Purpose
To evaluate the safety and bioactivity of MP0112, a designed ankyrin repeat protein (DARPin) that specifically binds vascular endothelial growth factor (VEGF) in patients with diabetic macular edema (DME). DARPins are a novel class of proteins selected for specific, high-affinity binding to a target protein.
Design
Phase I/II, open-label, multicenter dose-escalation trial.
Methods
After a single intravitreal injection of MP0112, the main outcomes were safety assessments, aqueous MP0112 levels, change in best-corrected visual acuity (BCVA), and foveal thickness measured by optical coherence tomography. Six cohorts were planned, but only 3 were enrolled (0.04, 0.15, 0.4 mg), because a maximally tolerated dose of 1.0 mg was identified in a parallel age-related macular degeneration trial.
Results
Median aqueous concentration of MP0112 was 555 nM 1 week and >10 nM in 3 of 4 patients 12 weeks post injection of 0.4 mg. Median BCVA improvement at week 12 was 4, 6, and 10 letters in cohorts 1, 2, and 3. Ocular inflammation was observed in 11 patients (61%) and was severe in 1. High-resolution chromatography separated proinflammatory impurities from MP0112, resulting in a new formulation.
Conclusions
A single intraocular injection of 0.4 mg MP0112 resulted in levels above the half-maximal inhibitory concentration and neutralization of VEGF in aqueous humor for 8-12 weeks. Despite inflammation in several patients, there was prolonged edema reduction and improvement in vision in several patients. The source of the inflammation was eliminated from a new preparation that is being tested in an ongoing clinical trial.
Diabetic macular edema (DME) is a highly prevalent cause of vision loss. Although its pathogenesis is not completely understood, recent studies have helped to elucidate important aspects. Retinal hypoxia is an important feature, because supplemental inspired oxygen reduces DME. Vascular endothelial growth factor (VEGF) is upregulated in hypoxic retina, and recent studies using nonselective and selective antagonists have demonstrated that VEGF is an important stimulator of DME.
There are several types of VEGF antagonists. Ranibizumab is an Fab fragment that binds all isoforms and active proteolytic fragments of VEGF. Several studies have demonstrated that intraocular injections of ranibizumab provide benefit in patients with DME. Ranibizumab is approved in Europe and the United States for treatment of DME. Bevacizumab is a humanized full-length monoclonal antibody that also binds all isoforms and fragments of VEGF. Intraocular injections of bevacizumab have shown benefit in patients with DME and it is widely used off label. Aflibercept is a recombinant protein that binds all isoforms and active fragments of VEGF and placental growth factor, and recent studies have suggested that it also will be useful for DME.
Antibodies (ranibizumab and bevacizumab) and receptor fragments (aflibercept) take advantage of protein motifs specifically designed in nature to bind to a ligand. Repeat proteins are also utilized in nature for binding. They consist of small structural units (repeats), such as leucine-rich repeats or ankyrin repeats, linked together to form domains. Each repeat binds tightly to preceding and following repeats and also has variable sequences that do not interact with other repeats and are oriented on the surface of the domain. The variable surface residues of the repeats provide the external shape and hence the specificity for binding to external partners. These principles were used to design an amino acid sequence motif with fixed and variable portions, the former mediating the interaction between repeats and the latter mediating part of the external shape available to engage a target. Designed ankyrin repeat protein libraries result in production of numerous domain proteins, designed ankyrin repeat proteins (DARPins), with varied shapes that can be screened for binding to target proteins. Using this strategy, a DARPin that selectively binds all VEGF-A isoforms with a dissociation constant (Kd, a measure of affinity) of 2 pM, MP0112, was identified (Molecular Partners AG, Zurich, Switzerland; MP is for Molecular Partners and 0112 is the identifying number for this DARPin). In this study, we tested the safety, tolerability, pharmacokinetics, and biologic activity of a single intraocular injection of MP0112 in patients with DME.
Subjects and Methods
This was a phase I/II, open-label, nonrandomized, dose-escalation clinical trial conducted at 4 sites in the United States. The study and data accumulation were carried out with approval from the Institutional Review Board (IRB) at Johns Hopkins University and Western IRB. Informed consent for the research was obtained from all participating patients and the study complied with the Declaration of Helsinki and the Health Insurance Portability and Accessibility Act. The study is registered at www.clinicaltrials.gov under the identifier NCT01042678 . The duration of the study was 16 weeks.
Patient Eligibility and Exclusion Criteria
Male or female patients (18 or older) with type 1 or type 2 diabetes were eligible if they had DME with best-corrected visual acuity (BCVA) of 20/40 to 20/400 in Snellen equivalent and central subfield thickness ≥250 μm measured by time-domain optical coherence tomography (TD-OCT, Stratus 3; Carl Zeiss Meditec, Dublin, California, USA). Patients were excluded if they had: (1) any potential contributing causes of reduced visual acuity other than DME; (2) received focal/grid laser treatment within 4 months; (3) received intraocular surgery or an intraocular injection of a steroid or anti-VEGF agent within 3 months; or (4) HbA1C ≥12%. Female patients of childbearing potential were required to have a negative pregnancy test and to use reliable contraception.
Study Protocol
The primary objective of this study was to assess the safety and tolerability of single intravitreal injections of MP0112. Secondary outcomes included changes in visual acuity, central foveal thickness (based on OCT), pharmacokinetics, aqueous humor VEGF levels, and serum anti-MP0112 antibodies. Once consented, a screening visit was done in which the patient’s medical history was obtained, including measurement of BCVA using the protocol established for the Early Treatment Diabetic Retinopathy Study (ETDRS), complete eye examination, TD-OCT and spectral-domain OCT (SD-OCT), fundus photographs, and fluorescein angiography. Each patient received a single intravitreal injection of MP0112 during the baseline visit. Follow-up visits were scheduled for 1 and 3 days and 1, 4, 8, 12, and 16 weeks after treatment. The first 3 visits were safety visits in which patients had assessment for adverse events, concomitant medications, eye examination, and pharmacokinetic analyses. At each of the other study visits, patients had assessment for adverse events, concomitant medications, measurement of BCVA, complete eye examination, and TD-OCT and SD-OCT. After the first cohort was enrolled, the protocol was amended to include OCTs at the 1-week visit for cohorts 2 and 3 to help determine if changes in visual acuity could be attributed to changes in macular edema. At selected study sites, aqueous humor samples (approximately 100 μL) were collected before MP0112 injection and at weeks 1, 4, 8, and 12. Samples were analyzed for active MP0112 and free VEGF concentrations by enzyme-linked immunosorbent assay (ELISA). Fundus photographs and fluorescein angiograms were done at baseline and at week 12.
A single patient was initially dosed in each dose cohort and if no severe ocular (sight-threatening) or serious drug-related adverse events were noted at 1 week post injection, the remaining 5 patients were enrolled. After all 6 patients in a cohort were dosed and 2-week safety data were collected, dose escalation could proceed if no severe sight-threatening drug-related ocular adverse events had occurred and no more than 2 patients had experienced a drug-related ocular dose-limiting toxicity, described as (1) intraocular inflammation, uveitis, or vitritis, defined as a change of 2 units on standard grading scales; (2) sustained elevation of intraocular pressure to >30 mm Hg; or (3) loss of VA >15 letters.
Study Treatments
Patients were given an intraocular injection of MP0112 using standard injection techniques including use of a lid speculum, topical anesthesia, cleaning the injection site with 5% povidone-iodine, and then injection of 0.05 mL of study drug with a 30-gauge needle. After injection the ability to count fingers was assessed and the fundus was examined with indirect ophthalmoscopy to assess retinal perfusion. After all patients in a cohort were dosed, the medical monitor and the study investigators reviewed all data and a teleconference with investigators was held to determine if the study should proceed to the next cohort. Planned doses were 0.04, 0.15, 0.4, 1.0, 2.0, and 3.6 mg (n = 6 for each dose), but only the first 3 dose levels were enrolled and evaluated, because of a maximally tolerated dose of 1.0 mg being reached in a parallel age-related macular degeneration trial (see Discussion section in this article). At the investigator’s discretion, standard-of-care alternative therapy could be administered at week 4 or later to patients who experienced a reduction in BCVA of 3 or more lines and at week 12 to patients without evidence of clinical improvement (BCVA or macular thickness).
Optical Coherence Tomography
At each clinical site, certified technicians acquired OCT scans using the TD-OCT Stratus 3 OCT (Carl Zeiss Meditec) and either 1 of the 2 SD-OCTs, Spectralis (Heidelberg Engineering, Vista, California, USA) or Cirrus OCT (Carl Zeiss Meditec). The selection of type of SD-OCT was dependent upon availability of the OCT device at the site. The same SD-OCT device was used for all visits for a given patient to allow comparison between visits for a given patient. However, because of the differences in thickness measurements between the 2 SD-OCT devices, foveal thickness values from SD-OCT were not compared across patients. The central subfield thickness, which is the average thickness within the central 1 mm of the fovea, was used as a measure of foveal thickness for all OCT devices. Scans were acquired using the fast macular scan protocol on Stratus. This consists of 6 line scans, each 6 mm long, centered on the fixation point and spaced 30 degrees apart around the circumference of a circle. Scans were acquired using the OCT volume mode on Heidelberg Spectralis. This consists of 25 horizontal lines covering a total area of 20 × 20 degrees of the macula, with a distance of 240 μm between the horizontal lines. Each horizontal scan was averaged at least 15 times. The TruTrak function of the Spectralis OCT device was used to acquire follow-up scans with the same settings as the scan at the initial visit to allow head-to-head comparison across visits for a given patient. The scan at the initial visit was set as reference; all subsequent OCT scans were acquired as progression scans. Scans were acquired using the 512 × 128 macular cube on the Cirrus. This consisted of 128 horizontal lines scanning a macular area of 6 mm × 6 mm, with 512 A-scans per line.
Data Analysis
OCT scans, fundus photographs, and FAs were graded and analyzed at the Retinal Imaging Research and Reading Center at the Wilmer Eye Institute. Scans were submitted via a password-protected web interface to the reading center. Readers reviewed the scans for artifacts and corrected for algorithm errors using the proprietary software (Stratus version 5.0.1, Heidelberg Spectralis version 5.3, and Cirrus research browser version 5.2). SD-OCT scans were further corrected for grid placement by manually moving the ETDRS grid to the foveal center in cases when automatic placement of the grid appeared to be incorrect. The software for Stratus did not have this capability.
Ocular Pharmacokinetics Determination
Anterior chamber taps were performed under topical anesthesia by biomicroscopic observation of the eye with the patient seated at a slit lamp. A 30-gauge needle was inserted into the anterior chamber and 0.1 mL of aqueous was removed and stored frozen at −80 C until assayed. Aqueous humor samples from anterior chamber taps were collected at baseline, week 1, week 4, week 8, and week 12 at selected sites. Active MP0112 concentrations in aqueous humor were determined by an ELISA method that was developed and validated for the determination of MP0112 in human serum. Briefly, the assay relied on VEGF-A–coated plates and an MP0112-specific monoclonal antibody coupled to colorimetric readout. The lower limit of quantification of the assay is 0.3 nM of MP0112. Free human VEGF-A (hVEGF-A) concentrations in aqueous humor were determined using the Quantikine VEGF-A sandwich ELISA (R&D Systems, Minneapolis, Minnesota, USA) according to the manufacturer’s instructions. In brief, a mouse monoclonal antibody specific for VEGF is used as capturing antibody. After incubation with VEGF-containing samples and washing, a horseradish peroxidase–linked polyclonal antibody specific for VEGF is used for detection of VEGF bound to the capturing antibody. Since MP0112 has an extremely high affinity to VEGF and remains totally saturated in the presence of the antibody, only free VEGF can bind to the capturing antibody and its concentration can be accurately determined. The lower limit of quantification of the Quantikine assay is at 0.1 pM VEGF-A, so that final concentrations above 1 pM in aqueous humor samples (diluted 10-fold in the assay) could be determined.
Results
Patient Demographics and Baseline Characteristics
Six patients were entered into each of 3 cohorts and given a single intraocular injection of 0.04 mg, 0.15 mg, or 0.4 mg of MP0112. The mean age was 64.8 years (range 50-82); 11 patients were male and 7 were female; 15 were white and 3 were Hispanic. All patients reported prior treatment in the study eye for DME: bevacizumab in 10 (56%), ranibizumab in 2 (11%), and “other” treatments in all 18. One patient in cohort 1 exited the study at week 12 because of deteriorating vision and alternative treatment was requested; the other 17 patients completed the study. The mean BCVA letter score at baseline was 57.1 ± 11.2 (range 30-72) with Snellen equivalent of 20/63 or better in 50% and 20/80-20/250 in 50%. Mean central subfield thickness by Stratus 3 OCT was 434.9 ± 124.0 μm.
Pharmacokinetics of MP0112 and Aqueous Humor VEGF Levels
Three patients in each of cohorts 1 and 2 and 4 patients in cohort 3 consented to have anterior chamber taps. Aqueous levels of MP0112 were undetectable at baseline and at 1 week after a single intravitreous injection of MP0112 ranged from 13 to 26 nM for cohort 1 (0.04 mg dose), 26 to 270 nM for cohort 2 (0.15 mg dose), and 230 to 622 nM for cohort 3 (0.4 mg dose) ( Figure 1 , Top left). Because of the limited number of samples per cohort, a dose correlation was not performed; however, based on the median values, a trend was observed: cohort 1 (14 nM) < cohort 2 (106 nM) < cohort 3 (555 nM). These aqueous levels are about 1000-fold to 100 000-fold above the affinity of MP0112 to VEGF (about 2 pM; data on file, Molecular Partners) or the potency of MP0112 to inhibit VEGF in a spheroid sprouting assay (about 17 pM; data on file, Molecular Partners). Data from the 4 cohort 3 patients were used to determine ocular pharmacokinetic parameters. Maximal observed aqueous MP0112 concentrations after a single intravitreous injection of 0.4 mg ranged from 230 to 622 nM with a median concentration of 555 nM (19 μg/mL) at week 1 ( Figure 1 , Top right). Four weeks after injection, aqueous MP0112 concentrations ranged from 41 to 89 nM with a median of 60 nM (2 μg/mL), and 12 weeks after injection, levels were still detectable in all 4 patients, with a median of 10 nM. These data suggest an ocular half-life ≥13 days. None of the patients had measurable serum levels of MP0112 at 1, 3, 7, or 28 days after a single intraocular injection of 0.04, 0.15, or 0.4 mg; all samples were below the lower limit of quantification of 0.3 nM.
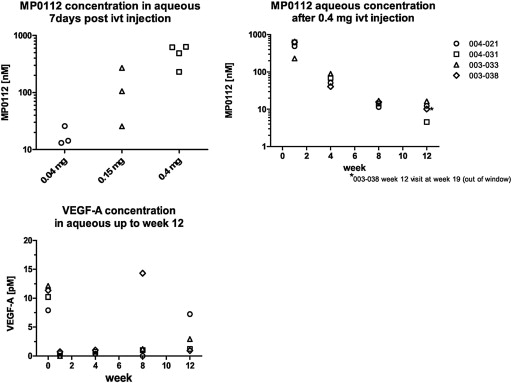
Baseline aqueous humor VEGF-A levels ranged from 7.5 to 12.5 pM in the 4 cohort 3 patients that had measurements ( Figure 1 , Bottom left). Aqueous humor levels of VEGF-A were below the limit of detection in the 4 cohort 3 patients at weeks 1 and 4, and in 3 of 4 patients at week 8. Patient 003-038 had a high level of VEGF-A at week 8 and a low level at week 12, which could represent a transient rebound effect at week 8 or a spurious measurement. At week 12, all 4 patients continued to have VEGF-A levels below baseline, with 3 of 4 <5 pM.
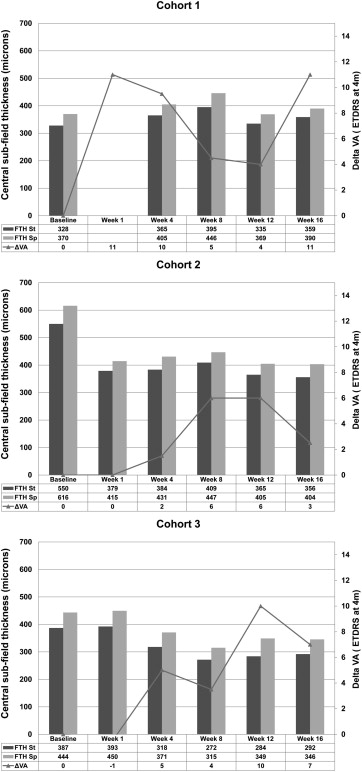
Biologic Activity of MP0112
Visual acuity was assessed at all visits. No patients received rescue therapy. Some patients in cohort 1 showed an improvement in BCVA after injection and the median improvement at week 1 was 11 letters ( Figure 2 , Top). At week 4, the median improvement in BCVA was 10 letters, but there was no decrease from baseline in mean central subfield thickness. The median BCVA decreased between weeks 4 and 12 and then increased somewhat at week 16. One patient in cohort 1 experienced a reduction in BCVA between week 4 and week 8 and exited the trial to receive alternative treatment. There was no overall change in median central subfield thickness.