Transpalatal Access for Nasopharyngectomy
Alexander C. Vlantis
INTRODUCTION
A nasopharyngectomy is the surgical excision of the mucosa and adjacent soft tissues of the nasopharynx usually performed for surgical salvage of residual or recurrent nasopharyngeal carcinoma following primary radiotherapy. It can be done as (i) an endoscopic procedure; (ii) a minimally invasive procedure with or without the use of an endoscope, surgical navigation, and/or a surgical robot; or (iii) an open procedure. Open procedures use wide access to the surgical field for adequate visualization and protection of vital structures during tumor resection and are named according to the approach taken to the nasopharynx as anterior (transnasal), anterolateral (transmaxillary), lateral (infratemporal fossa), or inferior (transpalatal).
HISTORY
These patients have a history of nasopharyngeal carcinoma (NPC) treated with radiotherapy with or without chemotherapy. Symptoms suggestive of a residual or recurrent cancer include nasal obstruction, blood-stained nasal discharge, epistaxis, blood-stained saliva, hearing loss, and a mass in the neck. The patient may volunteer these symptoms at routine follow-up visits or present because of them.
PHYSICAL EXAMINATION
The nasopharynx is examined at each planned routine follow-up visit and at any other time when symptoms or investigations such as imaging or serology dictate. Any suspicious lesions seen are biopsied transnasally under topical anesthesia with the endoscope used to direct biopsy forceps to the lesion. Occasionally, a general anesthetic is needed if the lesion is deeper and is less accessible or an awake biopsy is contraindicated.
INDICATIONS
The surgical salvage of residual or recurrent rT1 or early rT2 NPC where the tumor does not abut the internal carotid artery (ICA) and hence clear margins of resection can be anticipated. Surgery avoids the significant morbidity and remote chance of cure associated with a second course of external beam radiotherapy.
CONTRAINDICATIONS
Residual or recurrent NPC abutting the ICA makes safe and complete resection unlikely. Involvement of the bone of the base of the skull (rT3), intracranial or cranial nerve involvement (rT4), or distant metastases (M1) are also contraindications.
PREOPERATIVE PLANNING
Following histologic confirmation of residual or recurrent cancer, an MRI with contrast is mandatory to delineate the extent of the cancer and to define its relationship to surrounding structures, especially the internal carotid arteries. The presence and position of any ectatic portion of the ICA must be noted.
A PET-CT is useful to exclude regional and systemic disease.
SURGICAL TECHNIQUE
Tracheostomy
A tracheostomy is done under local anesthesia in an awake patient or under general anesthesia after intubation.
Mandibulotomy and Mandible Swing in Patients with Trismus
In patients with significant trismus, a mandibulotomy and mandible swing is done to gain access to the palate for the transpalatal procedure.
Transpalatal Access
Lateral Transpalatal Access
The lateral transpalatal approach is used for unilateral lesions involving the posterior and/or lateral wall of the nasopharynx that do not extend into the contralateral pharyngeal recess. This approach is also suitable for unilateral cancers that extend to the inferior nasopharynx or superior oropharynx.
Palatal Incisions
Soft palate incision: The soft palate is divided from its junction with the lateral pharyngeal wall on the side of the cancer. A finger or instrument placed behind the soft palate to tense it enables the correct position of the lateral incision on the oral surface of the soft palate to be made with a scalpel. The incision is made to meet the free edge of the posterior tonsil pillar/palatopharyngeal fold at 90 degrees. The wound is deepened until the nasopharyngeal soft palate mucosa is reached at which time it is incised with a scalpel at the junction of the soft palate and lateral pharyngeal wall.
Hard palate incision: The hard palate mucosal incision is marked to follow the curve of the gingiva and extends from the midline anteriorly to the medial aspect of the ipsilateral maxillary tuberosity posteriorly and then to join the soft palate incision (Figs. 33.1 and 33.2). The incision is made with a scalpel and carried through the periosteum to bone.
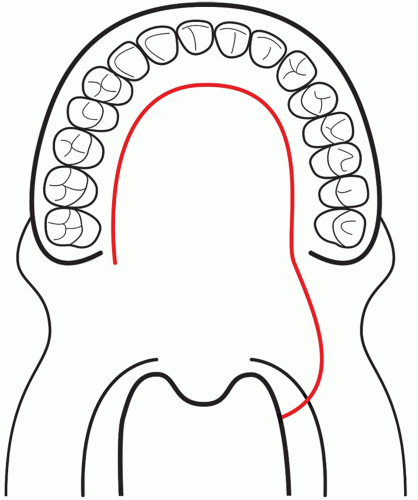 FIGURE 33.1 Hard and soft palate incision for lateral transpalatal access to the nasopharynx. |
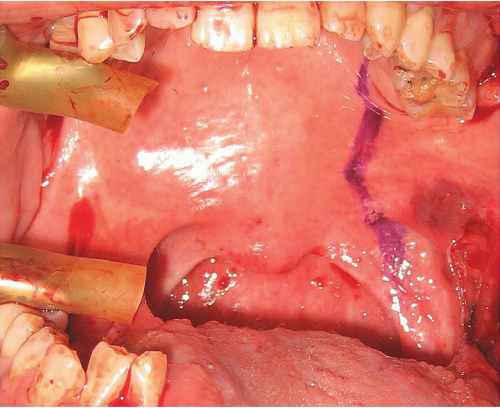 FIGURE 33.2 Hard and soft palate incision marked for lateral transpalatal access. |
Palatal Flap
A mucoperiosteal flap based on the contralateral palatine vascular pedicle is elevated in a subperiosteal plane off the underlying bone. The contents of the ipsilateral palatine foramina are ligated and divided. The flap is elevated across the midline while preserving the contents of the incisive canal and the contralateral palatine vascular pedicle. The nasopalatine nerve is preserved as it exits from the incisive foramen in the anterior midline to preserve sensation in the anterior palate. If greater exposure is needed, the anterior hard palate incision can be extended to the contralateral side and the nasopalatine nerve divided as further hard palate mucoperiosteum is elevated. As the palatal flap is elevated, the palatine aponeurosis and inferior choanal mucosa are divided along the posterior free edge of the palatine bone. The palatal flap is retracted in an appropriate manner.
Median Transpalatal Access
The median transpalatal approach can be used for midline lesions involving the posterior wall or roof of the nasopharynx that do not extend into the lateral pharyngeal recesses on either side. This approach is also suitable for midline tumors that extend to the inferior aspect of the nasopharynx or the superior aspect of the oropharynx.
Palatal Incision
Midline palatal incision: A midline incision is marked from the incisive foramen anteriorly to the uvula posteriorly keeping the integrity of the inferior free edge of the soft palate intact. If more exposure is eventually needed, the uvula can be divided in the midline so as to divide the soft palate completely (Figs. 33.3 and 33.4).
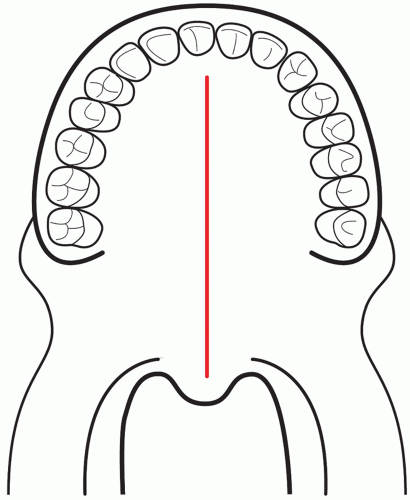 FIGURE 33.3 Midline palatal incision for median transpalatal access to the nasopharynx. |
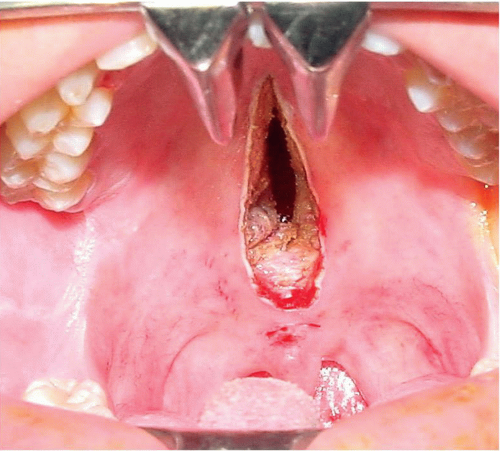 FIGURE 33.4 Midline soft and hard palate incision. |
U-shaped palatal incision: A U-shaped incision in the mucosa of the hard palate is marked to follow the curve of the gingiva from the ipsilateral third molar to the contralateral third molar. The incisions are placed anterior to the palatine foramina bilaterally to preserve the palatine vascular pedicles (Fig. 33.5).
Palatal Flap
Midline palatal incision with laterally based flaps




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
