To describe the incidence and the course of complications after the radiosurgical treatment of vestibular schwannomas, the authors reviewed their own experience and reviewed the literature. Failure is described in less than 3% of cases, and this had to be distinguished from transient enlargement of tumor volume. In case of failure, microsurgical resection or another radiosurgical procedure should be discussed. The risk of radio-induced tumorigenesis is not clearly established with single-dose radiosurgical technique. Incidence and management of potential complications should be explained at the time of decision making in the management of vestibular schwannomas.
| AICA | Anteroinferior cerebellar artery |
| CNN | Cranial nerve neuropathies |
| GKRS | Gamma knife radiosurgery |
| RS | Radiosurgery |
| SAH | Subarachnoid hemorrhage |
| VS | Vestibular schwannoma |
After several decades of technical refinements, radiosurgery (RS) is now considered an efficient treatment of vestibular schwannomas (VS), despite the fact that the goal of RS is not the removal of the tumor mass but the avoidance of tumor growth. Today, thousands of patients harboring VS have been treated with this technique all over the world with an excellent tumor control rate in the long-term setting and a reduced number of complications when the treatment is delivered in centers of excellence. However, there are several concerns about possible complications linked to this option that deserve special comments. Based upon the authors’ personal experience and an extensive review of the literature, we report the whole spectrum of the adverse effects of radiosurgery will be highlighted.
Before starting with specific complications, it must be stressed that, basically, complications due to the cranial and dural opening cannot occur. Likewise, complications that are more or less linked to the general anesthesia are not reported, since the procedure is carried on under local anesthesia.
Failure of radiosurgery in vestibular schwannoma
In modern series of radiosurgery, failure is considered as a very unusual event and published in less than 5% of cases ( Table 1 ). Considering that this complication deserves a proactive treatment, there is a need to identify the patterns of tumor growth after RS. These patterns justify a sequential clinical and radiological follow-up after RS, and it is recommended to perform a magnetic resonance imaging (MRI) scan at 6 months, 1 year, and 2, 3, 5, 7, and 9 years after the treatment.
| Center/Author/Reference | Number of Patients | Period of Study | Follow-Up (Months) | Tumor Volume (cc) | Peripheral Dose | Tumor Failure | Permanent Facial Palsy | Permanent Trigeminal Dysfunction | Hearing Loss |
|---|---|---|---|---|---|---|---|---|---|
| Charlottesville/Prasad et al | 153 | 89–99 | 51 | 2.7 | 13.2 Gy | 6% | 1% | 1% | 60% |
| Graz/Unger et al | 192 | 92–98 | 62 | — | 12–14 | 2% | 1% | 1.5% | 38% |
| Sheffield/Rowe et al | 238 | 96–99 | 35 | 3.7 | 14.6 | 8% | 1% | 1.5% | 25% |
| Tilburg Timmer et al | 97 | 03–07 | 21 | 2.7 | 11.1 | — | 8% | 16% | 22% |
| Pittsburg Chopra et al | 216 | 92–00 | 70 | 1.3 | 12–13 | 2% | 0% | 5% (10 years) | 29% |
| Pittsburg/Ogunrinde et al | 31 | 87–92 | 20 | <2 | 16.9 | 6% | 5% | 6% | 50% |
| Marseille/Regis et al | 97 | 92–98 | 48 | — | 12–14 | 3% | 0% | 4% | 30% |
| Bergen/Myrseth et al | 103 | 88–99 | 69 | — | 10–12 | 11% | 5% | — | — |
A transient growth in the year that follows RS is a frequent situation encountered in 15% to 30% of cases. Another situation is an initial growth followed by stabilization at a higher volume in the long term. This scenario is found in 5% to 10% of patients. The knowledge of these 2 patterns has to be known by the patients and referring physician when considering a misleading anticipated decision of treatment. Therefore, a reasonable definition of failure is a continuous growth for more than 3 years after RS. The factors that are linked with failure are ill-known, but large tumor volume at the time of treatment, inadequate dose coverage, and cystic texture of the VS are predictive of poor tumor control. In Fig. 1 we show a flowchart of our own contemporary management of these patterns of growth.
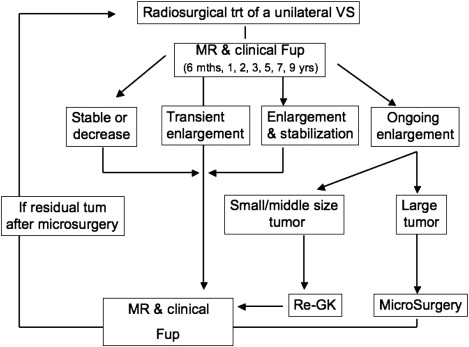
When a true failure is confirmed, it can be decided to operate or to retreat the tumor with RS, depending on the tumor size and clinical tolerance. When surgery is chosen, the surgeon may expect to observe some degree of arachnoid thickening. Modification of the vascularity and tumor texture is usually noted, and there is probably more adhesion with the brainstem and acousticofacial bundle. However, there is no scientific evidence that this surgery is systematically more difficult than in previously nonirradiated patients. To minimize the risk of facial nerve injury, it may be preferable to leave a small piece of tumor capsule along the facial nerve in case of excessive adherence. To avoid microsurgery (MS), the other option (see Fig. 1 ) is to propose a second procedure of RS if tumor size is still compatible with such treatment. In a recent series, such strategy was published by the Marseille team, whereby the results of additional Gamma knife RS (GKRS) in a series of 8 patients followed more than 2 years were reported. No failure was observed, and significant decrease of tumor size was shown in 6 patients, without any additional morbidity.
Radio-induced cranial nerve neuropathies
Due to various mechanisms, the cranial nerves that run in the close vicinity of the tumor may malfunction after radiosurgery (see Table 1 ). High doses delivered at the tumor margin and inadequate dose planning are clearly identified as risk factors. Considering the technical refinements of the machines and the accumulated expertise of the radiosurgeons/radiation oncologists, rates of cranial nerve neuropathies (CNNs) have dramatically decreased. However, there is still a risk of new deficit or worsening of a pre-existing deficit in the 2 years that follow RS. Their management is a matter of controversy. A short course of steroid therapy can be proposed if the hypothesis of edema is suggested. Above all, it is recommended to check the MRI to make sure that there is no local complications in the field of irradiation (eg, tumor volume modification, brainstem edema).
Facial Nerve Deficit
Facial palsy is a major concern after the treatmentof VS Thankfully, this is a very rare complication in the modern series. In the series from Sheffield, the rate of facial nerve deficit involved 4.5% of patients with less than 1% of permanent deficits. In Marseille, rates of less than 0.5% of facial palsy and 8% of hemifacial spasm were mentioned. Yang and colleagues provided a metanalysis that studied 2204 patients extracted from 23 series of GKRS for VS The overall facial nerve preservation rate (House & Brackmann grades 1–2) was 96.2%. Higher risk was found in elderly patients (older than age 60 years), high dose (<13 Gys), and tumor volumes superior to 1.5 cc.
Another issue, which is usually not reported in the main series, is the assessment of the intermedius nerve (Wrisberg nerve). As reported by the Marseille team, a careful analysis of lacrimation and taste before and after RS found a deterioration (ocular problems, taste disturbance) after the treatment in 14% of cases despite excellent facial nerve motility.
Hearing Loss
The known influencing parameters are: (1) tumor size, (2) hearing level (Gardner-Robertson class), (3) auditory brainstem response, (4) delivered dose at the tumor margin, and (5) dose delivered to the cochlea. The authors also showed that young age and presentation with tinnitus were predictive of hearing preservation.
Early hearing loss within 1 week may be related to direct neural radiation injury or edema, whereas delayed hearing loss may be related to vascular effects. A slow deterioration of hearing over a period of months, as observed after RS, has been considered to be preferable to the sudden deafness that occurs after microsurgical excision.
The hypothesis is that with lower marginal doses and longer follow-up, hearing loss may continue through a number of mechanisms, including direct radiation effects, vascular effects, and changes in the tumor remnant.
Taken together, the main series of the literature of GKRS indicate a loss of serviceable hearing in 30% to 50% of cases in the 2 years following treatment. This result has to be compared with the risk of spontaneous deafness in the natural course of the disease and with the potential of hearing deterioration after MS.
Vertigo, Tinnitus, Imbalance
Sughrue and colleagues made an extensive metanalysis of 63 articles reporting the results of 5631 patients treated for VS smaller than 25 mm in their largest diameter. They distinguished 2 cohorts of patients according to the marginal dose of radiation delivered:
- 1.
Lower dose cohort: less than 13 Gy for 3248 patients/58%
- 2.
Higher dose cohort: greater than 13 Gy for 2383 patients/42%
They found that 84 out of 5631 patients (1.5%) experienced vertigo or balance disturbance after their treatment. Surprisingly, they found in the lower dose cohort:
- •
An increased rate of vertigo and imbalance: 1.1% for less than 13 Gy versus 1.8% for greater than 13 Gy, P = .001
- •
An increased rate of tinnitus: 1.7% for less than 13 Gy versus 0.1% for greater than 13 Gy, P = .001
To explain this paradoxic phenomenon, the hypothesis is that patients treated with higher doses have more complete dysfunction of this nerve before treatment, while those treated with lower doses have enough function left to detect vertigo and tinnitus. In separate series, occurrence of tinnitus was described in 6% to 25% of patients after RS. It is of paramount importance to inform patients before treatment that RS will not provide better results than MS for these symptoms.
Nonaudiofacial Cranial Nerve Neuropathy
Trigeminal neuropathy (facial numbness) was defined as any temporary or permanent, subjective or objective decrease in facial sensation, or new pain within the ipsilateral trigeminal nerve distribution after radiosurgery.
Sughrue and colleagues reported that:
- •
Incidence of new trigeminal neuropathy was 2.3% and significantly increased with higher doses (3.15% for patients treated with doses >13 Gy and 1.63% for doses <13 Gy: P <0.001)
- •
Risk of VI nerve palsy was 0.03% (0.08% for doses >13 Gy and 0% for doses <13 Gy).
- •
Risk of XII nerve neuropathy was 0.08% overall (0.15% for doses <13 Gy, 0% for doses >13 Gy).
- •
Onset of the deficit occurred at 6 to 24 months after RS.
Ogunrinde and colleagues reported a 6% rate of delayed sensory trigeminal nerve dysfunction. Onset of new trigeminal dysfunction occurred at 11 and 22 months. At last follow-up, no patient in this series developed any deafferentation pain.
Rowe and colleagues published a rate of persistent trigeminal neuropathy of about 1.5%. Chopra and colleagues indicated that at 10 years, 95% of patients were free of trigeminal nerve problems.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


