and Yi Ning J. Strube2
(1)
Wright Foundation for Pediatric Ophthalmology and Adult Strabismus Medical Center, Los Angeles, CA, USA
(2)
Queen’s University, Kingston, Ontario, Canada
Keywords
TorticollisNystagmusParks-Kestenbaum procedureFace turnIncomitant strabismus6.1 Torticollis: Compensatory Head Posturing
Torticollis comes from the Latin word torti, meaning twisted, and collis, meaning neck. Simply speaking, we can consider two types of torticollis: musculoskeletal and ocular. Musculoskeletal torticollis is caused by tight neck muscles (usually the sternocleidomastoid) or a skeletal deformity. With musculoskeletal torticollis, the neck will resist passive flexion with the eyes open or closed, and these patients maintain their head posturing even during sleep. In contrast, ocular torticollis is a compensatory mechanism to achieve optimal vision in patients with nystagmus or incomitant strabismus. A face turn or head tilt is adopted to place the eyes in a position that either reduces nystagmus or improves eye alignment. Ocular torticollis may be horizontal (face turn), vertical (chin up or down), torsional (head tilt right or left), or a combination of the three. The best way to identify the presence of a face turn or chin posturing is by looking at the position of the eyes. A gaze preference indicates a face turn. For example, does the patient in Fig. 6.1 have a face turn?

Fig. 6.1
Patient with a compensatory face turn
Answer
Yes! This patient has a compensatory face turn to the left, to keep the eyes in right gaze. This right gaze preference could be the result of nystagmus with a null point in right gaze or an incomitant strabismus with orthotropia in right gaze. The key to assessing a compensatory face turn is to observe the position of the eyes. If the eyes remain in an eccentric gaze, then the face is turned.
6.1.1 Strabismic Torticollis
Incomitant strabismus means the eyes are not moving in synchrony. The cause can be ocular restriction, extraocular muscle paresis, extraocular muscle overaction, or A and V patterns. Patients with incomitant strabismus may adopt a face turn, a chin posture, or a head tilt to place the eyes in a position of alignment and achieve binocular fusion. For example, patients with a right congenital fourth nerve paresis will tilt their head to the left to reduce the hypertropia and maintain binocular fusion. Incomitant horizontal strabismus can cause a face turn. A tight medial rectus (MR) muscle in the right eye will produce an esotropia in right gaze and provoke a face turn to the right to keep the eyes aligned in left gaze.
The strategy for correcting a face turn caused by an incomitant strabismus is to correct the strabismus in primary position, and to increase the field of binocular fusion by improving the incomitance. If the ductions are relatively full, surgery can be done on either eye or both eyes to correct the incomitance. If there is only minimal limitation, it is often best to match the limitation by operating on the “good eye.” In cases with significant limitation of movement of one eye (restriction or muscle palsy), correct the face turn by moving the eye with limited ductions into primary position. It does not help to operate on the normal eye if the eye with limited ductions cannot move easily to the primary position. Below are examples for the treatment of incomitant strabismus causing a compensatory head posture.
Example 6.1. Strabismus, Face Turn with Full Ductions
The patient in Fig. 6.2 has a right partial sixth nerve paresis, good lateral rectus (LR) function, and full ductions.
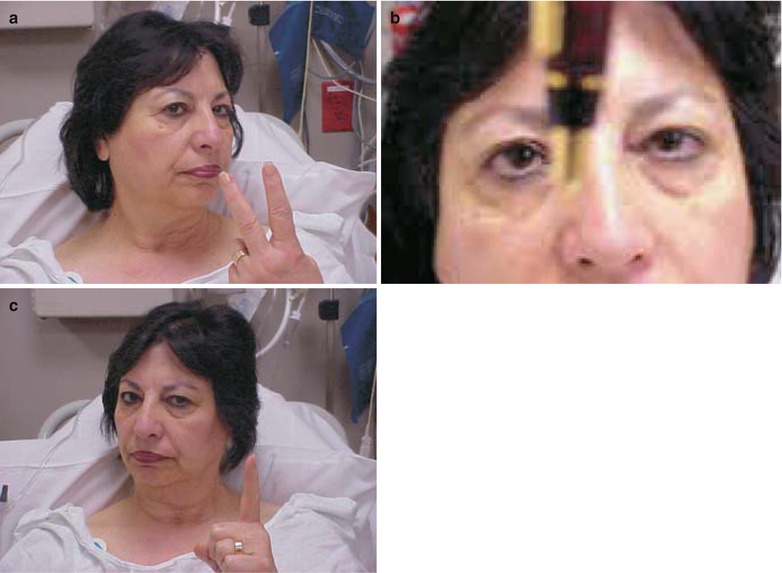
Fig. 6.2
Patient with a right partial sixth nerve paresis and good lateral rectus function. (a) The patient has an esotropia and diplopia in right gaze. (b) Esotropia in primary position. (c) Because the esotropia increases in right gaze the patient maintains a compensatory face turn to the right to keep the eyes aligned in left gaze and achieve single vision
Preoperative deviation:
Right gaze | Primary position | Left gaze |
|---|---|---|
ET 25PD | ET 15PD | E 2PD fusing |
Following are two treatment options to correct this strabismus and face turn:
Option 1. Operate on the paretic eye
Surgery: Right MR recession and right LR resection
Right gaze | Primary position | Left gaze | |
|---|---|---|---|
Result: | ET 10 PD | Orthotropia | XT 12 PD |
Option 2. Asymmetric bilateral surgery: Operate on the good eye
Surgery: Right MR recession 3 mm and left MR recession 6 mm
Right gaze | Primary position | Left gaze | |
|---|---|---|---|
Result: | E2 PD | Orthotropia | X2 PD |
In this case, the right lateral rectus is underacting, so the left MR is overacting (Hering’s law), producing an esotropia greater in right gaze. In Option 1, recessing the medial rectus and resecting the lateral rectus of the right eye does not improve abduction but limits adduction (see Chap. 2). Limiting adduction in the right eye induces an exotropia in left gaze and undercorrects the esotropia in right gaze. Option 2 is a better choice to provide the largest area of binocular single vision. A large left medial rectus recession reduces adduction slightly, and that matches the slight abduction deficit of the right eye. This strategy of matching the function of yoke muscles (Hering’s law) can be used in a wide range of incomitant strabismus cases, as long as the ductions are full or only slightly limited. Another aspect is that the left medial rectus recession has most of its effect in right gaze, where the esodeviation is greatest. (See Chap. 2 for surgical correction of incomitant strabismus.)
Example 6.2. Strabismus, Face Turn with Limited Ductions
If the face turn is due to limited ductions of one eye and the eye is fixed in an eccentric position of gaze, simply move the eye with limited ductions into primary position. In the case in Fig. 6.3, the left eye is in a position of rest in abduction because the left medial rectus muscle has slipped from previous strabismus surgery (elsewhere of course). The treatment is to advance the left medial rectus muscle and recess the tight lateral rectus muscle to move the left eye into primary position. Once adduction of the left eye has improved, then consider surgery on the right eye (LR recession) to correct the anticipated residual exotropia in right gaze. Surgery on the good eye to reduce the overshoot (Hering’s law) can be done primarily with the first surgery or as a secondary procedure.




