Robot-Assisted Neck Dissection Via Modified Face-Lift or Retroauricular Approach
Yoon Woo Koh
INTRODUCTION
Cervical lymph node metastasis is frequently encountered in the management of cancer of the head and neck, and its inappropriate treatment is often associated with treatment failure. Since the establishment of the basis for radical neck dissection by George Washington Crile in the early 20th century, the cultivation of neck dissection techniques has been directed toward the preservation of vital structures and the minimization of neck levels covered by neck dissection (e.g., modified radical neck dissection, functional neck dissection, selective neck dissection, superselective neck dissection, and sentinel lymph node biopsy). Elective neck dissection in the clinically N0 neck is performed not only to remove occult metastatic deposits in the regional lymph nodes at the time of initial treatment but also to provide pathologically proven nodal stage, which helps in determining whether adjuvant therapy is required. With all the efforts to optimize the surgical extent based on the distribution of lymph node metastasis and thereby reduce the surgical morbidity, the scar on the neck after neck dissection has been accepted as unavoidable. However, since disfiguring scars may be a great burden for both surgeons and patients, I sought to develop a surgical technique to hide the scar of neck dissection and recently reported our technique of robot-assisted neck dissection carried out through a modified face-lift or retroauricular approach.
HISTORY
In a situation of a known primary cancer, history taking for identifying nodal metastasis may not be of great importance because imaging studies (e.g., ultrasonography, CT, or MRI) can detect the nodal metastasis more precisely. However, the presence of pain/tenderness and the growth rate of a mass in the neck should be asked to add useful information for determining the necessity of fine needle aspiration biopsy (FNAB), which can confirm the preoperative diagnosis of cancer in the lymph node. History of previous neck surgery or parotid surgery should be sought.
PHYSICAL EXAMINATION
After the evaluation of the primary cancer, palpation of the neck is mandatory especially in the area of primary lymphatic drainage. The location of the mass and its size, fixation to the surrounding structures, consistency, and pulsation should be described. Function of the facial, lingual, vagus, spinal accessory, hypoglossal, and phrenic nerves should be evaluated preoperatively. Any findings indicative of previous neck or parotid surgery should be assessed. The length and circumference of the neck are major determinants of good exposure. Though the patient who has
a long slim neck provides the best exposure, I have accomplished the robot-assisted neck dissection successfully in less favorable situations. Therefore, the somatometry does not provide the absolute contraindication.
a long slim neck provides the best exposure, I have accomplished the robot-assisted neck dissection successfully in less favorable situations. Therefore, the somatometry does not provide the absolute contraindication.
Somatometry means: classification of persons according to body form and relation of types to physiological and psychological characteristics.
INDICATIONS
Indications for robot-assisted neck dissection are: (1) patients who have biopsy-proven cancer of the head and neck, for example, early cancer of the oral cavity that requires an elective neck dissection including levels I, II, and III or early cancers of the oropharynx or hypopharynx that need elective selective neck dissection including levels II and III; (2) patients who have not previously been treated for cancer of the head and neck; (3) patients who have a resectable primary cancer (T1 or T2); and (4) patients who lacked clinically suspicious metastatic neck nodes (cN0). Recently, I extended the indication up to cN1 without suspected extracapsular spread in accordance with the accumulation of experience.
CONTRAINDICATIONS
Contraindications for robot-assisted neck dissection are as follows: (1) patients expressing refusal after the explanation for the advantages and disadvantages of the procedure, (2) patients undergoing chemoradiation for primary treatment due to refusal of surgery, (3) patients in whom the primary cancer had recurred, (4) patients with distant metastasis at the time of initial presentation, (5) patients who were suspected of having extracapsular spread in the cervical lymph nodes, (6) patients who have advanced nodal stage more than N2, (7) patients who have had a cervical skin incision for the removal of primary cancers, or (8) patients who needed free flap reconstruction for a primary surgical defect. Recently, I have begun to gather data in patients in whom robot-assisted neck dissection and free flap reconstruction via modified face-lift or retroauricular approach were performed simultaneously. Therefore, the necessity for free flap reconstruction is a relative contraindication.
PREOPERATIVE PLANNING
Imaging Studies
CT and MRI are the most useful imaging studies and can reveal the size, number, location, and extent of cervical lymph node metastasis. It is especially important to define the extracapsular spread of cervical lymph node metastasis because the oncologic safety of the procedure can be violated due to the spillage of malignant cells during the manipulation of lymphoadipose tissues in robot-assisted neck dissection. PET-CT can also be useful for detecting occult metastasis in cN0 neck and for demonstrating distant metastasis.
Fine-Needle Aspiration Biopsy
To confirm the cervical lymph node metastasis, FNAB should be performed; the sensitivity and specificity of which are over 92% and 94%, respectively, according to the study of Frable. A successful FNAB is dependent on the skills of the radiologist and pathologist. The result of FNAB is one of the prime determinants in selecting the option for treatment of cervical lymph node metastasis.
SURGICAL TECHNIQUE
This technique is indicated for dissection of levels I, II, and III (supraomohyoid neck dissection), which is frequently performed as part of the treatment for cN0 cancer of the oral cavity. It could also be applied to levels II and III dissection for cN0 squamous cell carcinoma of the oropharynx and hypopharynx in the context of superselective neck dissection. The concept of this approach was originally presented by Terris et al. as a modified face-lift incision for parotidectomy in 1989, and the early cases were performed through the same incision. However, I found out that a retroauricular incision without preauricular extension provided enough space for the surgical exposure of levels I, II, and III and now the procedure is conducted entirely through a retroauricular approach. Recently I have accumulated experience with this approach for the endoscopic removal of benign masses in the upper neck including the submandibular gland. However, according to our experience, straight and rigid endoscopic instruments may have limitations in approaching the site of dissection in narrow and angled working space, and the endoscopic view may be hindered by the surrounding tissues or the instruments. In order to obtain sufficient surgical exposure and instrumentation to secure oncologic safety and prevent injury of vital neurovascular structures, I used the robotic surgical system for dissection in combination with conventional technique under direct vision.
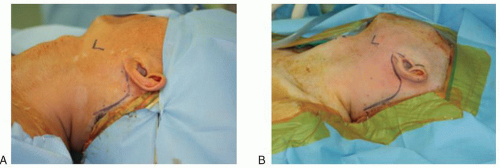 FIGURE 7.1 Skin incision. A: Retroauricular approach. B: Modified face-lift approach. |
Description of Technique
Skin Incision and Flap Elevation
The patient is placed in the supine position under general anesthesia with the neck slightly extended by inserting a soft pillow under the shoulder. The patient’s head is turned to the opposite direction of the primary lesion. The retroauricular incision is made starting from the inferior aspect of the retroauricular sulcus, moved superiorly to the midpoint of the sulcus, and then smoothly angulated downward 0.5 cm inside the hairline (Fig. 7.1A). The modified face-lift incision is extended from the retroauricular incision to the natural preauricular fold and continued behind the tragus (Fig. 7.1B). There have been reports of using a linear hairline incision for retroauricular approach to perform endoscope-assisted submandibular gland resection. However, an incision prolonged to the retroauricular sulcus may relieve the tension of the skin flap compared to that of a linear incision along the hairline only. The skin of the retroauricular sulcus shows more elasticity compared to that of the scalp at the hairline, and extension of incision to this area provides sufficient height (>4 cm) for the entrance to the surgical field. Moreover, instrumentation may be conducted in closer proximity than a linear hairline incision.
The skin flap is elevated along the subplatysmal plane (Fig. 7.2) just above the sternocleidomastoid (SCM) muscle using a monopolar cautery under direct vision and is continued to the midline of the anterior neck and superiorly to the inferior margin of the mandible and inferiorly to the level of the omohyoid muscle. Two assistants put traction on the skin flap using the Army-Navy or right-angle retractors.
Neck Dissection Under Direct Vision via a Modified Face-Lift or Retroauricular Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


