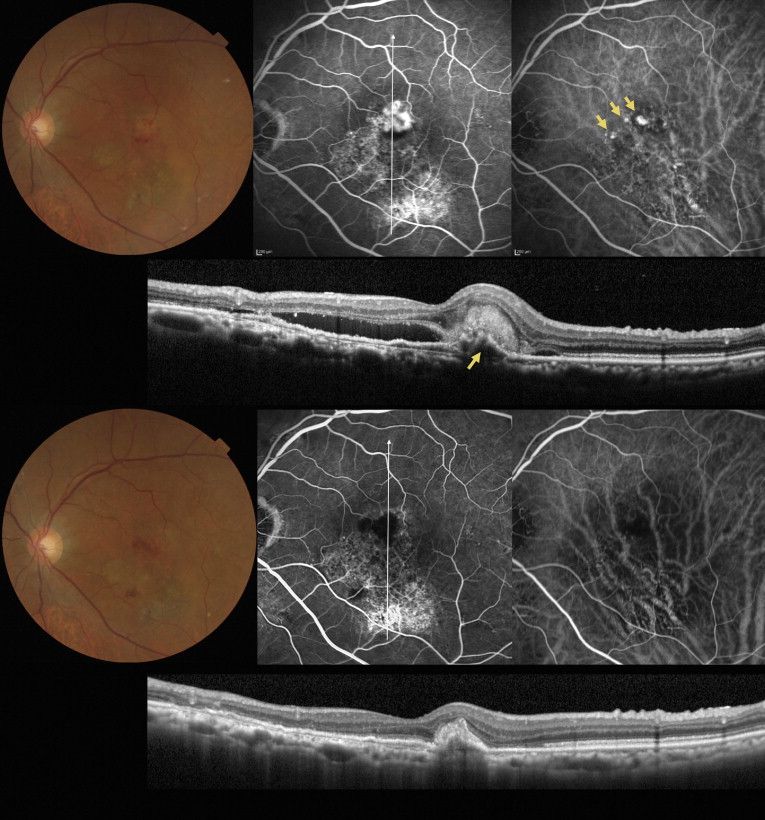
Figure 3 shows the change in VA and in foveal thickness after treatment of the treatment-naïve group. Combined therapy reduced substantially the exudative change immediately after initiation of treatment. The foveal thickness was reduced significantly from 390.3 ± 143.2 μm before treatment to 252.9 ± 104.3 μm ( P < .01) at 3 months and to 227.4 ± 50.3 μm ( P < .01) at 12 months. The mean VA before treatment (0.47 ± 0.37) also improved significantly, being 0.32 ± 0.30 ( P < .01) at 3 months. The improvement of VA was maintained until 12 months (0.29 ± 0.29; P < .01). At 12 months, significant improvement of VA was seen in 10 eyes (34.5%) and deterioration of VA was seen in 1 eye (3.5%) ( Figure 4 ) . Over this 12-month period, additional combined therapy to residual polypoidal lesions with an exudative change was performed in 9 eyes (31.0%). If only an exudative change remained, additional ranibizumab injections were given (7 eyes; 24.1%). In the treatment-naïve group, although 2 eyes showed subretinal hemorrhage (larger than 4 disc areas) after the combined therapy, the hemorrhage was absorbed spontaneously with no decrease in VA ( Figure 5 ) . During this 12-month period, no other serious adverse event was seen in the treatment-naïve group.
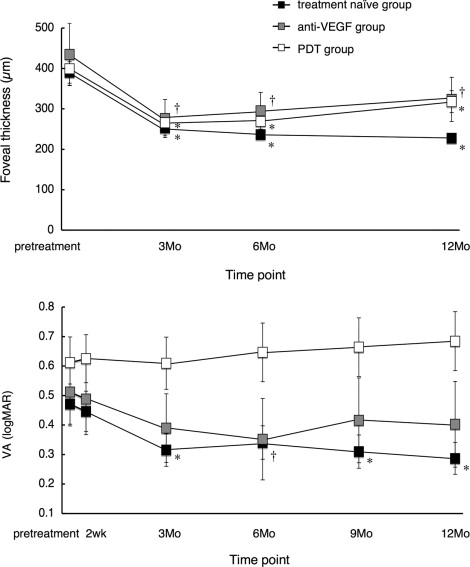
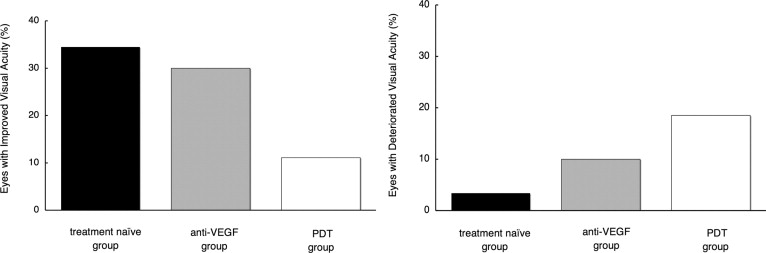
In the anti-VEGF group, combined therapy reduced substantially the exudative change. The mean foveal thickness was reduced significantly from 434.8 ± 243.2 μm before treatment to 276.1 ± 148.9 μm ( P < .05) at 3 months and to 311.4 ± 166.7 μm ( P < .05) at 12 months. The mean VA was improved from 0.51 ± 0.36 before treatment to 0.39 ± 0.37 at 3 months and to 0.40 ± 0.46 at 12 months, although this improvement was not statistically significant. At 12 months, significant improvement of VA was seen in 3 eyes (30.0%), whereas significant deterioration was seen in 1 eye (10.0%). During the first 12 months, additional combined therapy was administered in 4 eyes (40.0%) and additional ranibizumab injections were given in 1 eye (10.0%). During 12 months, no serious adverse event was seen in any eye of the anti-VEGF group.
In the PDT group, combined therapy reduced substantially the exudative change. The mean foveal thickness was reduced significantly from 399.3 ± 211.8 μm before treatment to 266.0 ± 95.2 μm ( P < .01) at 3 months and to 318.0 ± 140.6 μm ( P < .01) at 12 months. With treatment, however, the mean VA did not improve throughout the follow-up period. The mean VA (0.61 ± 0.45 before treatment) remained 0.61 ± 0.46 at 3 months and deteriorated somewhat to 0.68 ± 0.52 at 12 months ( Figure 6 ) . At 12 months, significant improvement of VA was seen in only 3 eyes (11.1%), whereas significant deterioration was seen in 5 eyes (18.5%). During 12 months, additional combined therapy was performed in 8 eyes (29.6%) and additional ranibizumab injections were given to in 2 eyes (7.4%). In this PDT group, 3 eyes showed extensive subretinal hemorrhage after treatment. Of these, vitreous hemorrhage developed in 2, necessitating pars plana vitrectomy.
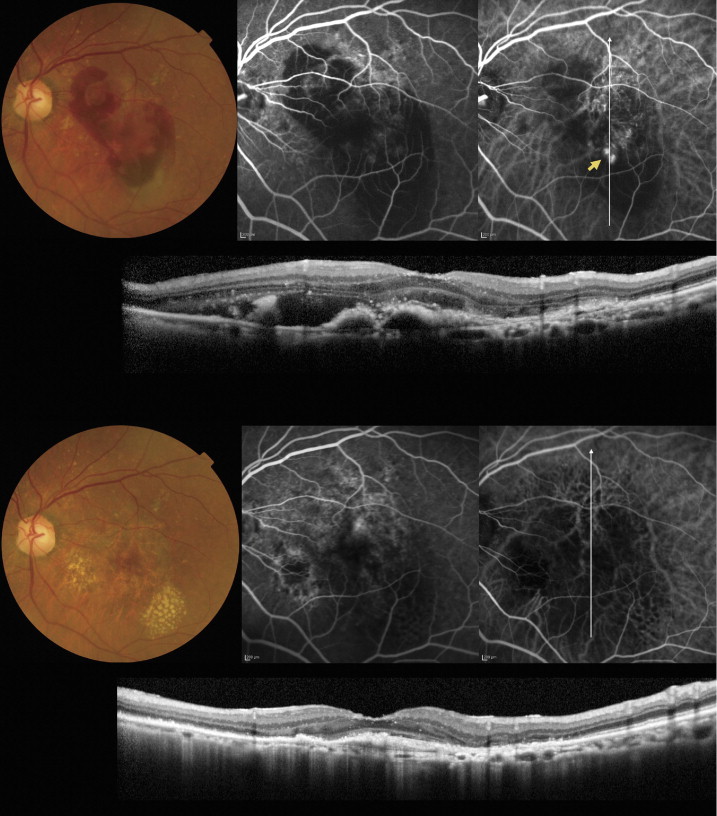
Table 2 shows the change in VA and foveal thickness from pretreatment values in each group. No difference was seen in the change of foveal thickness among the 3 groups. In addition, no significant difference was seen in the change of VA between the treatment-naïve group and the anti-VEGF group. However, change of VA in the PDT group was significantly worse than that of the treatment-naïve group at 3 months and thereafter ( P < .05).
| 2 Weeks | 3 Months | 6 Months | 9 Months | 12 Months | |
|---|---|---|---|---|---|
| Change in visual acuity (logMAR) | |||||
| Total group | −0.01 ± 0.14 | −0.09 ± 0.27 | −0.07 ± 0.30 | −0.06 ± 0.35 | −0.07 ± 0.35 |
| Treatment-naïve group | −0.02 ± 0.14 | −0.16 ± 0.27 | −0.13 ± 0.27 | −0.16 ± 0.35 | −0.18 ± 0.34 |
| Anti-VEGF group | −0.02 ± 0.14 | −0.12 ± 0.20 | −0.16 ± 0.26 | 0.10 ± 0.34 | −0.11 ± 0.34 |
| PDT group | 0.01 ± 0.14 | 0.00 ± 0.26 a | 0.03 ± 0.33 a | 0.05 ± 0.33 a | 0.07 ± 0.33 a |
| Change in foveal thickness (μm) | — | ||||
| Total group | — | −139.0 ± 148.3 | −141.7 ± 162.1 | — | −125.9 ± 189.5 |
| Treatment-naïve group | — | −137.4 ± 150.4 | −154.1 ± 141.2 | — | −171.3 ± 150.2 |
| Anti-VEGF group | — | −158.7 ± 154.2 | −139.3 ± 154.5 | — | −123.4 ± 262.4 |
| PDT group | — | −133.4 ± 149.2 | −130.1 ± 187.4 | — | −81.4 ± 190.8 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


