71 Tonsils and Adenoids • Lymphoid tissue encircling the pharynx • Consists of palatine tonsils (the tonsils), pharyngeal tonsils (the adenoids), lingual tonsils, and tubal tonsils • Constantly exposed to new antigens • Part of the MALT, which processes antigens and presents them to TH cells and B cells • Secretes IgA and IgG • Boundaries: • Vascular supply: • Venous drainage: • Nerve supply: • Lymphatic drainage: • Boundaries: • Vascular supply: • Venous drainage: • Nerve supply: • Lymphatic drainage: • Tonsils: lymphoid tissue covered with nonkeratinizing stratified squamous epithelium • Adenoids: lymphoid tissue covered with pseudostratified ciliated columnar epithelium • Only the tonsils lie in a capsule, this is formed from a specialized condensation of pharyngobasilar fascia • Viral tonsillitis: adenovirus, rhinovirus, reovirus, RSV, influenza, parainfluenza, CMV • Bacterial tonsillitis is usually due to group A β-haemolytic streptococcus (GABHS) but may also be due to staphylococcus, nonhaemolytic streptococci, Lactobacillus, Bacteroides, and Actinomyces • Other forms of tonsillitis include fungal tonsillitis (due to candidiasis, usually in immunocompromised patients), mycoplasmal tonsillitis, parasitic tonsillitis (toxoplasma), and tonsillitis due to chlamydia • Rare forms of tonsillitis include Vincent angina, caused by Treponema vincentii and Spirochaeta denticulata • Acute parenchymatous: the whole tonsil is infected but no exudative pus • Acute follicular: the crypts are filled with infected fibrin • Chronic forms: chronic parenchymatous and chronic follicular; these are sometimes associated with tonsillolith formation • Suppurative • Nonsuppurative • Infectious mononucleosis • Usually due to EBV, 10% of cases due to CMV • Transmitted by oral contact • Fever, generalized malaise, lymphadenopathy, hepatosplenomegaly, and pharyngitis • 10% become jaundiced • Blood count: lymphocytosis with atypical lymphocytes (activated T cells) • Sheep RBC agglutination in the presence of heterophile antibodies is the basis for the Paul–Bunnell test • Horse RBC agglutination in the presence of heterophile antibodies is the basis for the Monospot test • Airway obstruction • Myocarditis • Splenic rupture • Haemolytic anaemia • Acute interstitial nephritis, glomerulonephritis • Fatigue, depression • Neurological: optic neuritis, transverse myelitis, aseptic meningitis, encephalitis, meningoencephalitis, CN palsy or Guillain–Barré syndrome • Maculopapular rash develops with amoxicillin • Patients to avoid strenuous exercise for the first 3 weeks of illness • Prevent spread by avoiding close contact with body fluid secretions • Due to adenotonsillar hypertrophy • Association between OSAS and households where adults smoke • Complications: pulmonary hypertension, cor pulmonale, alveolar hypoventilation causing chronic CO2 retention • May result in craniofacial abnormalities over time • Benign: lipomas, fibromas, schwannomas • Malignant: lymphoma, SCC • Not a true neoplasm • Life-threatening complication of immunosuppression • Proliferative B-cell disorder associated with EBV in an immunocompromised host • Tonsillectomy is required to restore an airway and to provide tissue for diagnosis • Adenoiditis • OSAS as a consequence of their hypertrophy in conjunction with enlarged tonsils • Nasal obstruction • Contribution to recurrent or persistent otitis media • Contribution to recurrent acute sinusitis or chronic sinusitis • Enlarged tonsils resulting in upper airway obstruction/OSAS • Recurrent acute tonsillitis • Tonsillectomy to provide tissue for diagnosis – Swallowing difficulties – Tonsillar crypt debris (tonsilloliths) – Enlarged cervical LNs – Guttate psoriasis • See Fig. 71.1 • Bleeding diathesis • Anaemia • Acute infection • Poor anaesthetic candidate • Cold steel dissection • Diathermy • Laser—CO2, KTP, diode • Coblation • Radiofrequency • Ultrasonic scalpel • Ligasure • Post-operative haemorrhage • Damage to teeth • UK National Tonsillectomy Audit: “hot techniques” associated with 3-fold risk in post-operative haemorrhage • Enlargement resulting in upper airway obstruction • Recurrent or persistent otitis media • Recurrent acute sinusitis or chronic sinusitis • Dysphagia with failure to thrive • Significant speech problems • Bleeding diathesis • Risk of velopharyngeal insufficiency (VPI), especially in patients with short palate, submucous cleft palate (be suspicious if bifid uvula present), true cleft palate, palatal hypotonia • Risk of atlantoaxial joint laxity, especially in patients with Down syndrome (observed in 10% of patients) • Curettage • Suction diathermy • Microdebrider • Post-operative haemorrhage • Damage to teeth • VPI • Atlantoaxial subluxation in certain patients • Nasopharyngeal stenosis • Eustachian tube injury
71.1 Anatomy
71.1.1 Waldeyer Ring
71.1.2 Palatine Tonsils
 Anterior: palatoglossus
Anterior: palatoglossus
 Posterior: palatoglossus
Posterior: palatoglossus
 Lateral: superior constrictor
Lateral: superior constrictor
 Tonsillar a
Tonsillar a
 Ascending pharyngeal a
Ascending pharyngeal a
 Tonsil branch of facial a
Tonsil branch of facial a
 Dorsal lingual branch of lingual a
Dorsal lingual branch of lingual a
 Ascending palatine branches of facial a
Ascending palatine branches of facial a
 Peritonsillar plexus to lingual and pharyngeal vv to internal jugular v
Peritonsillar plexus to lingual and pharyngeal vv to internal jugular v
 Tonsillar branches of maxillary n and glossopharyngeal n
Tonsillar branches of maxillary n and glossopharyngeal n
 Directly to jugulodigastric nodes and upper deep cervical LNs and indirectly through retropharyngeal LNs
Directly to jugulodigastric nodes and upper deep cervical LNs and indirectly through retropharyngeal LNs
71.1.3 Adenoids
 Posterosuperior: posterior pharyngeal wall and base of skull
Posterosuperior: posterior pharyngeal wall and base of skull
 Ascending pharyngeal a
Ascending pharyngeal a
 Ascending palatine a
Ascending palatine a
 Tonsillar branch of facial a
Tonsillar branch of facial a
 Pharyngeal branch of maxillary a
Pharyngeal branch of maxillary a
 A of pterygoid canal
A of pterygoid canal
 Basisphenoid a
Basisphenoid a
 Peritonsillar plexus in conjunction with pterygoid plexus to internal jugular and facial vv
Peritonsillar plexus in conjunction with pterygoid plexus to internal jugular and facial vv
 Pharyngeal plexus
Pharyngeal plexus
 Retropharyngeal and pharyngomaxillary space LNs
Retropharyngeal and pharyngomaxillary space LNs
71.2 Histology
71.3 Tonsil Pathology
71.3.1 Tonsillitis
Types
Complications
 Peritonsillar abscess (quinsy)
Peritonsillar abscess (quinsy)
 Deep neck infections: parapharyngeal and retropharyngeal esses
Deep neck infections: parapharyngeal and retropharyngeal esses
 Thrombophlebitis: Lemierre disease (Fusobacterium necrophorum)
Thrombophlebitis: Lemierre disease (Fusobacterium necrophorum)
 Chronic adenotonsillar hypertrophy
Chronic adenotonsillar hypertrophy
 Scarlet fever
Scarlet fever
 Acute rheumatic fever
Acute rheumatic fever
 Poststreptococcal glomerulonephritis
Poststreptococcal glomerulonephritis
71.3.2 Glandular Fever
 This test is 100% specific and 85% sensitive, but more sensitive than the Paul–Bunnell test
This test is 100% specific and 85% sensitive, but more sensitive than the Paul–Bunnell test
 This test may be negative early in the course of EBV infectious mononucleosis
This test may be negative early in the course of EBV infectious mononucleosis
Complications
71.3.3 Obstructive Sleep Apnoea Syndrome
71.3.4 Neoplasms
71.3.5 Post-transplant Lymphoproliferative Disorder
71.4 Adenoid Pathology
71.5 Tonsillectomy
71.5.1 Indications
 7 or more episodes in the preceding year
7 or more episodes in the preceding year
 5 or more episodes in each of the 2 preceding years
5 or more episodes in each of the 2 preceding years
 3 or more episodes in each of the 3 preceding years
3 or more episodes in each of the 3 preceding years
 Other reported indications:
Other reported indications:
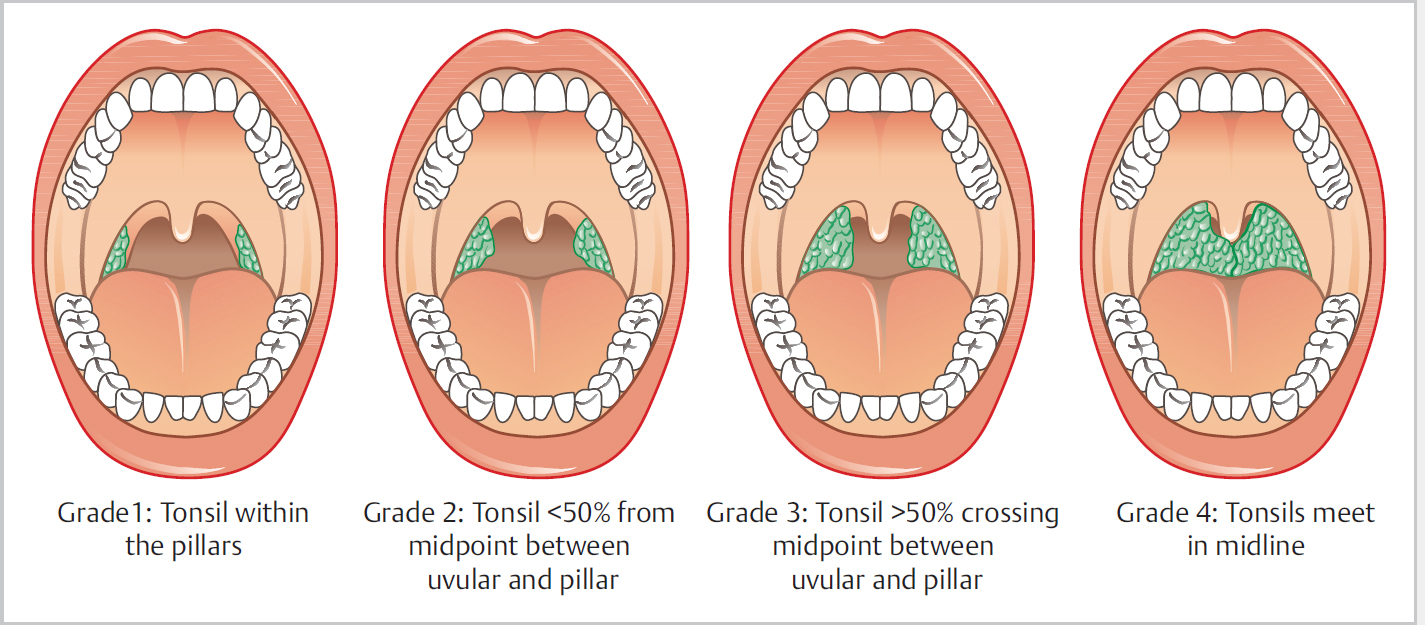
71.5.2 Brodsky Tonsil Classification
 Tonsil 0: Tonsils fit within the tonsillar fossa
Tonsil 0: Tonsils fit within the tonsillar fossa
 Tonsil 1+: Tonsils <25% of space between pillars
Tonsil 1+: Tonsils <25% of space between pillars
 Tonsil 2+: Tonsils <50% of space between pillars
Tonsil 2+: Tonsils <50% of space between pillars
 Tonsil 3+: Tonsils <75% of space between pillars
Tonsil 3+: Tonsils <75% of space between pillars
 Tonsil 4+: Tonsils >75% of space between pillars
Tonsil 4+: Tonsils >75% of space between pillars
71.5.3 Contraindications
71.5.4 Techniques
71.5.5 Complications
71.6 Adenoidectomy
71.6.1 Indications
71.6.2 Contraindications
71.6.3 Techniques
71.6.4 Complications
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


