Extracapsular Dissection of Parotid Tumors
Heinrich Iro
INTRODUCTION
The majority of tumors of the parotid gland are benign neoplasms with the pleomorphic adenoma, the most frequently encountered histologic type followed by Warthin tumor and then other less-frequent entities. The treatment of choice for these tumors is complete surgical removal. Besides the prospect of slow but constant tumor growth, two specifics have additionally to be taken into account in the case of the pleomorphic adenoma: the risk of malignant degeneration into a carcinoma ex pleomorphic adenoma with a reported frequency between 3% and 15% and the rare phenomenon of dissemination by developing benign distant (e.g., pulmonary) metastases documented by a number of case reports in the literature in recent years.
Therefore, the complete removal of the tumor to prevent recurrence as the objective of surgical treatment is without disagreement. However, the required scope of surgical resection has been the subject of controversy during the last several decades: proponents of the standardized surgical techniques of superficial and total parotidectomy base their arguments mainly on a supposedly raised level of recurrence after less-invasive resection procedures. Those who favor extracapsular dissection (ED) and other partial parotidectomies claim a lower rate of postoperative complications for this approach, in particular a lower risk of facial nerve paresis.
The controversy about ED of parotid tumors is understandable in light of the historical development of parotid surgery during the last century. In the first half of the 20th century, benign parotid tumors were often treated by (intracapsular) enucleation, that is, the tumor was exposed, the capsule was intentionally opened, and the contents were shelled out leaving the capsule in situ. The rate of tumor recurrence was high, reaching rates of 20% to 45% in different reports. The relationship of these tumors to the facial nerve was not recognized, so no effort was made to identify it. This led to a high association of the removal of parotid tumor with facial paralysis. Over the following decades, the technique of parotidectomy became refined, in the sense that the tumor was removed in toto with surrounding glandular tissue and that the facial nerve was fully dissected and preserved. Since the 1950s, the consistent use of either a superficial or a total parotidectomy led to a dramatic reduction in the recurrence of pleomorphic adenomas resulting in numerous reports with recurrence rates of 0% to 5%.
However, the dissection of the facial nerve and its branches together with the removal of large parts of the parotid gland can lead to significant postoperative complications. The rates of temporary and permanent facial nerve paresis are reported to be 15% to 25% and 5% to 8%, respectively, after superficial parotidectomy and as high as 20% to 50% and 5% to 10%, respectively, after total parotidectomy. There is also a risk of developing Frey syndrome, the incidence of which has been reported by some authors to be over 10% after superficial parotidectomy and over 30% after total parotidectomy. Moreover, doing a total parotidectomy will usually result in a visible cosmetic defect.
In view of these complications and the benign nature of the tumors, more conservative techniques have evolved over the past 20 years. These include partial resection of the parotid gland where less than the entire superficial lobe of the gland is removed and the facial nerve is dissected only in part or not
at all. The introduction of more conservative procedures has resulted in markedly lower rates of facial nerve paresis and Frey syndrome. At the same time, the first published long-term observations show no increase in recurrence after circumscribed resections (ED) of this type. Unfortunately, the descriptions of the surgical technique used for partial resection of the parotid gland vary greatly and consequently are confusing.
at all. The introduction of more conservative procedures has resulted in markedly lower rates of facial nerve paresis and Frey syndrome. At the same time, the first published long-term observations show no increase in recurrence after circumscribed resections (ED) of this type. Unfortunately, the descriptions of the surgical technique used for partial resection of the parotid gland vary greatly and consequently are confusing.
Classification of Parotidectomies
As the descriptions of the different surgical techniques of parotidectomy vary greatly in the literature, we propose the consistent use of a five-stage classification system based on the exposure of the main trunk of the facial nerve and the extent of the resection:
1. An extracapsular dissection (ED) is defined as the removal of a tumor from the parotid gland without exposure of the main trunk of the facial nerve.
2. Whenever the main trunk is exposed, the procedure is designated as a partial parotidectomy because parts of the superficial or deep lobe of the gland are left in place.
3. Removal of the entire superficial lobe defines a superficial lobe parotidectomy.
4. Removal of the entire gland is a total parotidectomy.
5. A radical parotidectomy implies resection of the entire parotid, surrounding tissue including the facial nerve or parts of it, which may become necessary in surgery of malignant tumors.
On no account should the term “enucleation” be used nowadays to refer to a partial resection, since this will cause confusion with the historical and obsolete technique of opening and shelling out the tumor. The general lack of acceptance of ED for the treatment of pleomorphic adenomas is sometimes based on the supposedly higher recurrence rates resulting from the inexact differentiation of the different surgical techniques and especially of equation of the historical enucleation and the contemporary ED.
HISTORY
The patient’s history usually suggests a benign neoplasm of the parotid gland in case of a painless swelling of the cheek or the mandibular angle persisting for several months or years showing slow growth and lacking any impairment of function of the facial nerve.
PHYSICAL EXAMINATION
The clinical examination includes a complete examination of the head and neck including endoscopy but focuses on bimanual palpation of the tumor in order to thoroughly appreciate the size, location within the gland, consistency, and mobility. Facial nerve function is assessed in detail and recorded in the patient’s record along with the characteristics of the mass.
INDICATIONS
The surgical technique to be performed in an individual case is defined in a two-stage process: First, the preoperative clinical and sonographic findings suggest a potential approach. For example, patients can be scheduled for ED in case of a single and mobile tumor located superficially within the superficial lobe of the parotid gland. On the contrary, a total parotidectomy should be planned for a lesion lying in the deep lobe of the gland or in case of multifocality. However, the final decision about the surgical procedure and especially about preparation of the main trunk of the facial nerve is always made intraoperatively: a supposedly superficial mobile tumor can turn out to extend deeper into the gland or to be located in close proximity to the facial nerve—preparation of the nerve and performance of a conventional parotidectomy are mandatory in this situation. Thus, the surgeon has to be capable of switching between ED and the different forms of parotidectomies at any time during the operation.
CONTRAINDICATIONS
Any suspicion of malignancy by clinical or sonographic findings is a clear contraindication for ED; the patient has to be scheduled for total parotidectomy and neck dissection in this case. Moreover, if multiple lesions are present within the gland or if the lesion extends into the deep lobe, a parotidectomy will be necessary.
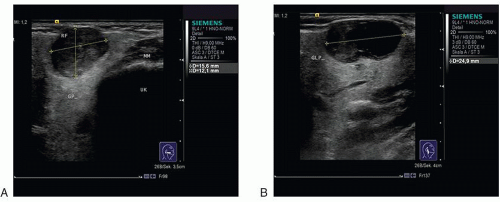 FIGURE 26.1 B-mode sonography of a benign tumor (oncocytoma) located in the inferior part of the right parotid gland in the transverse (A) and longitudinal (B) plane. |
PREOPERATIVE PLANNING
Imaging is indispensable for the preoperative evaluation of tumors of the parotid gland and for further planning. Ultrasound is the imaging modality of choice as it is frequently available without a waiting period and as neither exposure to radiation nor contrast enhancement is necessary. Because of the excellent accessibility of the parotid gland, tumors can be examined in detail sonographically with regard to their shape, echotexture, perfusion, and exact localization within the gland (Fig. 26.1). If ultrasound is not available, additional investigations such as computed tomography (CT) and magnetic resonance imaging (MRI) may be used instead. CT especially is carried out in the case of suspected invasion of the mandible, whereas MRI is the modality of choice to evaluate deep lobe involvement of a tumor. However, tumors scheduled for ED will neither expand into the deep retromandibular part of the parotid gland nor raise any suspicion of bone invasion.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


