Topography, Bones, Vessels, Sensory Nerves
1 The ocular globes reside in two symmetrical bony cavities called the orbits.
2 Nerves and vessels enter the orbit, and their course and distribution must be understood. The aerated sinuses as well as the anterior and middle cranial fossae are intimately related to the orbital walls. The first edition, Surgical Anatomy of the Orbit, focused on this orbit and its contents, but very little on the neighboring areas. This edition expands widely, leaving the orbital confines to expose structures around it. Some basics are still required, so this initial chapter was rewritten to present an updated compendium of the essential data.
3 In this portion, you will learn certain orbital distances and relationships that you, the surgeon, will need to commit to memory. For that reason, some key numbers may be repeated.
Notes to the reader: Throughout this book, all dissections use the right orbit. Labels are kept to a minimum so as not to distract the reader; perusing the legends will allow the pictures to really tell the story. This approximates “truth” where labels do not exist.
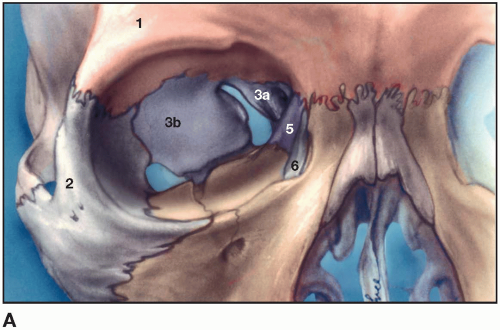 Figure 1.1A Bony components of the right orbit 1. Frontal bone (orange) 2. Zygoma (light gray) 3. Sphenoid bone (purple) 3a. Lesser wing 3b. Greater wing Maxilla (tan) Ethmoid bone (purple – 5) Lacrimal bone (6) Palatine bone (no. 4 below) |
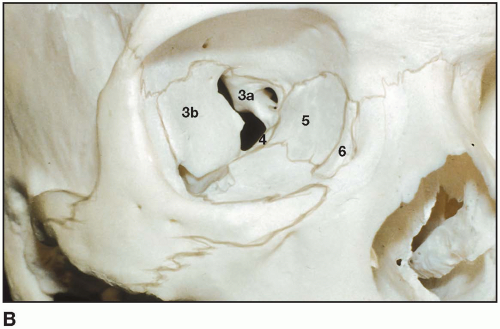 Figure 1.1B Dried skull with bony borders accented 3a. Lesser wing of sphenoid 3b. Greater wing sphenoid 4. Palatine bone 5. Ethmoid bone 6. Lacrimal bone |
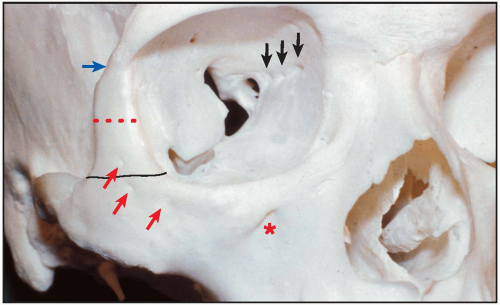 Figure 1.2 Anatomic points 1. The infraorbital foramen(*) opens downward and medially. 2. Red arrows point to exits of zygomaticofacial sensory nerve branches which supply the malar eminence and below. 3. The width of the lateral orbital rim inferior line is 1.3 to 1.5 cm. 4. The width of the lateral orbital rim at canthal level is 1.0 to 1.1 cm (dotted), and thinner as it approaches zygomatico-frontal suture (blue arrow). 5. Intraorbital arrows: Anterior and posterior ethmoidal foramina separate frontal bone above from ethmoid bone below it at the frontoethmoidal suture. The anterior foramen is 20 mm behind the anterior orbital margin, and the posterior is 12 mm behind this. The ophthalmic artery gives off the posterior ethmoidal arteries for the posterior ethmoidal air cells, anterior cranial fossa dura, and upper nasal mucosa. The anterior ethmoidal artery enters the anterior cranial fossa, and then via the cribriform plate into the nose. The anterior ethmoidal nerve, a sensory branch of the nasociliary, supplies anterior ethmoidal air cells, mucosa of the upper nose, and then exists as the dorsal nasal nerve (responsible for herpes zoster of the nasal tip). |
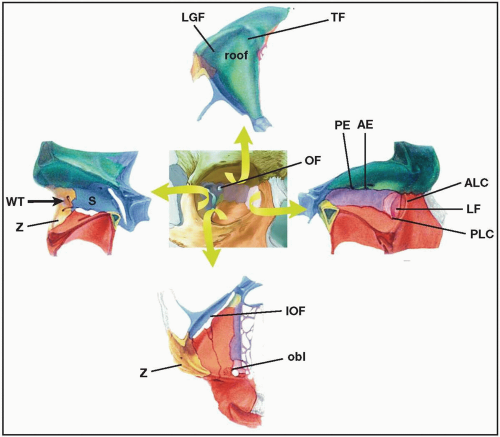
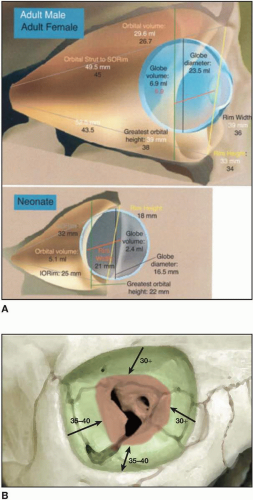 Figures 1.4(A-B) Volumes and distances: Males/females and babies In theory, everything outside the annulus (Fig. 1.4A) and superior orbital fissure is safe. As the surgeon realizes the distance to the optic foramen is approximately 50 mm (men) and 45 mm (women) and gives at least 1 cm margin, the surgeon may dissect 35 to 40 mm back on the floor and roof region. Lateral dissection may even go a bit farther back.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|