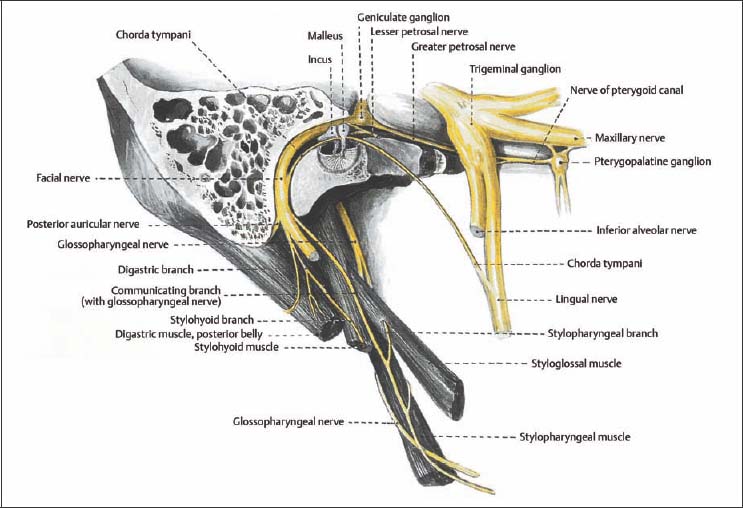
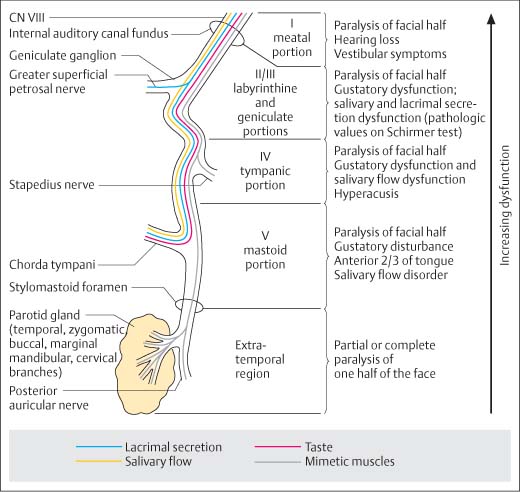
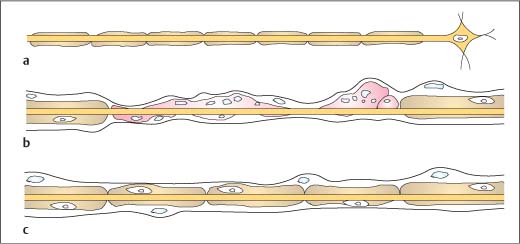
8 Diagnosing Injuries of the Facial Nerve The course of the facial nerve can be divided into three segments: The intracranial segment extends ca. 3.5–6 mm from where it emerges from the brainstem to the entrance to the internal auditory canal. The intratemporal segment is divided into five portions: The meatal portion extends from the opening of the internal auditory canal to the fundus of the internal auditory canal, the entrance to the fallopian canal. The fallopian canal begins at the internal auditory canal fundus and ends at the stylomastoid foramen. The nerve is void here of perineurium or epineurium, as is also the case in the cerebellopontine angle. The cerebrospinal fluid-containing subarachnoidal space extends to the exit of the superficial petrosal nerve. Not until the ganglion is there formation of epineural and perineural connective tissue. In the geniculate portion the ganglion itself lies with pseudounipolar parasympathetic cells on the facial nerve genu. Fig. 8.1 Intratemporal course of the facial nerve (from Tillmann 1997). The tympanic portion extends from this region to the pyramidal eminence where it continues into the mastoid portion with the formation of the genu of the third facial nerve, which is up to 2 cm long. It ends where the nerve exits the cranial base at the stylomastoid foramen (Fig. 8.1). Topodiagnostic localization of injuries is based on anatomic relationships (Fig. 8.2): – Preganglionic secretion fibers to the lacrimal gland: These branch off from the nerve at the geniculate ganglion into the greater superficial petrosal nerve. A lesion in the preganglionic or ganglionic segments leads to unilateral impairment of lacrimal secretion. A Schirmer test for pathologic values can be useful for detection. – Preganglionic secretion fibers to the submandibular gland: These exit the nerve together with the chorda tympani. Damage in the tympanic portion causes reduced ipsilateral saliva production of the submandibular gland. A sialometry test is used (cannulation and collection of whole saliva). A pathologic sialogram, along with remarkable Schirmer values on the same side, are a sign of damage in the tympanic portion of the nerve course. If the Schirmer test is additionally positive, the lesion can be presumed to be more centrally localized (usually in the labyrinthine portion). – Motor fibers to the stapedius muscle: Damage occurring proximal to the pyramidal process causes reflex dysfunction or increased reflex threshold on the injured side. Fig. 8.2 Schematic illustration of topodiagnosis of facial nerve lesions. Nerve damage resulting from fracture is usually caused by blunt trauma. There is crushing damage on both sides of the injury site. The nerve lesion itself may exhibit varying degrees of damage: A variety of scales are used for classification of facial nerve damage according to the severity of injury. The scale most commonly used is the House–Brackmann scale. The House–Brackmann scale is internationally the most widely used classification system for clinical evaluation of facial nerve function. The score is based on assessment of functional impairment, declining gradually from I–VI (Table 8.1). Fig. 8.3 Schematic illustration of neurapraxia (modified from Richter 1992). a Intact neuron, made up of cell body, axon, and dendrites. b Degeneration of the myelin sheath and proliferation of Schwann cells. c Remyelinization of the axon, complete recovery.
 Checklist Injuries of the Facial Nerve, Chapter 3, p. 19.
Checklist Injuries of the Facial Nerve, Chapter 3, p. 19.
 Treatment of Injuries of the Facial Nerve, Chapter 18, p. 153.
Treatment of Injuries of the Facial Nerve, Chapter 18, p. 153.
Surgical Anatomy
 intracranial portion;
intracranial portion;
 intratemporal portion;
intratemporal portion;
 extratemporal portion.
extratemporal portion.
Intracranial Segment
Intratemporal Segment
 meatal;
meatal;
 labyrinthine;
labyrinthine;
 geniculate;
geniculate;
 tympanic;
tympanic;
 mastoid segment.
mastoid segment.
 Organ functions (lacrimal secretion, salivary flow, taste sensation, and stapedial reflexes) remain intact if injury is localized peripheral to the corresponding nerve branches.
Organ functions (lacrimal secretion, salivary flow, taste sensation, and stapedial reflexes) remain intact if injury is localized peripheral to the corresponding nerve branches.
 Centrally localized lesions involve loss of the following functions:
Centrally localized lesions involve loss of the following functions:
Pathomechanism and Classification
 Neurapraxia: The electrical conductivity of the nerve fails to exhibit an elevated threshold in response to stimulation (Fig. 8.3). Restitution of nerve function occurs spontaneously and within a short period of time. Even total palsy is managed conservatively.
Neurapraxia: The electrical conductivity of the nerve fails to exhibit an elevated threshold in response to stimulation (Fig. 8.3). Restitution of nerve function occurs spontaneously and within a short period of time. Even total palsy is managed conservatively.
 Axonotmesis: Regeneration takes considerably longer than with neurapraxia.
Axonotmesis: Regeneration takes considerably longer than with neurapraxia.
 Neurotmesis: The nerve is transsected. The nerve does not heal spontaneously and must be surgically reconstructed. This results in defect healing with synkinesis and residual palsy.
Neurotmesis: The nerve is transsected. The nerve does not heal spontaneously and must be surgically reconstructed. This results in defect healing with synkinesis and residual palsy.
Classification
House–Brackmann Scale
I | Normal symmetrical function in all regions |
II | Mild motor weakness, only visible on close inspection; complete lid closure with minimal effort, minimal asymmetry with strong facial expression |
III | Marked unilateral motor weakness, complete lid closure with effort, asymmetry of the mouth movements with maximum intention, minimal synkinesis |
IV | Marked asymmetry of mimetic muscles, incomplete lid closure, marked asymmetry of the mouth with maximum effort, marked synkinesis and mass motion |
V | Barely detectable mimetic muscle motion, minimal motion of the corners of the mouth, no synkinesis or mass motion |
VI | Absence of mimetic muscle motion, loss of muscle tone, no synkinesis |
Clinical Signs and Functional Tests
Topodiagnostic Evaluation
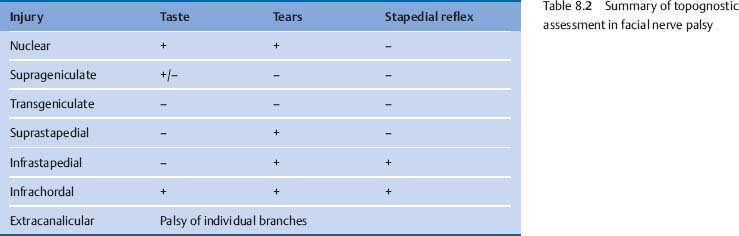
Table 8.2 provides a summary of topodiagnosis of facial palsy.
Tearing (Schirmer Test)
This test distinguishes between pre-ganglionic and post-ganglionic injury. After administering a local anesthetic, lacrimal secretion is measured in both eyes for five minutes using filter papers which are placed in the conjunctival sac.
In the Schirmer test if lacrimal secretion measured on one side is less than 70 % that of the opposite side, this is considered a pathologic finding (positive).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


