(1)
St. Johns, FL, USA
(2)
Helen Keller Foundation for Research and Education, International Society of Ocular Trauma, Birmingham, AL, USA
(3)
Consultant and Vitreoretinal Surgeon, Milos Eye Hospital, Belgrade, Serbia
(4)
Consultant and Vitreoretinal Surgeon, Zagórskiego Eye Hospital, Cracow, Poland
Trauma is the most exciting and challenging subspecialty in ophthalmology. Much of it is (and should be) handled by the VR surgeon1 because of the expertise needed; vitrectomy instrumentation may be necessary in many conditions. Only a selected few topics are detailed in this chapter; hyphema is discussed in Chap. 47, the iris in Sect. 39.2 and Chap. 48, the lens below (see Sect. 63.6) and in Chaps. 38 and 44, suprachoroidal hemorrhage in Chap. 60, VH in Chap. 62, RD in Chaps. 54 and 55, subretinal hemorrhage in Chap. 36, PVR in Chap. 53, and endophthalmitis in Chap. 45.
63.1 The Timing of Surgery
It is a much more complex question than it initially appears. Table 63.1 provides some guidelines based on which the individual surgeon can make a decision for the particular patient.
Table 63.1
The timing of surgery for the injured eye
Variablea | Comment |
|---|---|
Child/elderly patient | In general, the earlier the better |
Endophthalmitis, high risk | Emergency surgery is needed: wound closure and PPV in the same session. With certain organismsb, the time from “no symptom” to a fulminant, retina-destroying infection may be only a few hours |
Endophthalmitis, present | Emergency surgery is needed: wound closure and PPV in the same session |
General anesthesia, availability | If the patient ate or drank in the previous 6 hc, the surgeon should discuss the options with the anesthesiologist. If the anesthesiologist, for whatever reason, will not be able use general anesthesia and the surgery is otherwise urgent, some type of local anesthesia (see Chap. 15) should be used. The surgeon himself should administer the periocular injection |
Hyphema | In adults, the primary factors are whether the retina can be visualized and the IOP can be kept in the normal range. High IOP in the presence of full hyphema is an urgent indication; the surgeon should err on the side of early intervention |
Hypotony | Early removal of vitreous, fibrin, and any capsular remnantd from the surface of the ciliary body can prevent scarring, which in turn is irreversible |
IOFB | Some of the mechanical damage has already been done, but there is an immediate risk of infection (and chalcosis if the object is copper), further mechanical injury due to the body’s scar-producing reaction, as well as the longer-term threat of chemical trauma (siderosis) |
IOL implantation | In a child of the amblyopic age, this can be urgent (in those under 2 years, a contact lens may be a better optione). In virtually all other cases, deferral of the implantation may be preferable |
Iris, retraction (“missing iris”) | The sooner the better. Once the fibrinous membrane turns into a scar tissue, the condition becomes irreversible |
Lens, damage to either capsules | In adults, there is no urgency In children, the lens may swell in hours, leading to pupillary block glaucoma with extremely high IOP: urgent lens removal is needed |
Lens, cataract | In adults, the primary factor is whether the retina can be visualized; otherwise there is no urgency In children, amblyopia is the key factor: the younger the child, the more urgent the visual rehabilitation is |
Perforating injury | Immediate or early surgery is needed to prevent PVR and retinal incarceration |
PVR | Early surgery is recommended if the macula is involved or threatened; otherwise it may be preferable to delay the PPV until the PVR cycle is complete |
RD | PPV is urgent but not necessarily an emergency |
Rupture | Especially if the wound is posterior to the muscle insertions, immediate or early surgery is needed to prevent PVR and retinal incarceration |
Subretinal hemorrhage | Usually, no action is needed unless the blood is under the macula. If it is, removal or at least displacement should be done as soon as possible |
Suprachoroidal hemorrhage | If it occurs intraoperatively, the wound/s must be closed immediately and the IOP raised. Otherwise, surgery is urgent only if a kissing choroidal is present, the blood is underneath the macula, or an RD accompanies the bleeding |
Surgery, secondary (reconstructive) | In general, the earlier the better; if the infrastructuref is in place and the surgeon is aware of the possibility and handling of ECH, comprehensive primary reconstruction may be performed. If the traditional staged (2-step) approach is chosen, it is best to apply heavy topical steroid therapy and perform the PPV within 4 days |
Systemic condition of the patient | Hypertension and agitation in patientsg with open-globe injury make the surgery more urgent Anxious patients should be operated earlier, but this is not an absolute requirement (antianxiety medications may be needed if the surgery is delayed). Proper counseling may have a calming effect |
VH, contusion | There is no urgency to remove the blood, but leaving it in the eye for an extended period is unjustifiable today (see the text for more details) |
VH, open-globe injury | The sooner the blood is removed, the better. The blood not only prevents visualization of the retina but is a strong inciting factor in PVR development |
Wound, corneal | Close it as soon as possible, although it may be acceptable to postpone it from the middle of the night till the morning hoursh if the wound is small and the proper infrastructure (see above) is not unavailable The longer the wound, the more urgent the need for early closure |
Wound, scleral | The longer the wound, the more urgent the need for early closure The more anterior the wound, the more urgent the need for early closure |
63.2 Contusion
The most common acute complication of this closed globe injury is VH. Traditionally, a 3-month waiting period has been recommended before vitrectomy would be considered.
Q&A
Q
What is the rationale for waiting 3 months to remove a contusion-related VH?
A
There is none. The 3-month period has no scientific basis at all, and the blood may represent more risk than its removal (see Chap. 62).
About half of the eyes with a severe contusion will develop RD in the first 2 years. Surgery is able to restore the patient’s vision instantly and allow the surgeon to treat and/or prevent most retinal complications.
Additional, rather common, complications include lens dislocation (see Sect. 44.2.1) and a macular hole (see Sect. 50.2.4).
Pearl
Surgery for a traumatic macular hole is often delayed because there have been reports of spontaneous closure. This is certainly true, but the surgeon has to consider two opposing options. On one hand, spontaneous closure indeed occurs – but it is impossible to predict what the likelihood in that particular patient is. On the other hand, the sooner the hole is closed, the greater the chance of excellent recovery – but surgery is obviously not risk-free.
Finally, the vitreous may prolapse into the AC, even if the lens is only mildly subluxated. It is extremely rare that the prolapse causes glaucoma or endothelial damage, but the presence of vitreous in the AC changes the surgical technique of lens removal (see below).
63.3 Wound Toilette
As a general rule, the wound should not be sutured until all debris and tissue that have prolapsed into (through) the wound edges have been cleaned.2 The technique of dealing with the material found in the wound depends on the material’s nature (see Table 63.2).
Table 63.2
Wound toilette
Material in the wounda | Surgical to-do |
|---|---|
Blood, fibrin, foreign material | Mechanical cleaning with a Wechsel sponge, antibiotic jet spray, occasionally forceps |
Choroid | Do not excise it; if it bulgesb, gentle diathermy will shrink it sufficiently |
Iris | Pull the iris back into the AC through a paracentesis (see Sect. 39.2). The iris almost always can be saved; excision is restricted to cases when the iris is severely macerated or soiled to the point that it cannot be cleaned |
Retina | Try to prevent it from prolapsing; if it did prolapse, try to keep it back with a blunt instrument, held by the assistant, while you are suturing. Address the incarceration from the inside as soon as possible (see below) |
Vitreous | External prolapse: Do not use a Wechsel sponge because it may cause traction on the anterior vitreous; the probe is the ideal instrument to deal with the prolapse. If a Wechsel sponge must be used, at least do not lift it up from the eye surface; keep it dipped into the vitreous and use the scissors to first push down on the eyewall and then cut the vitreous Internal prolapse: Inject TA to identify the vitreous in the AC. If the eye is phakic, use a paracentesis for probe entry; in the aphakic eye, the pars plana approach is preferable since it gives better access to the vitreous. In the pseudophakic eye an individual decision must be made. If the eye is phakic, it may be impossible to completely remove the vitreous; at least sever the connection between the remaining prolapsed vitreous and the gel proper |
63.4 Suturing the Cornea3
There are basic rules that should be followed so as to minimize the additional trauma to the cornea and therefore reduce the edema in the early, and astigmatism in the late, postoperative period. The creation of a watertight wound is the minimum necessary goal of the surgery, but it is only one of the mandatory goals. The suture placement must be carefully planned; random suture introduction is unacceptable (see Fig. 63.1).
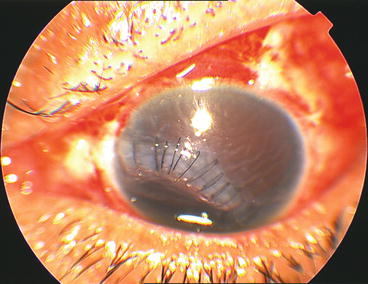
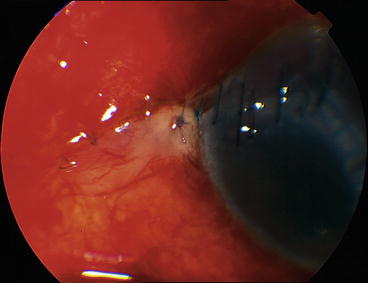
Fig. 63.1
Poorly sutured corneal wound. The suture bites are of more or less equal length and their spacing is haphazard. The healing will be poor and take a long time. TKP-PPV (possibly EAV, even though a PK will most probably be needed anyway) is unavoidable since the posterior segment surgery cannot be delayed indefinitely
Fig. 63.2
The advantages of the full-thickness corneal suture. (a) The typical recommendation is for a suture to be “90%” (80%, 2/3 etc.) deep. The problem with any of these suggestions is that the back of the wound remains open for a while, providing aqueous access to the stroma (arrow). Furthermore, the 2 edges of the wound, which are already edematous, are of different thickness, due to the different amount of edema: a suture that is of 80% deep on one side may be only 70% deep on the other side. This results in a permanent distortion (the effect does not disappear upon suture removal). (b) With a full-thickness suture, the posterior “door” is instantly closed, and the stroma rapidly dries. The suture is 100% deep, irrespective of the difference in the thickness of the 2 wound edges
Fig. 63.3
Sequence of suture-introduction for a transcorneal wound. (a–d) The wound is limbus to limbus. The suturing commences from the 2 endpoints at the limbus and gradually approaches the center of the wound with ever-shorter bites. (e) There is no suture at the epicenter of the wound since it wound interfere with the visual axis
Fig. 63.4
Suturing and resuturing a corneal wound. (a) The long wound was originally closed with a running suture. The result is an AC with significantly reduced depth; in addition, the eye is inflamed since the knots are not buried. (b) Resuturing was necessary. Note how few (full-thickness) sutures, all with long bites, were sufficient to make the wound watertight, without the risk of shallowing the AC. During the original surgery, the cornea was too edematous to allow safe removal of the traumatic cataract (seen on a). Conversely, once the wound was resutured, both the cataract removal and the vitrectomy could be completed. (c) An extremely poorly sutured wound. Because the initial closure was done 10 days earlier and the eye needed urgent vitrectomy, a TKP had to be used. To trephine the cornea, however, the still-leaking wound had to be partially resutured, using 5 10-0 nylon sutures (thick arrows)
Fig. 63.5
Unburied suture knot at the limbus. Leaving the knot and the trimmed suture endings unburied results in major irritation to the patient and increases the eye’s inflammatory reaction as well as the risk of corneal vascularization
The fundamental rules and goals are summarized in Table 63.3.
Table 63.3
The basics in corneal wound closure
Variable | Rule | Comment |
|---|---|---|
Timing | As early as possible | Delaying the wound closure is a crucially important risk factor in endophthalmitis development. Still, in certain casesa it may be acceptable, after proper counseling, to delay the closure for a few hoursb |
Making the wound watertight | Absolutely yes | A leaking wound has difficulty healing, and there is an increased endophthalmitis risk |
Excision of loose fragments | Never | The suture must be placed so that the fragment is preserved; otherwise either a gap will be present or the suture needs to be overtightened to close it |
Type of suture material
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|