Transposition Procedures
David A. Plager
Daniel E. Neely
Kathryn M. Haider
Muscle Transpositions
General Indications
A muscle transposition procedure may be indicated when the function of one or more of the rectus muscles is absent or severely deficient as a result of third or sixth cranial nerve palsy, lost muscle, type I Duane syndrome, supranuclear defects, monocular elevation deficiency (double elevator palsy), or in the rare case of congenital absence of one or more extraocular muscles.
Background
Hummelsheim is credited with describing the first rectus muscle transposition procedure for treatment of paralytic strabismus in 1908.1 His procedure for treating the esodeviation that results from sixth nerve palsy involved splitting the vertical recti and reattaching the temporal halves of each vertical rectus muscle adjacent to the insertion of the lateral rectus muscle. Several modifications to this procedure have been described, including those of O’Connor (1921),2 Berens and Girard (1950),3 Wiener and Scheie (1952),4 Hildreth (1953),5 Costenbader (1958),6 Schillinger (1959),7 Jensen (1964),8 Uribe (1968),9 and Knapp (1969).10 These modifications were reviewed by Helveston in 1971.11 More recent alternatives have been suggested by Carlson and Jampolsky (1979),12 Kushner (1979),13 Rosenbaum et al. (1989),14 and Foster (1997).15 Even with these modifications, the original principle remains the same. All extraocular muscle transpositions that involve the rectus muscles shift forces of antagonist muscles to a rectus muscle that lies between them and acts in the opposite plane. For example, vertical recti are transposed nasally or temporally to enhance horizontal function, and horizontal recti are transposed superiorly or inferiorly to enhance vertical function. In this manner, a surgeon is able to alter both active contractile and passive elastic force vectors to augment the action of a deficient rectus muscle, improving alignment, ductions, and anomalous head postures while expanding the field of single binocular vision.
The most widely used procedures for rectus muscle transposition are the full-tendon transfer combined with either chemodenervation or recession of the antagonist of the paretic muscle, the Hummelsheim procedure, and the Jensen procedure. The most common indication for muscle transposition is lateral rectus weakness secondary to acquired sixth nerve palsy. Transposition is indicated less often for superior rectus weakness as occurs in double-elevator palsy, or lateral rectus dysfunction associated with esotropic Duane syndrome,16,17,18,19 and is least often utilized for inferior rectus palsy. Transpositions are necessary when a rectus muscle has lost attachment to the globe and cannot be found and reattached. This occurrence most commonly is a complication of medial rectus surgery. Superior oblique transposition can be used for medial rectus paralysis when the vertical recti also are compromised, an occurrence most often associated with third nerve palsy. Techniques for this procedure have been described by Jackson20 and also by Scott.21
Contraindications
Restriction
Muscle transposition alone is not effective when free movement of the eye is restricted. Some mild restriction, or stiffness, of the antagonist of a paretic muscle invariably occurs after several months. This restriction is due to the effects of the chronic contracture of the antagonist of the paretic muscle. In most cases, it can be relieved by recessing the muscle or treating it with botulinum toxin. When restricted movement is caused by abnormal attachments of the orbital fascia to other orbital fascia or to the globe, the attachments must be freed by surgery before an extraocular muscle transposition is performed if the best result from this surgery is to be obtained.
Vascular Insufficiency
This surgery is relatively contraindicated in older patients who have significant vascular disease because these individuals have an increased risk of developing anterior segment ischemia after surgery. This topic is covered more fully in the section that discusses complications.
Surgical Techniques
Full-Tendon Transfer
Our preferred technique for muscle transposition is a full-tendon transfer. Any two antagonist rectus muscles can be used for the transfer, but the most common method involves transposing the vertical recti temporally to treat lateral rectus palsy. This procedure can be performed through two fornix incisions, for example, superotemporal and inferotemporal, or through a large, 240 degrees limbal peritomy, such as from the 5:00 o’clock position clockwise around to the 1:00 o’clock position in the right eye.
The superior rectus muscle is located, engaged on a muscle hook, and dissected free of the overlying anterior Tenon’s capsule and the intermuscular membrane at least 10 mm posteriorly. Attachments to the underlying superior oblique muscle also are divided. The muscle insertion is secured with a double-armed 6-0 absorbable suture (Vicryl, Ethicon, Somerville, NJ; Biosorb, Alcon, Ft. Worth, TX) and disinserted from the globe. The inferior rectus muscle is exposed, secured, and disinserted in a similar fashion. Thorough dissection of the inferior rectus muscle from attachments to Lockwood’s ligament is necessary to minimize lid fissure changes postoperatively.
The superior and inferior rectus muscles are then reattached to the globe in juxtaposition to the lateral rectus insertion. We prefer to suture the vertical recti so that the temporal corner of the transposed muscle abuts the adjacent corner of the lateral rectus insertion. The nasal corner of the transposed muscle is attached so that the new insertion of this muscle coincides with the spiral of Tillaux (Fig. 1).
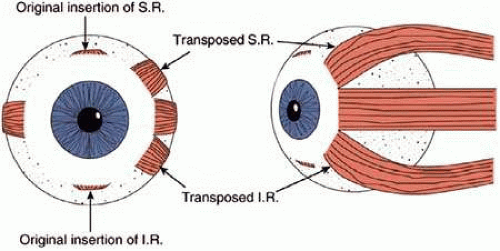 Figure 1. Full-tendon transposition of the rectus muscle. |
The antagonist muscle, in this case the medial rectus, often must be weakened. Our preferred method is by chemodenervation with botulinum A toxin. This method, when successful, obviates the need for recession of a third rectus muscle. A single injection of up to 5 units of botulinum may be given at the time of surgery with the site of injection in the muscle belly under direct observation. As an alternative, botulinum may be given before or after the transposition procedure with or without the aid of electromyographic localization.
Some surgeons believe that there is an advantage to pretreating the restricted antagonist with botulinum several days before the transposition so that the drug will have a chance to initiate relaxation of the antagonist muscle before the transposition and thereby enhance the effect of surgery. Usually, we inject the antagonist at the time of the transposition; it also can be effective if given after surgery. An initial overcorrection after muscle transposition with botulinum injection is desirable. This overcorrection resolves in several weeks as the effect of the botulinum diminishes. A potential side effect of botulinum treatment is ptosis from diffusion of the botulinum into the levator, which can persist for several weeks or months, but usually resolves. If the surgeon chooses not to use botulinum, or if restriction persists in spite of treatment with botulinum, then recession of the antagonist muscle is indicated. In the case of a lateral rectus palsy, a recession of the ipsilateral medial rectus muscle, either with or without an adjustable suture would be performed.
Normally transposed rectus muscle bellies are known to approach their new insertion at an angle approximating 45 degrees.22 This produces a significant gap between the borders of the paretic muscle and the two transposed rectus muscles (Fig. 1). Magnetic resonance imaging studies confirm that, despite significant displacement of the anterior insertion sites, transposition procedures produce relatively small changes in more posterior portions of the rectus muscle. Following vertical rectus muscle transposition to the lateral rectus, the path of the muscle belly posterior to the equator has been found to shift 3 mm or less.23
In 1997, Foster described a modification of the traditional full-tendon transfer15 which involves vertical muscle transposition augmented with a lateral fixation suture (Fig. 2). The goal of the Foster procedure is to close the gap between the transposed rectus muscles and the nondisplaced paretic muscle, thereby enhancing the desired force vectors of the transposed muscles (Fig. 3). For a lateral rectus palsy, a full-tendon transfer is performed as described previously, with the addition of a 5-0 nonabsorbable, polyester fiber suture placed through the sclera adjacent to the border of the lateral rectus. This suture is placed 16 mm posterior to the limbus, or approximately 8 mm posterior to the insertion of the lateral rectus, and separate sutures are placed along the upper and lower borders of the muscle. Once anchored in the sclera, the sutures are then passed through the adjacent transposed vertical rectus, incorporating 25% of its width. When the suture is pulled tight and tied, the gap between the muscles is closed as the borders are drawn into approximation and securely fixed at the equator.
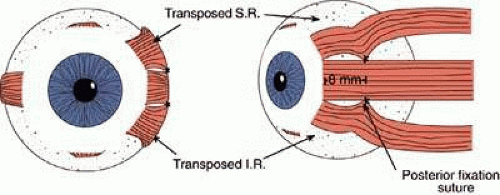 Figure 2. Foster modification of the full tendon transfer procedure. |
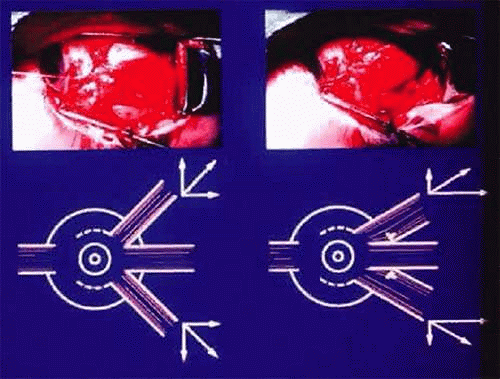 Figure 3. Effect of augmented transposition on the force vectors produced. (Foster RS: Vertical muscle transposition augmented with lateral fixation. J AAPOS 1:20, 1997). |
Lateral fixation suture augmentation has been shown to significantly increase the tonic force of the transposed vertical muscles in cases of sixth nerve palsy, type I Duane syndrome, and partial third nerve palsy.15,19,24,25,26,27 MRI scans by Clark and colleges have documented an increase in the displacement of the muscle belly from 3 mm to approximately 5 mm on average.28 This creates a greater force in the direction of the paretic muscle and enhances the transposition effect. This augmentation may result in a more satisfactory alignment, improved ductions and a larger diplopia-free visual field without requiring surgery on a third rectus muscle (Fig. 4).
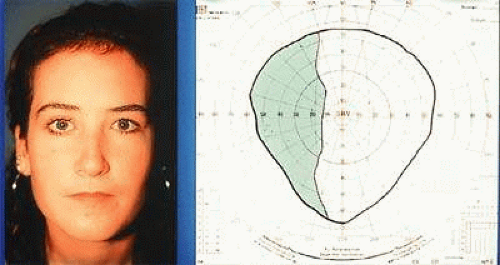 Figure 4. Diplopia-free visual field of patient with type I Duane syndrome after undergoing left augmented transposition. (Foster RS: Vertical muscle transposition augmented with lateral fixation. J AAPOS 1:20, 1997). |
The Hummelsheim Procedure
The technique for the Hummelsheim procedure is similar to that described previously for the full-tendon transfer, except that the muscle is divided along its long axis, and only half of the muscle is transposed. The other half remains attached to the globe with some vasculature presumably intact. This procedure is indicated for cases in which preservation of anterior segment circulation is a special concern.
Once the vertical recti have been identified, engaged on a muscle hook, and freed of surrounding attachments to intermuscular membrane and anterior Tenon’s capsule, a small muscle hook is used to split the muscle and tendon, beginning at the insertion and extending approximately 15 mm posteriorly. The anterior ciliary arteries should be identified and the splitting done between the vessels, leaving intact the vessel in the half of the muscle that was not detached. The half of the muscle to be transposed is secured on a double-armed, absorbable 6-0 suture and disinserted. The same splitting procedure is performed on the direct antagonist. In a fashion similar to the full-tendon transfer, the halves of the two muscles are then secured to the sclera, concentric with the limbus, at the edges of the insertion of the palsied or lost muscle (Fig. 5) and the ipsilateral antagonist to the lost or palsied muscle should be weakened by chemodenervation or surgical recession.
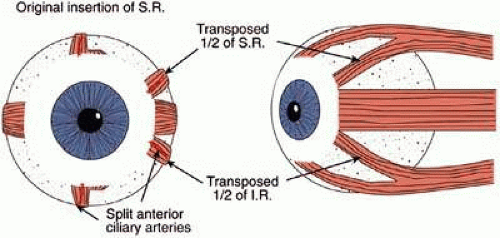 Figure 5. The Hummelsheim procedure. |
The Jensen Procedure
The Jensen procedure is performed by splitting the palsied muscle and joining the midportion of this muscle to the similarly split midportions of the two adjacent rectus muscles. The dissection and splitting are performed as described for the Hummelsheim procedure, but the muscles are not disinserted. Instead, a 5-0 nonabsorbable polyester fiber suture is used to join the muscle bellies to affect a union of the two muscles just anterior to the equator (Fig. 6).
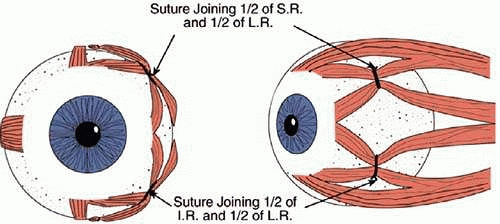 Figure 6. The Jensen procedure.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|