Tracheal neoplasms are rare, accounting for only 1% of all malignancies (1), but the impact on the individual is generally severe (2,3,4). With regard to incidence, these tumors may also be underreported, incompletely diagnosed, and undertreated because of the rarity, lack of mandatory registration, limited surgical experience, and the relative sporadic nature of the lesions (4). The most common tumors are classified as benign, primary malignant and secondary malignant in Table 126.1. Because these tumors occupy the main airway conduit, as they enlarge, the impact and potential fatality increase. Stridor, hemoptysis, and shortness of air are the most common symptoms, and many patients present in need of acute airway management. Injudicious airway management may precipitate airway obstruction and/or potentially interfere with subsequent definitive surgical management (4,5).
CLINICAL PRESENTATION
History
Tracheal tumors tend to cause progressive symptoms over several months to years due to their slow-growing nature often causing accurate diagnosis to be delayed (6). Gaissert et al. (7) reviewed 270 cases of squamous cell and adenoid cystic carcinoma of the trachea and carina, and the mean duration of symptoms was 12.2 months. The duration of symptoms was longer in adenoid cystic carcinoma and in tumors that were deemed to be unresectable (resected adenoid cystic carcinoma 18.3 months, resected squamous cell carcinoma 4.54 months, unresectable adenoid cystic carcinoma 23.7 months, unresectable squamous cell carcinoma 7.58 months, P < 0.0001) (6).
Symptoms at presentation depend largely on extent of airway obstruction and tumor type, but not location within the tracheobronchial tree (8). Dyspnea with exertion or phonation is the primary symptom when the tumor has caused significant airway obstruction. If lesions are ulcerative and mucosal irritation is severe, chronic cough and hemoptysis are common. Wheezing, stridor, hoarseness, difficulty clearing secretions, and frequent respiratory infections are also encountered.
Presentation may vary with tumor type with hemoptysis being the main symptom in patients with squamous cell carcinoma, and wheezing and dyspnea predominate in those with adenoid cystic carcinoma (Table 126.2) (9). Wheezing is often misdiagnosed as “asthma” and is refractory to bronchodilator therapy. Prolonged use of systemic corticosteroids is common, and patients may even be secondarily cushingoid at presentation (10).
Imaging
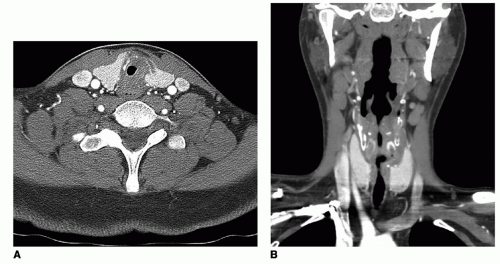
Imaging studies that are most frequently employed are CT scan with contrast and in some instances PET-CT. CT with contrast allows for adequate multiplanar imaging of the airway from hyoid to segmental bronchi. CT can be further exploited to derive three-dimensional images allowing for “virtual endoscopy.” It is useful in the identification of involvement of mediastinal soft tissues, esophagus, and vasculature. It is additionally helpful in demonstrating coexisting pulmonary metastatic disease. PET-CT may be useful in distinguishing more aggressive pathology and may be more sensitive in the detection of paratracheal and mediastinal nodal involvement. MRI scanning may be useful in the examination of the cervical trachea, but mediastinal and thoracic structures may be significantly be distorted by motion artifact due to respiratory and circulatory movement (11,12,13). Figure 126.1A and B represent a demonstration of a high tracheal adenoid cystic carcinoma in both the axial and coronal planes.
TABLE 126.1 PATHOLOGY OF TRACHEAL TUMORS
Primary Tumor
Tumor Type
Epithelial (benign)
Papilloma
Adenoma
Myoepithelial tumor
Pleomorphic adenoma
Oncocytoma
Epithelial (malignant)
Squamous cell carcinoma
Adenoid cystic carcinoma
Adenocarcinoma
Mucoepidermoid carcinoma
Large cell undifferentiated carcinoma
Carcinoma ex-pleomorphic adenoma
Neuroendocrine tumors:
Typical and atypical carcinoids
Large cell neuroendocrine tumor
Small cell carcinoma
Mesenchymal (benign)
Lipoma
Neurofibroma
Fibroma
Pyogenic granuloma
Plexiform neurofibroma
Benign fibrous histiocytoma
Hemangioma
Hemangiopericytoma
Chondroma
Leiomyoma
Chondroblastoma
Granular cell tumor
Plasmacytoma
Paraganglioma
Schwannoma
Glomus tumor
Mesenchymal (malignant)
Chondrosarcoma
Malignant melanoma
Malignant lymphoma
Leiomyosarcoma
Spindle cell sarcoma
Malignant fibrous histiocytoma
Carcinosarcoma
Rhabdomyosarcoma
Secondary Tumor
Tumor Type
Local invasion
Thyroid carcinoma
Lung carcinoma
Esophageal carcinoma
Metastatic
Renal cell carcinoma
Colon carcinoma
Breast carcinoma
Metastatic melanoma
INITIAL AIRWAY MANAGEMENT
For tracheal tumors, bronchoscopy is the mainstay of initial airway management and diagnosis. If the airway is stable at presentation, elective bronchoscopy can be arranged. However, in patients with acute airway compromise, urgent bronchoscopy may be needed to stabilize the airway. Bronchoscopy allows accurate estimation of the extent of airway pathology and airway obstruction. The exact tumor location, length of tracheal involvement, and its proximity to key anatomical structures can be determined. Tissue diagnosis is obtained during initial bronchoscopy, and margin mapping can be performed to help with treatment planning. For proximal tracheal tumors, rigid bronchoscopy is preferred over flexible bronchoscopy due to its ability to ventilate during the evaluation. Flexible bronchoscopy can provide additional information concerning the more distal airways.
TABLE 126.2 PRESENTING SYMPTOMS IN 270 PATIENTS WITH PRIMARY TRACHEAL CARCINOMA
Symptoms (%)
Adenoid Cystic
Squamous Cell
Dyspnea
65
50
Cough
55
52
Hemoptysis
29
60
Wheeze
44
27
Stridor
21
27
Hoarseness
10
13
Dysphagia
7
7
Fever
7
4
Other
12
14
Gaissert HA, Grillo H, Mathisen D, et al. Long-term survival after resection of primary adenoid cystic and squamous cell carcinoma of the trachea and carina. Ann Thorac Surg 2004;78:1889-1897.
Patients are sometimes able to tolerate significant obstruction (75% or more), but can decompensate rapidly with increased secretions or inflammation. In the event of an urgent airway, endotracheal intubation may not be feasible and could cause tumor dislodgement with subsequent complete airway obstruction. In this setting, rigid bronchoscopy can help stabilize the airway by dilating the stenotic segment, and tumor debulking can be performed. Flexible bronchoscopy alone can be dangerous, potentially causing edema and bleeding, which can precipitate complete airway obstruction. A rigid bronchoscope has the ability to tamponade bleeding while bypassing the site of obstruction for ventilation.
Emergency intervention via a surgical airway could prove troublesome depending on tumor location. Injudicious tracheotomy may transgress a lesion or make subsequent tracheal resection and reconstruction more difficult. If tracheotomy can be safely accomplished distal to the lesion, it may be warranted if the tumor is unresectable or patient comorbidities preclude definitive surgical management.
Finally, in addition to stabilizing the airway, therapeutic bronchoscopy can prepare and optimize a patient for airway surgery (14). Inflammation adjacent to the lesion may represent malignant submucosal extension or benign reactive changes. By delaying the resection and palliating the airway through repeated bronchoscopic intervention, obstructive pneumonia with resulting airway inflammation can be resolved. This allows for better delineation of margins and may decrease perioperative complications such as wound disruption and pneumonia (14).
Figure 126.1 A,B: Adenoid cystic carcinoma. Contrast-enhanced axial CT showing a mass involving the lateral and posterior aspect of the proximal trachea. Adenoid cystic carcinoma. Coronal CT shows a submucosal lesion similar in appearance to tracheal stenosis.
DEFINITIVE SURGICAL MANAGEMENT
Tracheal Resection
Tracheal resection and primary reanastamosis is the preferred treatment for the majority of both benign and malignant tracheal neoplasms. The ability to perform this preferred management is predicated upon patient-, tumor-, and surgeon-related factors. Patient factors that are important include body habitus, medical comorbidities, and patient preference. Increasing body mass index (BMI) and a thick and short neck may be impediments to the execution of tracheal resection and reanastamosis. In this patient group, the mobilization of the trachea inferiorly and superiorly may be limited, and access to the segment of trachea containing the tumor may not be able to be accomplished solely through a cervical approach. Patients with coexisting chronic obstructive pulmonary disease may require a longer intubation and may be more prone to coughing exacerbations that may place additional strain on the tracheal repair. Furthermore, patients who have diabetes mellitus or are otherwise immunocompromised may have poorer wound healing, especially with longer segment resections that are under tension.
Tumor factors are important in decision making. The length of the proposed segment that would require resection for adequate margins represents one of the key factors in determination of treatment. Segmental resections of greater than 4 cm or six tracheal rings represent conditions in which the tracheal repair is under increased tension and dehiscence may be more likely. Submucosal, esophageal, mediastinal, and extensive tracheal or bronchial extension may require combined cervicothoracic procedures or nonsurgical treatment. A variety of extended tracheobronchial resections have been described and are best managed in a multidisciplinary approach with otolaryngologist and thoracic surgeon. Premature tracheotomy in the securing of an airway may create additional scar tissue and potential seeding of the soft tissues of the neck and make subsequent surgical resection efforts more difficult. Prior radiation therapy may additionally have an impact on the ability to dissect soft tissues, mobilize the trachea and larynx, identify critical structures, and allow for optimal wound healing.
Surgeon preference and experience may influence approach. Experience with benign tracheal stenosis, laryngectomy, and tracheal resection increases the confidence and ability of the surgeon to manage these lesions. Cooperation between otolaryngologists and thoracic surgeons allows for improved patient selection, procedure selection, and technical execution of these complicated cases (2,3,4,5,15). Contraindications for tracheal resection are relative rather than absolute in many cases. Because airway patency represents a fundamental goal in the management of patients with tracheal neoplasms, resection may be offered even in the face of primary tracheal tumors with regional or distant metastatic disease as well as selected metastatic lesions to the trachea. Lesions that are involve greater than 4 cm or are greater than six tracheal rings may not be eligible for resection; factors ultimately affecting this decision include body habitus, ability to adequately mobilize the upper respiratory tract, and experience of the surgical team in both the procedure and management of its complications. Extensive extratracheal disease in the mediastinum involving the esophagus, mediastinal vessels, and prevertebral spaces represents cases in which resection is contraindicated and tracheotomy, endoscopic tumor ablation, and stent placement may be preferred.
Standard resection steps are predicated upon adequate bronchoscopic evaluation of the airway, imaging of the trachea and related neck and mediastinal structures, pathological confirmation, surgical team selection and approach, anesthetic preparation and management plan, and finally execution of the procedure. The steps of the tracheal resection procedure are as follows: transverse cervical incision outlined in cervical crease at midpoint between the sternal notch and the inferior border of the cricoid cartilage that are readily palpable landmarks. In extended cases or in cases in which cervical and extensive mediastinal dissection or proximity to the innominate artery is anticipated, both the neck and chest should be sterilely prepped and draped. The transverse cervical incision can be readily connected to a vertical chest incision for addition of a median sternotomy (total or partial). After preparation and skin incision choices are made, the steps of tracheal resection with primary repair are as follows:
Elevation of a subfascial, supramuscular flap above the strap musculature and the sternomastoid muscles sternal heads both superiorly and inferiorly into the suprasternal space of Burns.
Separation of the strap muscles from the thyroid cartilage to the sternal and clavicular origins of the muscles. Retraction of the wound may be done with a variety of self-retaining retractors, elastic stays, or sutures.
Exposure of the trachea requires the surgeon to anticipate extratracheal extension. For example, thyroidectomy may be required if resection is being performed because of well-differentiated thyroid cancer with focal tracheal invasion. In cases of endoluminal primary tracheal neoplasms, the thyroid isthmus should be divided with careful hemostasis, and the thyroid lobes mobilized laterally.
Recurrent (inferior) laryngeal nerve identification is not performed routinely, although identification of the nerve may be required for adjunctive procedures such as thyroidectomy, central lymphadenectomy, or extended cricotracheal procedures. Monitoring of the recurrent nerves may be helpful in maintaining integrity of the nerves and monitoring the condition of the nerve during retraction; there is no current evidence that use of neural monitoring improves recurrent laryngeal nerve outcome in these procedures.
Tracheal mobilization. The trachea should be carefully mobilized from the cricoid to two to three rings below the intended inferior margin of resection. Concomitant use and measuring of the lesion with imaging studies and intraoperative bronchoscopy may add accuracy to the determination of the segment requiring resection. Mobilization of the resection segment must be circumferential. Beyond the resection segment inferiorly, care should be taken to perform anterior and posterior mobilization, but careful lateral preservation of soft tissues in order to preserve the blood supply to the distal trachea from the inferior thyroid artery and other thyrocervical trunk arterial tributaries.
Only gold members can continue reading. Log In or Register to continue