This article presents a comprehensive review of the translabyrinthine surgical approach for vestibular schwannoma. Additionally, it addresses the traditional labyrinthectomy and identifies a time-efficient version. Indications and outcomes of the approach are presented, along with detailed procedural technique from opening incision through closure. Complications and management of complications are discussed in detail, as well as postoperative patient care.
| CPA | Cerebellopontine angle |
| IAC | Internal auditory canal |
| PTA | Pure tone average |
| SDS | Speech discrimination score |
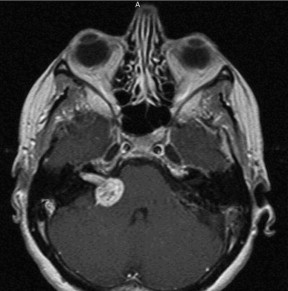
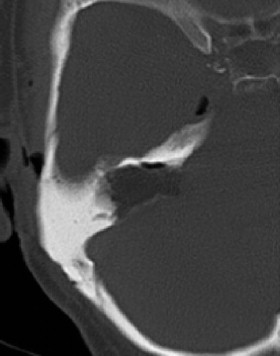
Otologists first described the translabyrinthine craniotomy as an approach to the cerebellopontine angle (CPA) at the beginning of the twentieth century; however, William F. House was the first surgeon to successfully perform the approach with regularity for vestibular schwannoma (VS) removal. Although hearing is sacrificed in its traditional form, the translabyrinthine craniotomy allows the most direct access to the CPA, as well as exposure of the facial nerve from brainstem to stylomastoid foramen ( Figs. 1 and 2 ). All drilling is extradural. The entire length of the internal auditory canal (IAC) from fundus to porus, as well as its connection to the CPA, is routinely exposed.
Indications for translabyrinthine approach for VS
The translabyrinthine approach is used for VS when the hearing is poor or in cases in which hearing preservation would be unlikely. Advantages of the translabyrinthine approach are
- •
It is the most direct route to the CPA
- •
It exposes the IAC in its entirety
- •
The facial nerve can be found with typically undisturbed anatomy anterior to vertical crest (known as the Bill bar) at the fundus.
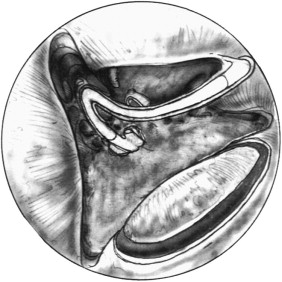
These factors allow for excellent tumor exposure and a reliable potential plane between tumor and facial nerve at the beginning of tumor dissection. The approach can also be used for facial nerve lesions of neoplastic or traumatic causes. The full-length exposure allows for decompression, involved facial nerve resection, translocation, and end-to-end anastomoses or nerve grafting ( Fig. 3 ). The surgeon can extend the dissection through the stylomastoid foramen and into the parotid gland if required.
The translabyrinthine approach can also be used for other tumors in the CPA. These include, but are not limited to, meningiomas, epidermoids, glomus tumors, and choroid plexus papillomas—so long as the determination is made that the potential for hearing preservation or hearing return is outweighed by the direct route of the approach. For tumors that are anterior to the IAC, the approach can be extended through removal of cochlea with or without facial nerve rerouting ( Fig. 4 ). Removal of the cochlea allows better exposure of clival lesions, but requires multilayer closure of the external auditory canal (EAC).

The chosen approach for a given VS is highly variable based on the experience and background of the surgical team members. Tumor size and residual hearing are the most important factors influencing VS approach in centers that routinely use the translabyrinthine, retrosigmoid, and middle fossa craniotomies. Tumors larger than 2.5 cm tend to have poor likelihood of hearing preservation regardless of approach. The translabyrinthine approach is recommended in cases in which the tumor is larger than 2.5 cm and hearing has progressed to a nonserviceable level.
The definition of nonserviceable varies by institution. Some centers adhere to a 50-50 rule in which the hearing is serviceable if the pure tone average is 50 dB or less, and the speech discrimination score is 50% to 100%. Other centers use the 30-70 rule in which hearing is serviceable if the pure tone average is 30 dB or less and the speech discrimination score is 70% to 100%. Use of the nonserviceable hearing cutoff assumes that hearing is not likely to improve after tumor removal. Hearing generally is not expected to improve through VS surgery.
Technique
General Considerations
The translabyrinthine approach is performed under general endotracheal tube anesthesia without long-term muscle relaxation. Cranial nerve monitoring, especially the facial nerve, crucially depends on no paralysis and provides immediate feedback to the surgeon during tumor dissection, aids in facial nerve localization, and provides prognostic facial function information at the end of the case.
After satisfactory anesthesia is induced, the patient receives an orogastric tube, a Foley catheter, recording needle electrodes into the facial musculature, and sequential compression devices to the lower extremities to help prevent deep venous thromboses.
The surgical side is then confirmed with the aid of the patient’s audiogram and MRI films, and a postauricular shave using clippers is performed.
Within 1 hour of skin incision, the patient receives a dose of broad spectrum intravenous antibiotics with good cerebrospinal fluid (CSF) penetration; these antibiotics usually are continued for 24 hours perioperatively.
The operative sites at the ear, scalp, and neck, as well as the fat harvest site in the left, lower quadrant, are then outlined with adhesive drapes. Both areas are prepped and draped with towels and antibiotic-impregnated translucent adhesive drape.
Temporal Bone Exposure
One percent lidocaine with 1:100,000 epinephrine is injected into the postauricular region, extending into the temporal region, and an incision is made 2 to 4 cm behind the postauricular sulcus.
The larger the tumor, the more the retrosigmoid dura needs to be exposed to allow access, and the further posterior an incision is needed.
Simultaneous placement of an osseointegrated abutment for attachment of a hearing appliance is possible. In such cases, the incision is kept more anterior to prevent a soft tissue plane connection between the abutment site and the craniotomy site because this might lead to CSF wound leak through the abutment site, which cannot be water tight. The more anteriorly placed incision does make the posterior aspect of the craniotomy more difficult. Consequently, the authors prefer to place bone-anchored hearing devices at a secondary procedure after complete healing from the tumor resection.
Following a scalp incision, a musculoperiosteal incision is created such that it is staggered and minimizes any overlap with the scalp incision.
The bony EAC is identified with the use of the cautery and elevators.
Care is taken not to macerate the edges of soft tissue because a comprehensive, layered closure is essential to prevent CSF wound leak.
Emissary veins are often encountered with elevation of the pericranium posteriorly. This provides an estimate of the sigmoid sinus location and the bleeding is controlled with bone wax.
Temporalis muscle is harvested from underneath the temporalis fascia and saved for packing of the eustachian tube and middle ear.
Antibiotic is used in the irrigation throughout all stages of the procedure.
The microscope is used throughout the bone dissection, tumor removal, and closure steps.
The traditional arrangement has the operative surgeon positioned on the tumor side of the patient’s head with the stereoscopic binocular microscope and an observer with binocular viewing of half the field on one side and a camera taking images from the opposite side. Modern operative microscopes can be arranged so that two operating surgeons can have simultaneous stereoscopic visualization permitting a “four-handed” technique. By avoiding a “beam splitter” and positioning the binocular eye-pieces at 180° from each other, the cosurgeons can sit opposite each other and truly operate as cosurgeons. Although this is not necessary for all parts of the procedure, the authors have found this strategy facilitates rapid debulking, safe hemostasis, and countertraction during facial nerve dissection. A particular advantage of the technique is that during difficult aspects of tumor dissection, both surgeons have simultaneous access for visualization and palpation of crucial structures as the surgery proceeds and specific steps are completed. This simultaneous access with the four-hand technique is a contrast to the usual side-arm view, which is not stereoscopic for the observer and is not ergonomically positioned for access to the surgical field.
A wide cortical mastoidectomy is performed with saucerization of the edges at least 2 cm superior to the middle fossa floor and posterior to the sigmoid sinus.
The mastoid antrum, lateral semicircular canal, and incus are identified and the bone is thinned over the sigmoid sinus.
Bone is removed from the middle and presigmoid posterior fossa dura. The sigmoid sinus is then decompressed with a bony island of bone (the Bill bar) left over its center to protect it as drilling proceeds medially ( Fig. 5 ).
Bleeding along the sigmoid sinus may be encountered. This is readily controlled using patiently applied gelatin sponge or powder, or oxidized cellulose packing soaked in thrombin.
At this point, the bony EAC is thinned to remove air cells and the facial recess is opened using the incus and lateral semicircular canal as landmarks. It is helpful to identify the descending facial nerve through a thin layer of bone during this portion the procedure. The anterior limit of the more medial dissection is the descending facial nerve. The bone posterior to it can be more aggressively thinned if its location is recognized with certainty.
A labyrinthectomy is then performed and all three ampullae of the semicircular canals are identified leading to the vestibule. The vestibule marks a thin layer of bone that overlies the fundus of the IAC.
Traditional Labyrinthectomy
There are traditional and more time-efficient methods of performing the labyrinthectomy.
The traditional labyrinthectomy opens the semicircular canals methodically, beginning with the superior half of the lateral semicircular canal anterior to posterior.
The inferior half of the lateral semicircular canal provides a bony barrier that protects the mastoid (second) genu of the facial nerve.
The posterior dissection of the lateral semicircular canal leads one to the posterior semicircular canal, which is followed posterior, superiorly, and medially to the common crus.
The common crus is traced medially and anteriorly to the vestibule and then followed along the course of the superior semicircular canal, which proceeds superiorly, anteriorly, and laterally.
Bleeding from the subarcuate artery is often encountered while the superior semicircular canal is removed and it may be cauterized with a bipolar, occluded with bone wax, or controlled with a diamond burr.
Following the superior semicircular leads to its own ampulla first and then to the lateral canal ampulla, which lies inferior to that of the superior canal.
The inferior half of the posterior semicircular canal is followed with confidence posterior and sometimes medial to the already identified descending facial nerve to its ampulla.
At this point, the vestibule connecting all three ampullae should be fully exposed ( Fig. 6 ). The labyrinthectomy is performed being mindful of a potential high-riding jugular bulb, which may be encountered while the posterior semicircular canal is followed.
If the bulb is not identified during the labyrinthectomy, drilling is performed inferiorly at the level of the labyrinthectomy.
The bulb marks the inferior-most extent of medial dissection and it should be identified with a layer of bone overlying it.
Time-efficient Labyrinthectomy
The more time-efficient labyrinthectomy is begun along the medial-most aspect of the sinodural angle.
Bone removal begins here and continues with circular motion of the drill to remove all bone superiorly and posteriorly to the medial middle and posterior fossa dura.
Bony removal proceeds anteriorly to the descending facial nerve and inferiorly to the jugular bulb.
Care is taken to readily identify and preserve the vestibule connecting the three ampullae because these serve as landmarks for the fundus of the IAC and location of the Bill bar.
Steps Following Labyrinthectomy
After the labyrinthectomy is completed, the orientation of the IAC must be considered before performing further drilling. From porus to fundus, the IAC points parallel to the orientation of the EAC. There is typically a great deal of bone still overlying the porus.
Bony removal proceeds posteriorly along the posterior fossa dura down to the level of the porus of the IAC, which may be identified through bone by its darker color.
Bony removal continues laterally following the IAC’s “blue line” up to the area of the vestibule.
At this point, the inferior trough is created between the inferior IAC and the identified jugular bulb.
Bone removal first occurs around the porus inferiorly and continues laterally, ideally drilling away bone such that the trough is flush with the anterior face of the IAC.
The cochlear aqueduct is encountered in this location, parallel and inferior to the IAC, which may lead to CSF leakage.
Drilling is not performed anterior and inferior to the cochlear aqueduct because this places cranial nerves IX, X, and XI at risk.
The superior trough is created in similar fashion with greater care taken laterally because the location of the facial nerve assumes a superior medial position in the lateral IAC.
At this point, the IAC should be uncovered approximately 270°, with the vestibule and bone still overlying the fundus ( Fig. 7 ).
The drilling of the fundus should be done with great care because the landmarks delineating the vestibular and facial nerves are in very close proximity.
The vestibule is further opened with a diamond bur and the superior and inferior vestibular nerves are identified separated by the transverse crest. The superior canal ampulla serves as a landmark for the Bill bar, which lies superior and deep to it.
Using copious, but not visually-obstructive irrigation, the bone superior and medial to the superior vestibular nerve is gently removed until the blue-line of the facial nerve is identified coursing in anterior superior direction, and placed medial to the superior vestibular nerve.
The proximity of the facial nerve is typically announced by a brief burst of the facial nerve monitor at this point.
The triangular section of bone separating the superior vestibular nerve and the facial nerve at the fundus is the transverse crest (Bill bar).
At this point, the wound is copiously irrigated to remove all free bone dust from the incision edges, the retractors, and the craniotomy defect.
Before opening the dura, the eustachian tube is occluded to prevent postoperative CSF leakage through the nose.
First, the incus is removed with a hook and the tensor tympani tendon is cut to improve access to the eustachian tube and to facilitate complete packing of the anterior epitympanum.
The distal end of the eustachian tube is packed with alternating small pieces of oxidized cellulose and temporalis muscle.
The middle ear, facial recess, and antrum are then filled with more temporalis muscle with care not to disrupt the tympanic membrane. A tear in the tympanic membrane will likely result in CSF otorrhea and increase the risk of meningitis.
Opening the IAC
Attention is then turned back to the fundus of the IAC.
Using the Bill bar as the medial landmark, superior, then inferior, vestibular neurectomies are performed using a sharp hook ( Figs. 8 and 9 ). The Bill bar is used to initiate the plane of dissection between the superior vestibular nerve and the facial nerve deep to it.
This plane is followed medially as nerve or tumor dissection proceeds.
Certain identification of the facial nerve in the IAC allows for removal of all its other contents because they serve no more purpose after labyrinthectomy.
Posterior Fossa Tumor Removal
After section of the eighth nerve, the posterior fossa dura is opened sharply.
The incisions should be made widely enough to encompass the tumor’s dimensions, with room to spare.
Blood vessels running along the dura, as well as blood vessels adjacent and deep to the dura, must carefully be avoided.
The posterior fossa dura incision is then carefully continued along the porus and brought onto the IAC over the inferior vestibular nerve.
For smaller tumors that are primarily intracanalicular, the facial nerve is identified both proximal and distal to the tumor with aid of the stimulator.
The plane between the tumor and facial nerve is further developed proximally and the tumor can typically be “shelled out.”
If the plane between the tumor and the facial nerve is less clear, then one errs on the side of caution and removes tumor that is confirmed by appearance, texture, and electromyogram (EMG) stimulation to not be a stretched or distorted facial nerve. Increasingly, a philosophy of tumor management has evolved that emphasizes the reality that a VS is a benign disease process. If there is uncertainty regarding the ability to remove a small portion of tumor without injury to the facial nerve, these scraps of tumor are left behind. Long-term follow-up has shown that these remnants rarely grow, perhaps because they have been devitalized.
Larger tumors will often stretch and distort the facial nerve, creating a difficult plane between tumor and nerve. With such tumors, the most urgent issue that needs to be dealt with is the brainstem compression.
After the posterior fossa dura is opened, the plane between the tumor and brainstem may be developed and preserved with cottonoid pledgets.
By remaining directly on the tumor surface, one may avoid blood vessels in the CPA.
Given the anatomic relationship of the vestibular nerves to the facial nerve, the facial nerve is typically deflected anteriorly by tumor, but rarely may be located superior or inferior.
If the facial nerve is deflected posteriorly, one might question the diagnosis of VS.
After stimulation confirms absence of facial nerve, the posterolateral surface of the capsule is cauterized with the bipolar surface.
The tumor capsule is opened and the tumor is eviscerated with a combination of scissors, an ultrasonic dissector, a mechanical dissector, forceps, suction, and bipolar cautery ( Fig. 10 ). Although direct trauma to the facial nerve may be avoided through this technique, indirect traction injury can still occur with excessive tumor manipulation. By staying within the tumor capsule, one avoids damaging the facial nerve and other neurovascular structures within the CPA.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


