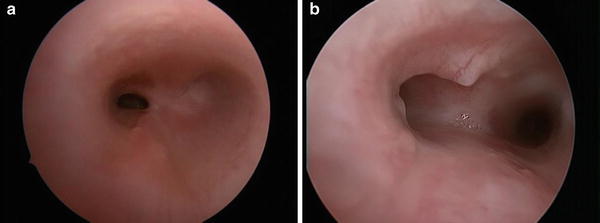
Fig. 1
Endoscopic views of a child with long-segment complete tracheal rings. (a) View showing beginning of rings; (b) view showing mid-section of rings; (c) view showing distal segment of rings
Diagnostic Workup
The initial evaluation should include plain airway films, as these may indicate that congenital tracheal narrowing is present. Although imaging studies may be very useful, bronchoscopic evaluation remains the gold standard for definitive assessment. This should be performed with extreme care, as instrumentation in an area of stenosis may cause enough swelling to convert a narrow airway to a critical airway, necessitating abrupt intervention. If the smallest bronchoscope available (whether rigid or flexible), cannot be easily passed through the area of stenosis, it is better to identify the proximal extent of the stenosis without fully evaluating the distal airway. Good communication with anesthesia colleagues is essential, and to facilitate the bronchoscopy, the child should be spontaneously breathing. We recommend the use of sevoflurane and propofol; steroid administration is also advisable. The trachea is then suctioned with a soft 6 Fr catheter and the patient is preoxygenated. Next, a further propofol bolus is delivered to temporarily halt respiratory efforts during the bronchoscopy.
Ideally, the aims of endoscopic evaluation are: to confirm the diagnosis of tracheal stenosis; establish whether this is due to CTRs; estimate the size of the smallest ring; estimate the percentage of the airway involved with CTRs as well as the position of the rings within the trachea; and evaluate the bronchial anatomy.
In patients with distal tracheal stenosis, an adequate evaluation cannot be made with a ventilating bronchoscope, as even the smallest ventilating bronchoscope is too large for most complete rings. The Hopkins rod telescope (removed from the bronchoscope) should thus be introduced into the airway to assess the stenosis. The initial bronchoscopic view is often sufficient to establish the diagnosis, thereby avoiding the risk of airway edema.
Estimating the size of the airway is valuable. In a normal full-term neonate, the narrowest point of the airway is at the cricoid, and this should measure 4.5–5.5 mm. Subglottic stenosis is defined as an airway diameter of <4.0 mm (by comparison, a 2.5 mm endotracheal tube has an outer diameter of 3.6 mm). Although the trachea should be of greater capacity than the cricoid, the airway in patients with CTRs may be too small to easily permit safe passage of any form of instrumentation. For comparative purposes, the smallest Storz 2.5 ventilating bronchoscope has an outer diameter (OD) of 3.7 mm. The smallest 20017 Hopkins rod telescope (as found in the Storz 2.5 ventilating bronchoscope) has an OD of 1.9 mm.
Because 50 % of children with CTRs have a tracheal inner diameter of approximately 2 mm at the time of diagnosis, the standard interventions for managing a compromised airway are not applicable. More specifically, the smallest endotracheal tube (2.0 mm inner diameter [ID]; 2.9 mm OD) and the smallest tracheotomy tube (2.5 mm ID; 3.9 mm OD) cannot pass through the stenotic segment without severe damage to mucosa or tracheal rupture. As the stenosis usually extends to the carina, bypassing the stenosis risks bronchial intubation. This may leave extracorporeal membrane oxygenation (ECMO) as the only viable alternative for stabilizing the child in the event of decompensation following bronchoscopy. In an effort to avoid ECMO in a child who is decompensating and poorly ventilating, intubation proximal to the complete rings is preferable. The endotracheal tube should be sized to the cricoid, with the Murphy eye just below vocal fold level. Given that it is unusual for the proximal two tracheal rings to be complete, shallow intubation is achievable in most children with CTRs. A nasal intubation to allow tube stabilization (as it is so shallow) is advisable. Ventilation requires a long inspiratory phase and an even longer expiratory phase to allow air to pass the stenosis. Higher than typical ventilator pressures may be tolerated, as the stenosis ensures that the lungs are not exposed to the same pressures as the subglottis. Maintenance of high humidity levels is crucial, as mucus accumulation may be lethal and is often heralded by rising CO2 rather than low oxygen saturation. In a crisis, 1 mL of 1:10,000 epinephrine delivered down the endotracheal tube may assist ventilation. If possible, extubation is desirable, as most children with CTRs maintain ventilation more effectively themselves than on a ventilator. To prevent mucus accumulation, saline may be regularly nebulized if required.
In view of the high proportion of patients with other congenital anomalies, a thorough diagnostic investigation should include a contrast-enhanced computed tomography (CT) scan of the chest with three-dimensional reconstruction, and an echocardiogram. These tests will identify any coexisting cardiovascular pathology, which should be repaired concurrently with the tracheal repair. As mentioned earlier in this chapter, our clinical experience indicates that a pulmonary artery sling is the most common cardiovascular anomaly; intracardiac anomalies and the presence of a persistent left superior vena cava draining to the coronary sinus, with absence of the innominate vein are, however, also frequently seen. Other anomalies may be incidental (e.g., limb or central nervous system anomalies) or also affect the airway. Nearly one third of children with CTRs have a tracheal (or pig) bronchus, and subglottic stenosis is present in approximately 20 % [6]. Rarely, CTRs may coexist with a tracheoesophageal fistula or laryngeal cleft. Pulmonary anomalies may also occur, with subsegmental branching patterns almost universally aberrant, though of limited significance. Pulmonary hypoplasia or agenesis, more commonly affecting the right lung, is more significant, as it may cause mediastinal shift and aortic compression of the already stenotic trachea.
Although most children with CTRs require early tracheal reconstruction, some (10–15 %) have sufficient tracheal growth to avoid the need for reconstruction. A further 10–15 % eventually outgrows their trachea and requires late repair. The recommended surgical technique is the slide tracheoplasty (discussed later in this chapter). This approach yields significantly better results than any other tracheal reconstruction technique and is applicable to all anatomic variants of CTRs [6, 7].
Most children with CTRs have distal tracheal involvement. If the distal one-third of the trachea is involved or if there are coexistent cardiovascular anomalies that require repair, we recommend repair utilizing cardiopulmonary bypass. More than 90 % of children requiring slide tracheoplasty for CTRs fall into this category. If only the upper or mid-trachea is involved, repair may be performed with routine anesthesia through a cervical approach. Hyperextension of an infant’s neck over a shoulder roll allows good access to the upper two thirds of the trachea through a cervical approach. Exposure can be further enhanced through a limited upper sternotomy if required.
Sleeve Trachea
Albeit extremely rare, tracheal sleeve is the second most common condition falling within the general classification of problems involving the tracheal exoskeleton with stenosis. In infants with this condition, the trachea consists of a single sheet of cartilage rather than 15–20 separate tracheal rings; this cartilaginous sheet may extend proximally into the cricoid and distally into the bronchi. Sleeve trachea is universally associated with a craniosynostosis syndrome, with Pfeiffer, Crouzon, and Apert syndromes, represented in that order [8]. Nonetheless, only a small number of patients with craniosynostoses have a sleeve trachea, and even fewer have associated tracheal obstruction with the posterior aspects of the tracheal cartilage overlapping, effacing the trachealis muscle (Fig. 2). In these cases, a slide tracheoplasty is still an effective reconstructive option, although technically more challenging than a straightforward repair of CTRs. Of note, most children with sleeve trachea have multiple levels of airway obstruction from the choana to the bronchi. Although a slide tracheoplasty may therefore not prevent the need for a tracheotomy, in some children, it does, however, allow for the safe placement of a tracheotomy.

Fig. 2
Endoscopic view of sleeve trachea
Absent Tracheal Rings
Although compromised tracheal airflow in exoskeletal problems with stenosis usually results from abnormalities in cartilage structure, an infant may also present with stenosis or collapse resulting from an absence of cartilage [9].. This extremely rare condition generally presents in an otherwise normal child as an isolated segment of trachea (usually just proximal to the carina) that is missing cartilage in a two- to three-ring segment (Fig. 3a, b). Clinical presentation is similar to that in infants with complete tracheal rings; however, bronchoscopically the stenotic segment lacks cartilage and is therefore distensible. While most affected children are otherwise normal, we have seen associated congenital left vocal fold paralysis as well as esophageal atresia.