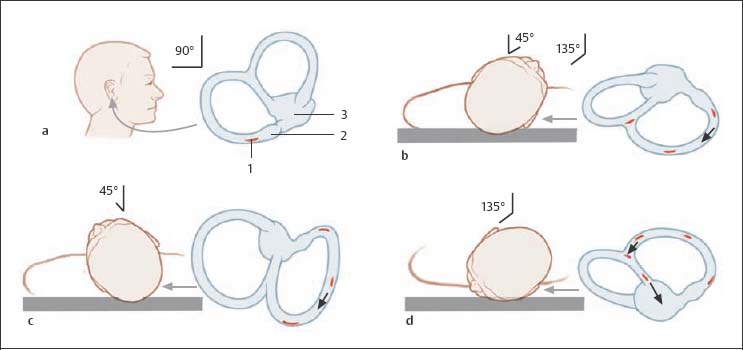
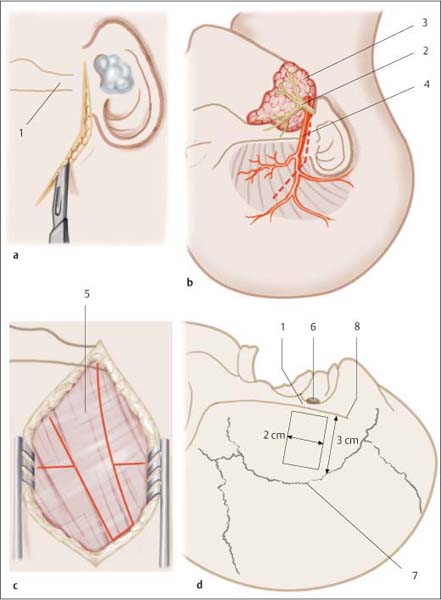
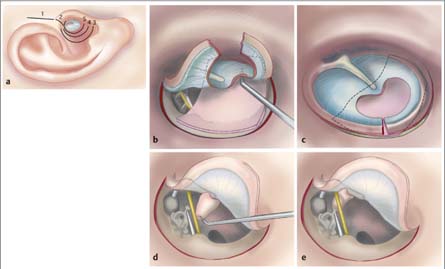
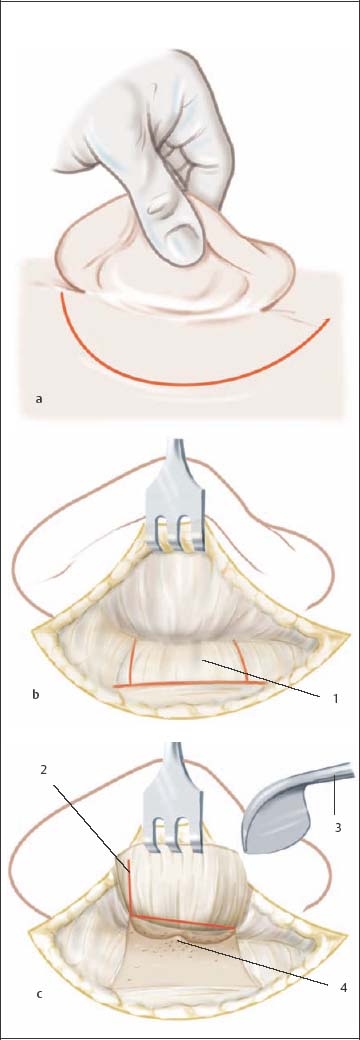
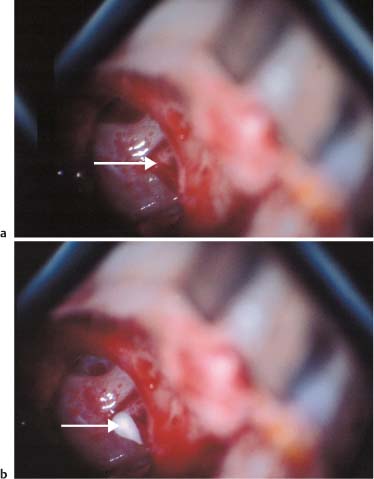
18 Treatment of Injuries of the Ear and Lateral Skull Base Any injury of the external ear must receive primary treatment. Seroma or hematoma causes shearing injury to the cartilage of the ear. Fluid accumulation between cartilage layers does not resolve primarily and must be drained. Aspiration of fluid is rarely successful and thus surgical drainage is usually necessary. The cavity is opened, either one or both sides of the cartilage layers are removed, and the cutaneous layers fixed to one another under pressure (Fig. 18.1). Intervention in adults can be performed under local anesthesia; in children, general anesthesia is advised. A retroauricular or anterior approach is possible. The skin is closed primarily and the wound drained. Mattress sutures are then placed over a pressure dressing for compression and modeling of the auricle. The cavity can be conformed using small cotton balls and the helix using cotton-tipped swabs. The cotton balls and swabs are removed after 10 days and the sutures, if reachable, after 7 days. Fig. 18.1 Surgical management of an auricular hematoma. a Hematoma and clear loss of antihelix fold. b Decompression of the hematoma and exposure of cartilage. c Modeling bandage on the auricle. Whenever possible, auricular injuries must be primarily reconstructed. Intervention can be done under local anesthesia or under general anesthesia for children. Cartilage suturing should be avoided; in most cases coaptation of wound margins is sufficient. A compression dressing using mattress sutures or ointment-soaked gauze packing should be applied after intervention to protect against hematoma development. Primary adaptation can be attempted if the amputated portion of the ear is transported with the patient. In isolated instances, microvascular grafting is possible, though generally an alternative procedure should be used. An incision is made over the mastoid skin at the level of the amputation margins. The retroauricular skin is sutured to the skin of the mastoid directed toward the ear. The skin is completely separated from the retroauricular area of the amputated portion of the auricle and its anterior aspect sutured to the corresponding part of the remaining ear. The severed portion of the auricle is then fixed to the mastoid using through-and-through mattress sutures. This may require resecting mastoid skin and a segment of the mobilized retroauricular skin of the amputated portion of the auricle. The free skin margins of the amputated auricle are then sutured to the mastoid. The mattress sutures should be left in place for 10–14 days. In a second operation after ca. 3–4 months, the auricle can be lifted away from the mastoid. The retroauricular skin defect is closed using a free skin graft from the opposite side. Primary closure of the skin defect is usually possible (Fig. 18.2). For partial loss of the auricle with loss of the amputated portion primary management is the first step in definitive plastic/reconstructive surgery. For a small defect in the helix region, reconstruction in the form of a wedge-shaped resection may be wise. If more than 1/3 of the auricle has been lost, reconstructive surgery must be planned. This involves connecting the edges of the skin of the auricle with the skin of the mastoid. At the height of the amputation, a skin incision is made over the mastoid and the margins are connected with the margins of the auricular skin. After 2–3 months reconstruction, for example with cartilage grafts, can begin (Fig. 18.2). Fig. 18.2 Management of a partial amputation of the auricle. a Visible partial amputation of the right auricle. b Healed amputation, still attached to the cranium. c Appearance after elevation of the auricle. Primary management of inner ear and vestibular disturbances is conservative. Primary management of posttraumatic inner ear hearing impairment and vestibular disturbances (labyrinthine concussion, blast and explosion trauma) is conservative. Medication therapy has the goal of restoring lost function. Auditory, Vestibular Disorder, p. 60. Functional Testing, Chapter 7, p. 61. Fig. 18.3 Treatment of benign paroxysmal positional vertigo (BPPV, canalolithiasis) with positioning maneuvers based on Parnes and Epley. The blue arrow indicates the view of the labyrinth. The open oval inside shows the previous position of the particles in the “most dependent” portion of the posterior canal. The dark oval indicates the new position. a, b The patient is reclined to the supine position (headrest is lowered 45°), the affected (lesional) ear is rotated 45° toward the afflicted side. c The affected ear is slowly turned (60 seconds) to the contralesional side, until the healthy ear is rotated 45° laterally (to the healthy side). d The patient is turned another 135° in this direction (60 seconds), until he rotates over the healthy side onto his side. At the end of this rotation, the patient’s nose is pointing toward the floor. The patient then slowly assumes the sitting position, holding his head up. A cervical support must be worn for 48 hours to prevent abrupt head-turning movements. Fig. 18.4 Schematic illustration of a Type I tympanoplasty by endaural approach (modified from Strutz and Mann 2001). a Endaural incisions (1, vertical l.; 2, intercartilaginous l.; 3, 4, 5 lateral, intermediate, and medial [circumferential]). b, c Tympanic membrane injury. The limbus was severed at a right angle, and an upper and a lower tympanomeatal flap are formed. The perforation is positioned with perichondrium in the underlay technique. Both tympanomeatal flaps are reflected backward. d, e Injury of the ossicles. Incus interposition between malleus handle and stapes. The reconstructed ossicular chain must be held under tension. Functional Testing, Chapter 7, p. 61. Following infiltration with a local anesthesia solution containing a vasoconstrictor, an endaural incision is made between the tragus and the crus of the helix. A tympanomeatal flap is created, and reflected forward. The mobility of the ossicular chain is tested (Fig. 18.4a–c). Following infiltration with local anesthetics, a retroauricular skin incision is made 5 mm inferior to the postauricular crease. After exposing the mastoid plane and the entrance to the external acoustic canal with a periosteal elevator, the canal skin can be incised. A tympanomeatal flap is then created (Fig. 18.5). Fig. 18.5 Tympanoplasty: incision and dissection via a postauricular approach (modified from Fisch 1994). a Retroauricular skin incision (ca. 2 cm from the postauricular crease). b Formation of a periosteal flap by incising to the cortical bone of the mastoid process. c Elevation of the periosteal flap and incision of the external auditory canal to proceed further. 1 Incision to the mastoid, 2 opening of the auditory canal, 3 periosteal elevator. Access is through a craniotomy cranial to the external auditory canal. After lifting the dura from the floor of the middle cranial fossa, the middle meningeal artery and arcuate eminence are identified. Fixation of the bone flap is performed after concluding reconstruction (Fig. 18.6). Injuries of the external auditory canal caused by foreign objects can usually be managed with careful coadaptation of meatal skin, placement of silicone tubing, and auditory canal packing for about 3 weeks. If there is a fracture of the anterior canal wall, arising in conjunction with temporomandibular joint injury, reduction of the fracture can be achieved using a narrow periosteal elevator. This is followed by packing for 3 weeks. An exception is a canal injury caused by hot welding slag. Management requires complete removal of the skin of the external auditory canal, as nitrates formed in the welding process make skin healing impossible. Reconstruction is then with a free skin graft, a tympanoplasty may be required. Isolated injury of the TM without any sign of injury to the ossicles can be sufficiently managed with splinting of the tympanic membrane. If there is discharge from the middle ear (e. g., swimming accident), antibiotic therapy for 5–7 days must precede any splinting to be certain of cessation of infection. The TM can be splinted under local or brief general anesthesia. A transmeatal approach is usually possible, though occasionally an endaural or postauricular approach can be prudent. Intervention should attempt to free the folded-over flaps of the tympanic membrane and return them to their original position. It is sometimes advisable to support the edges of the tympanic membrane with tympanic packing. After placing silicone sheets, the external auditory canal is packed for 3 weeks. Persistent defects must be managed with tympanoplasty (Fig. 18.4d, f). Fig. 18.6 Transtemporal approach to the cerebellopontine angle. a Preauricular incision extending to the temporal region. b Surgical anatomy of the temporal region. c Incision in the temporalis muscle region to expose the calotte. d Depiction of the bone flap that is to be elevated for exposure of the cerebellopontine angle. 1 Zygomatic arch, 2 facial nerve, 3 parotid gland, 4 temporal artery, 5 temporalis muscle, 6 external auditory canal, 7 temporoparietal suture, 8 zygomatic line. Occasionally a displaced fracture involving the posterior wall of the auditory canal can restrict mobility of the ossicles, without causing direct injury. In such cases, an attempt should be made at removing the protruding fracture ends with a House curette. Disarticulation of the incudostapedial joint should be managed with a type III tympanoplasty. This involves removing the incus from its anatomic position and placing it as an autologous transplant between the malleus and stapes. Interposition of a heterologous graft is also possible. Fractures of individual stapedial crura can be fixated with bone cement (Fig. 18.7). If this is unsuccessful, or there is fracture of the stapedial footplate, stapedioplasty is necessary. Fig. 18.7 Type II tympanoplasty for stapedial crus fracture. a Visible fracture of the stapedial crus (arrow). b Management of the fracture with cement (arrow). Suspected rupture is managed by covering the round and oval windows with connective tissue. Prior to covering the windows, rupture can be detected by placing sponges for beta transferrin detection or with intrathecal fluorescein sodium. The use of fibrin adhesive to secure the connective tissue covering is mandatory. Depending on localization of the fracture gap, persistent cerebrospinal fluid (CSF) otorrhea should be managed by mastoidectomy (postauricular approach) using a diamond burr to expose the fracture gap and seal it.
 Flowchart and checklist Injuries of the Ear and Lateral Skull Base, p. 18.
Flowchart and checklist Injuries of the Ear and Lateral Skull Base, p. 18.
 Antibiotic Therapy, Chapter 24, p. 210.
Antibiotic Therapy, Chapter 24, p. 210.
 Diagnosing Injuries of the Ear, Chapter 7, p. 53.
Diagnosing Injuries of the Ear, Chapter 7, p. 53.
Injuries of the External Ear
 Diagnosing Injuries of the External Ear, Chapter 7, p. 53.
Diagnosing Injuries of the External Ear, Chapter 7, p. 53.
Indications
Surgical Methods
Seroma and Hematomas of the Ear

Injuries of the Auricle
Auricular Amputation

Injuries of the Vestibulocochlear System
Indications
Conservative Management
 Injuries of the Petrous Temporal Bone and Labyrinth, Chapter 7, p. 57.
Injuries of the Petrous Temporal Bone and Labyrinth, Chapter 7, p. 57.
Inner Ear Auditory Dysfunction
 Hearing impairment should be treated with procaine (increasing from 400 to 1000 mg/daily) for 7–10 days in step-up doses (over 4–6 hours) in a carrier solution (e. g., HAES 10 %).
Hearing impairment should be treated with procaine (increasing from 400 to 1000 mg/daily) for 7–10 days in step-up doses (over 4–6 hours) in a carrier solution (e. g., HAES 10 %).
 For considerably impaired hearing function, additional corticoid administration (massive dose therapy) in step-down doses may be advisable (1000, 500, 250, 125 mg prednisolone, descending further). Alternatively, cortisone can be administered according to Stennert¢¢s scheme (cf. Table 18.1).
For considerably impaired hearing function, additional corticoid administration (massive dose therapy) in step-down doses may be advisable (1000, 500, 250, 125 mg prednisolone, descending further). Alternatively, cortisone can be administered according to Stennert¢¢s scheme (cf. Table 18.1).
 If after 5 days there is no change in hearing ability and/or vestibular disorder using one of the infusion therapies mentioned above, a tympanoscopy should be performed to rule out rupture of the round and oval windows.
If after 5 days there is no change in hearing ability and/or vestibular disorder using one of the infusion therapies mentioned above, a tympanoscopy should be performed to rule out rupture of the round and oval windows.
 If hearing ability is not restored, or tinnitus eliminated, with the therapies mentioned above 10 days after the blast or explosion trauma, hyperbaric oxygen therapy can be considered.
If hearing ability is not restored, or tinnitus eliminated, with the therapies mentioned above 10 days after the blast or explosion trauma, hyperbaric oxygen therapy can be considered.
Vestibular Disorder
 Vestibular dysfunction may initially require sedation of the patient as well as symptomatic administration of vestibular suppressant drugs (e. g., dimenhydrinate, benzodiazepine). Administration of betahistidine should be avoided in the acute phase as it can lead to delayed compensation of the vestibular disorder.
Vestibular dysfunction may initially require sedation of the patient as well as symptomatic administration of vestibular suppressant drugs (e. g., dimenhydrinate, benzodiazepine). Administration of betahistidine should be avoided in the acute phase as it can lead to delayed compensation of the vestibular disorder.
 Exercise therapy under the care of a physical therapist should be initiated as soon as possible for vestibular dysfunctions.
Exercise therapy under the care of a physical therapist should be initiated as soon as possible for vestibular dysfunctions.
 Benign paroxysmal positional vertigo (BPPV) is treated with the positioning maneuver based on Parnes and Epley (Fig. 18.3).
Benign paroxysmal positional vertigo (BPPV) is treated with the positioning maneuver based on Parnes and Epley (Fig. 18.3).
Surgical Management
 Diagnosis of Injuries of the Middle Ear, Chapter 7, p. 55.
Diagnosis of Injuries of the Middle Ear, Chapter 7, p. 55.
Approaches
Endaural Approach
Postauricular Approach
Transtemporal Approach
Surgical Techniques
Injury of the Auditory Canal
Injuries of the Tympanic Membrane (TM)
Injuries of the Ossicles
Incus/Stapes Injury
Stapedial Fracture
Ruptures of the Round and Oval Windows
Cerebrospinal Fluid Otorrhea
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


